Malnutrizione e Sarcopenia nel paziente con BPCO Prof

Malnutrizione e Sarcopenia nel paziente con BPCO Prof Mauro Zamboni Clinica Geriatrica Università di Verona
 40 Men 30 - 2.")
muscle mass and Aging 50 Women Muscle Mass (kg) 40 Men 30 - 2. 0 kg per decade in men - 1 kg per decade in women 20 10 0 15 25 35 45 55 Age (years) 65 75 85 Janssen et al. , J Appl Physiol 89: 81 -88, 2000

“Sarcopenia is a term that denotes the decline in muscle mass and strength that occurs with healthy aging. ” Rosenberg, Am J Clin Nutr 1989 “ Sarcopenia is part of normal aging and does not require a disease to occur, although it is accellerated by chronic diseases. ” Roubenoff et al, J Gerontol 2000

Skeletal Muscle Dysfunction in Chronic Obstructive Pulmonary Disease A Statement of the American Thoracic Society and European Respiratory Society American Journal of Respiratory and Critical Care Medicine, Vol. 159, Skeletal Muscle Dysfunction in Chronic Obstructive Pulmonary Disease 1999

Fat mass Body composition changes in COPD: 7 –years longitudinal data from the Health ABC Study Leg Fat Free mass 260 subjects with obstr lung dis (OLD) 157 smoking controls 866 formerly smokers 891 controls
/h (mt)2 Baumgartner et al,")
Operative definitions based on muscle mass index appendicular FFM (Kg)/h (mt)2 Baumgartner et al, 1998 total FFM (Kg)/body weight (kg) Janssen et al, 2002 Distribution in Young Adults Normal at Risk for Sarcopenia Severe Sarcopenia -2 SD -1 SD Mean Skeletal Muscle Mass
, disease severity (B), and Body mass index,")
Prevalence of sarcopenia according to age (A), disease severity (B), and Body mass index, obstruction, dyspnoea, exercise capacity index (i. BODE) (C). 622 outpatients with stable COPD Prevalence of sarcopenia was 14. 5% (11. 8% to 17. 4%), which increased with age and Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD) stage, but did not differ by gender Sarah E Jones et al. Thorax 2015; 70: 213 -218

Thigh muscle cross sectional area in COPD and control subjects Am J Respir Crit Care Med Vol 158. pp 629 -634, 1998

low body weight may induce over estimation of sarcopenia low muscle mass with high physical performance Defininition of sarcopenia just based on low muscle mass is likely sub-optimal

3 -year changes in muscle mass and strength in older adults declines (% / year) Loss of leg lean mass (hatched bar) and muscle strength (black bar) in older adults Results from the Health, ABC Study White men * Black men * White women * Black women * * Gender difference: p <. 01, Racial difference: p <. 05 Goodpaster et al. J Gerontol Med Sci, 2006, 61 (10), 10591064

muscle strenght in patients with COPD compared to normal subjects Am J Respir Crit Care Med Vol 158. pp 629 -634, 1998

Body composition changes in COPD: 7 –years longitudinal data from the Health ABC Study SPPB Leg Fat Free mass 260 subjects with obstr lung dis (OLD) 157 smoking controls 866 formerly smokers 891 controls
: 5 anni di follow-up Rossi")
Modificazione della composizione della coscia valutate con. TAC (n=1981): 5 anni di follow-up Rossi AP et al. J Geront 2011 Area del muscolo (cm 2) P<0. 001 Infiltrazione lipidica del muscolo (cm 2) P<0. 001

Miosteatosi e Miofibrosi riducono la qualità del muscolo miofibrosi miosteatosi Barbat-Artigas, Rolland Y, Zamboni M, Aubertin Leheudre J Nutr Health and Aging, 2012

Vastus lateralis biopsies of COPD weight-stable patients and healthy age matched controls * Fybrosis Increase in muscle fibrosis and fat infiltration is similar to that induced by age. Fat infiltration Eur Resp J 2003; 22: 280 -85

Inflammatory cells in limb muscles of patients with COPD leucocytes macrophages

Decrease in • cross-bridging between Fibers Effect of age on motor and muscle • number and size of Mithocondria • synthesis of myosin • type II fibers • motor unit Lang et al, Osteoporosis Int 21: 543 -559, 2010 (mod)

Vastus lateralis biopsies of COPD weight-stable patients and healthy age -matched controls Type 1 fibers (oxidative) Type IIX fibers (glycolitic) * * (atrophic) Muscle fiber shift is opposite to the shift induced by age. COPD Eur Resp J 2003; 22: 280 -85

Criteria for the diagnosis of sarcopenia Diagnosis is based on documentation of criterion 1 plus (criterion 2 or criterion 3). 1 - Low muscle mass 2 -Low muscle strength 3 - Low physical performance Age and Ageing, 2010

alterations in limb muscles in COPD patients

Sarcopenia categories by cause Primary sarcopenia Age No other cause evident except ageing Secondary sarcopenia Activity-related sarcopenia Disease-related sarcopenia Nutrition-related sarcopenia Bed rest, sedentary lifestyle, deconditioning or zerogravity conditions Associated with advanced organ failure (heart, lung, liver, kidney, brain), inflammatory disease, malignancy or endocrine disease Inadequate dietary intake of energy and/or protein, malabsorption, gastrointestinal disorders or use of medications that cause anorexia

high BMI may induce under-estimation of Sarcopenia high BMI and high FFM Mobility limitation Probably Sarcopenic high BMI and high FFM No mobility limitation No Sarcopenic

