MALIGNANT SOFT TISSUE CONNECTIVE TISSUE TUMORS Fibrosarco Ma

MALIGNANT SOFT TISSUE /CONNECTIVE TISSUE TUMORS

Fibro-sarco. Ma

Definition • A malignant tumor derived from fibrous connective tissue and characterized by immature proliferating fibroblasts or undifferentiated anaplastic spindle cells. • This is a type of sarcoma that is predominantly found in the area around bones or in soft tissue such as muscles, connective tissues, blood vessels, joints and fat. • Fibrosarcomas develop from fibroblasts, which produce connective tissue such as collagen.

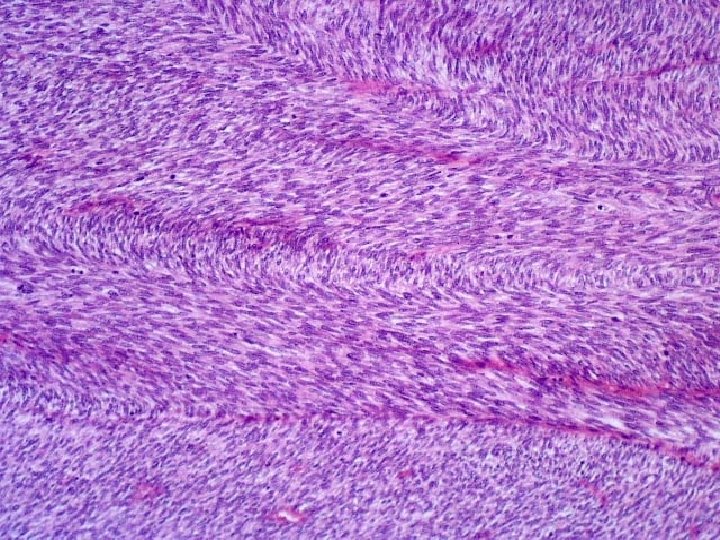
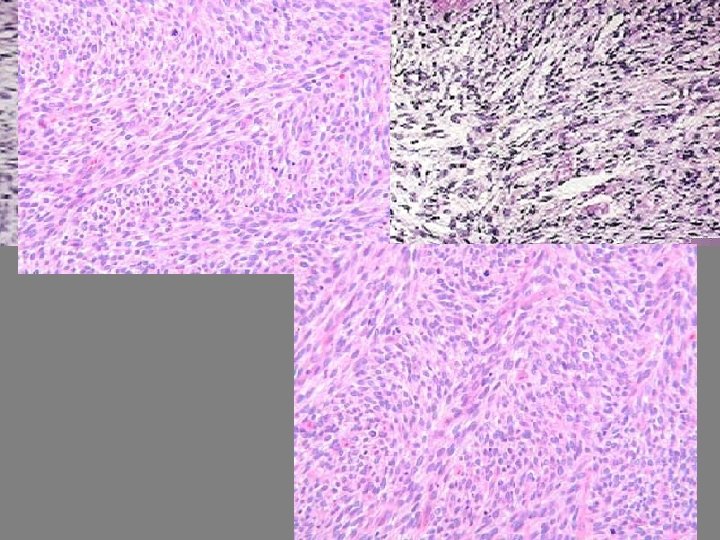
• The immature, proliferating fibroblasts take on an interlacing, or herringbone, pattern.

ETIOPATHOGENESIS • Genetic mutation • Inherited syndromes – Multiple neurofibromas • From preexisting lesions

TYPES Secondary Primary Soft tissue Bone From preexisting lesions/Radiotherapy INFANTILE OR ADULT FIBROSARCOMA

Fibrosarcomas of the bone • Fibrosarcoma can also occur in bones because it has an organic element made up of 95% collagen, similar to the collagen found in the skin. • Fibrosarcomas of the bone usually occur in long bones in the bone marrow cavity where collagen is formed. • The bones that predominantly yield fibrosarcomas are those in the legs, arms, pelvis, and hip.

• Fibrosarcomas of the bone are sometimes connected with underlying benign bone tumors. • As a side effect from previous radiation therapy for primary cancer treatment. • Individuals with other bone diseases, such as Paget's disease and osteomyelitis, are at a higher risk for developing fibrosarcomas.

Clinical features • Demographics – between the ages of 25 -79. (peak age 55 -69 years). – equally in men and women, Site – soft tissue or bone • Though they are rare in children, there is a condition called Infantile fibrosarcoma, which is also known as congenital fibrosarcoma or juvenile fibrosarcoma, is unique. • It is similar to fibrosarcomas seen in adult, but have a more positive prognosis with a posttreatment, five-year survival rate of 83% to 94%.

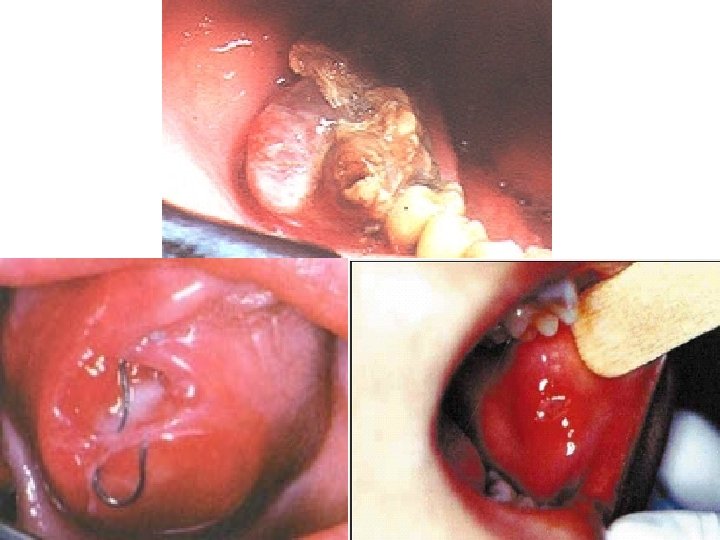
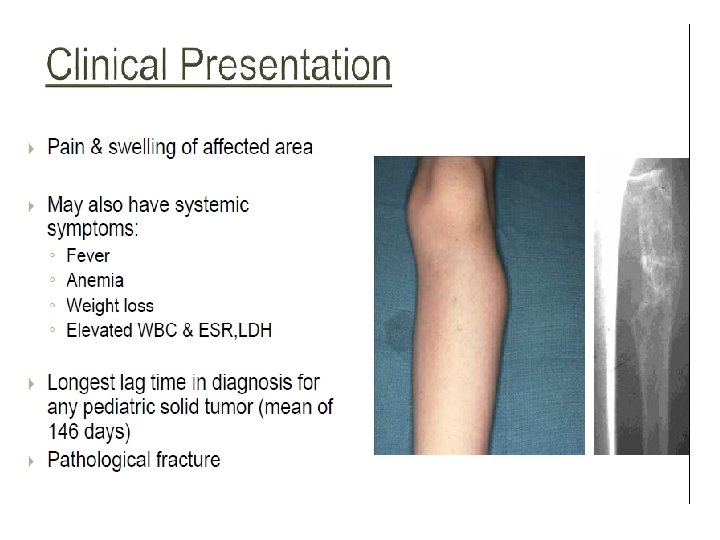
Clinical presentations • FIBROSARCOMA OF BONE – PAIN & SWELLING – PATHOLOGIC FRACTURE • SOFT TISSUE FIBROSARCOMA – PAINLESS MASS (Large painless mass deep to fascia with ill defined margins)