Mechanisms involved in age related Sarcopenia Moto-neuron loss Physical inactivity Bed rest Zero gravity age related hormones decline: ↓GH/IGF 1 ↓ Testosteron, DHEAS ↓ Estrogens ? ↓ Vitamin D sarcopenia ↑ Myostatin dysregulation of catabolic cytokines nutrition Oxidative damage
 loss by quintile of energyadjusted total protein intake. N= 2066")
Adjusted lean mass (LM) loss by quintile of energyadjusted total protein intake. N= 2066 Protein intake: from 0. 7 g/kg to 1. 2 g/kg Adjusted lean mass (LM) loss by quintile of energyadjusted total protein intake and weight change status. N= 2066 Low protein intake means higher risk of Sarcopenia Denise K Houston, 2008

Activity related Sarcopenia Effect of 10 days of bed rest in older adults Kortebein et al. JAMA 2007

Influence of Age and bed rest on Skeletal Muscle Mass 50 Women Muscle Mass (kg) 40 Men - 1. 5 kg per decade in men - 1 kg per decade in women 30 1. 5 kg per - 10 days bed-rest in old subjects - 30 days bed-rest in young subjects 20 10 0 15 25 35 45 55 Age (years) 65 75 85 Janssen et al. , J Appl Physiol 89: 81 -88, 2000

Mechanisms involved in Sarcopenia in COPD patients Moto-neuron loss Physical inactivity Bed rest Zero gravity Acute Exacerbations Smoking hormones decline: ↓GH/IGF 1 ↓ Testosteron, DHEAS ↓ Estrogens ? ↓ Vitamin D sarcopenia ↑ Myostatin dysregulation of catabolic cytokines Nutrition Oxidative damage Corticosteroids

Muscle proteins oxidation levels Oxidative stress is a contributor to COPD muscle dysfunction Oxidants contained in cigarette smoke induce oxidative modifications of key muscle biological structures and in particular of muscle proteins increasing proteolisis, decreasing proteosintesis, and reducing muscle growth

Quadriceps peak torque in patients with acute exacerbations and after 90 days of follow-up Decrease in quadriceps strenght by 5% after 5 days of hospitalization After 3 months only partial recovery

Mechanisms leading to muscle dysfunction in acute exacerbations

Steroid induced myopathy Proximal muscle weakness after long-term treatment with low doses of oral corticosteroids Atrophy of type II fibres (IIx) with less or no impact in type I fibres

Malnutrition risk and COPD

39 out-patient centers 389 patients with moderate to svere COPD Age 40 -75 years Black: BMI normal FFM depletion White: BMI depletion and normal FFM Dots : BMI and FFM depletion

sarcopenia malnutizione per difetto

Overlap Cachexia, Starvation and sarcopenia Malnutrizione Perdita di peso FM FFM Cachessia Perdita di peso FFM FM PCR > 10 mg/dl Sarcopenia No perdita di peso FFM FM stabile/aumentata Forza Perfornance fisica Modificata da: Thomas Clinical Nutrition 2007,

Definition Limb muscle dysfunction is defined as the morphological and functional changes that are seen in limb muscles in patients with COPD Limb muscle dysfunction is an important systemic consequence of COPD, because of its impact on physical activity, exercise tolerance, quality of life, and even survival.
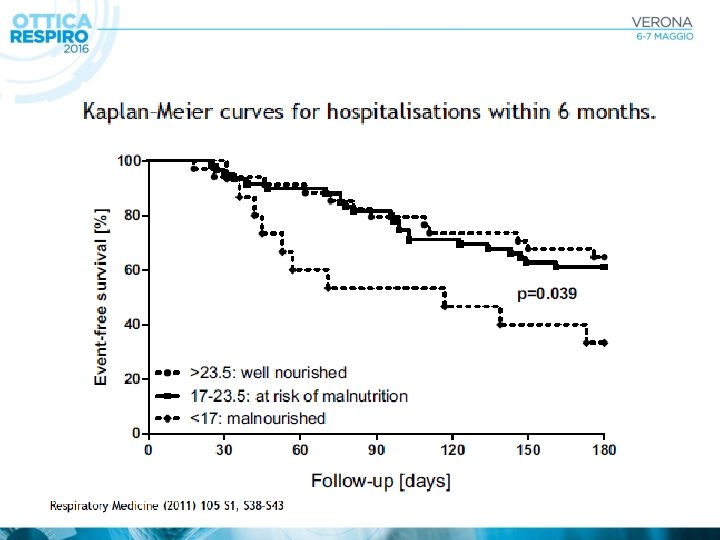

Relation between muscle mass and strength and clinical outcomes in patients with COPD
- Slides: 38