RADIOGRAPH

H/F • WELL DIFFERENTIATED • INTERMEDIATE • HIGH GRADE

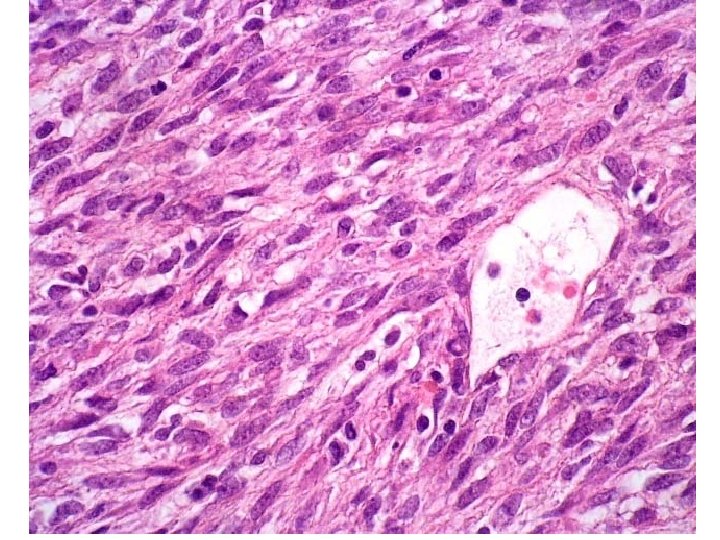
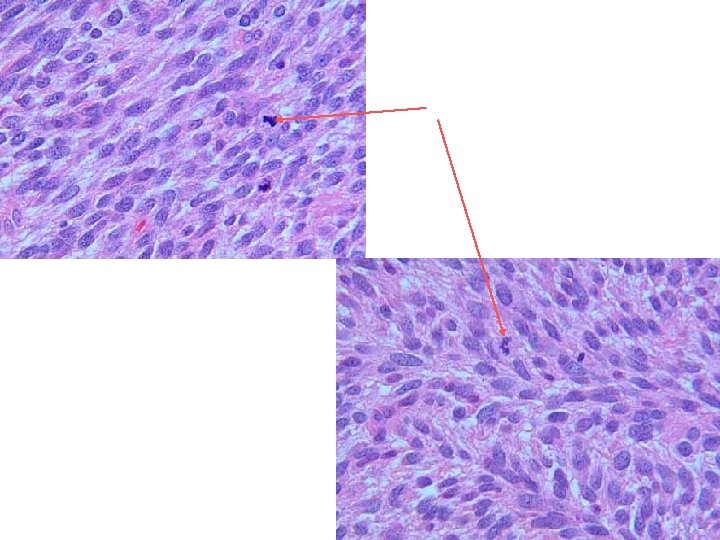
WELL DIFFERENTIATED • Multiple plump fibroblasts in a rich collagenous back ground • Normal mitotic figures

INTERMEDIATE • Cellular • Herring bone pattern • Slight degree of cellular pleomorphism • Moderate amounts of mature collagen • Areas of hyalinisation

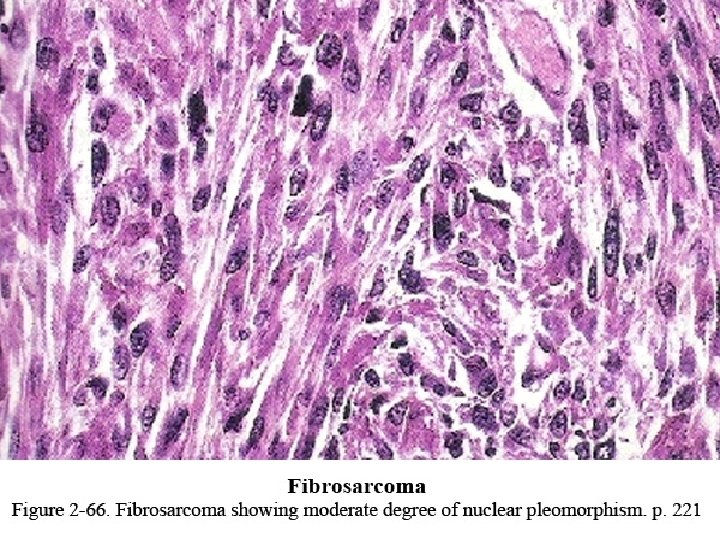
HIGH GRADE • Very cellular • Marked cellular atypia • Increased mitotic activity • Higher grades extremely anaplastic & pleomorphic

Diagnosis • Patient's medical history • physical exam. • Blood tests to rule out other conditions • x ray can show the location, size, and shape of the tumor. • computed tomography (CT) scans, magnetic resonance imaging (MRI), angiograms, and biopsies.

Treatment & Prognosis • Radical excision, associated or not with radiotherapy, is therapy of choice. • Adjuvant chemotherapy has also been used in high grade lesions • The local recurrence rate ranges between 18 and 79% • Distant metastases occur in 63% of the cases within 5 years after the diagnosis and the lungs and bones are the most common sites. • Currently, the overall 5 -year survival rate of the adult fibrosarcoma is 39%.

OSTEOSARCOMA

Osteosarcoma • is the most common type of malignant bone cancer, accounting for 35% of primary bone malignancies affecting mainly tubular long bones. • It is a malignant connective (soft) tissue tumor of primitive bone forming cell whose neoplastic cells present osteoblastic differentiation and form tumoral bone.
 • Children with")
ETIOLOGY • Genetic predisposition • Bone dysplasias (Pagets disease, Fibrous dysplasia) • Children with inherited one of the rare syndromes also are at higher risk for osteosarcoma. 1. retinoblastoma (a malignant tumor that develops in the retina, usually in children younger than age) 2. Li-Fraumeni syndrome (a kind of inherited genetic mutation). • Exposure to radiation is another trigger for DNA mutations, children who have received radiation treatments for a prior episode of cancer are also at increased risk for osteosarcoma
,")
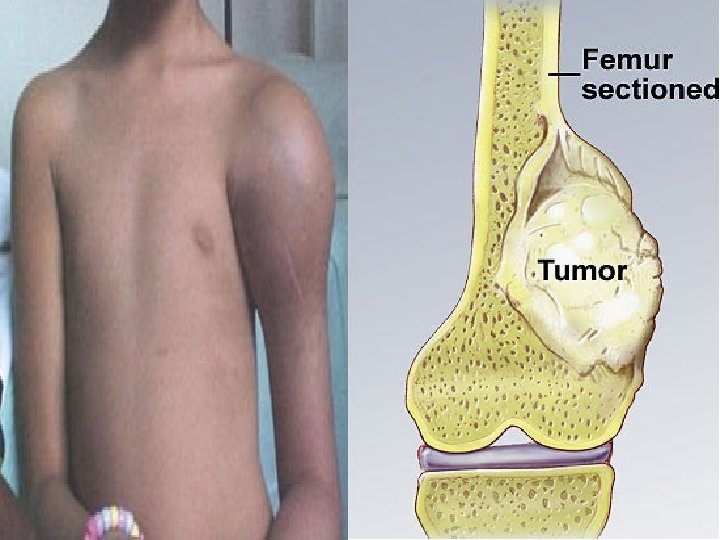
• Because osteosarcoma usually develops from osteoblasts (the cells that make growing bone), it most commonly affects teens who are experiencing a growth spurt. • Boys are more likely to have osteosarcoma than girls, and most cases of osteosarcoma involve the knee. • Most osteosarcomas arise from random and unpredictable errors in the DNA of growing bone cells during times of intense bone growth.

• • • VARIANTS CONVENTIONAL - OSTEOBLASTIC - CHONDROBLASTIC - FIBROBLASTIC MULTIFOCAL TELANGIECTATIC SMALL CELL INTRA OSSEOUS WELL DIFFERENTIATED INTRACORTICAL PERIOSTEAL PARAOSTEAL HIGH GRADE EXTRAOSSEOUS

C/F • Incidence - 3 RD most common cancer • Site – Long bone of extremities (There is a preference for the metaphyseal region of tubular long bones. 50% of cases occur around the knee. ) • Also involve Skull or Jaw • Gender predilection - M>F • Age - 10 -25 yrs ( related to growth spurts)

C/F • The most common symptoms are SWELLING & PAIN in a child's leg or arm. • Pain may be worse during exercise or at night, • A lump or swelling may develop in the affected area up to several weeks after the pain starts. • Pain that persistently wakes the child up at night and pain • In osteosarcoma of the leg, the child may also develop an unexplained limp. • In some cases, the first sign of the disease is pathological fracture because the cancer has weakened the bone to make it vulnerable to a break.

Oral Manifestations Tooth ache Bleeding Nasal obstruction Mand > Max

Diagnosing Osteosarcoma • • detailed medical history a physical exam, X-rays to detect any changes in bone structure. magnetic resolution imaging (MRI) scan

R/F • SUNRAY PATTERN • WIDENING OF PERIODONTAL SPACE • CODMANS TRIANGLE – Acute angle b/w periosteum and bone surface

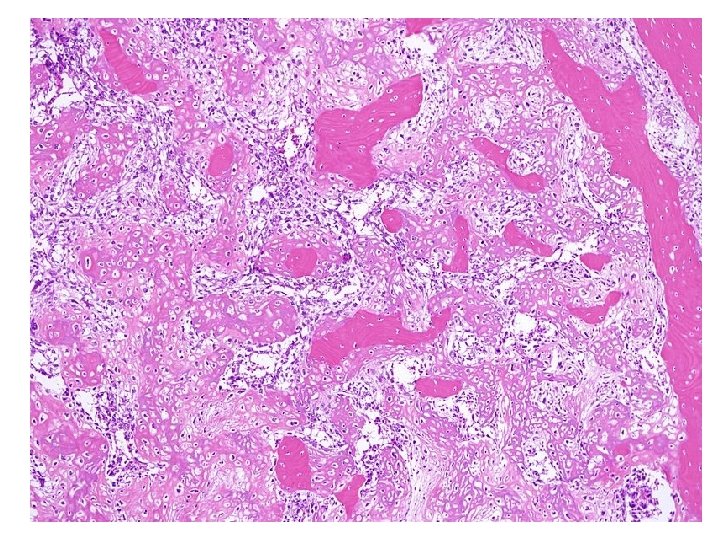
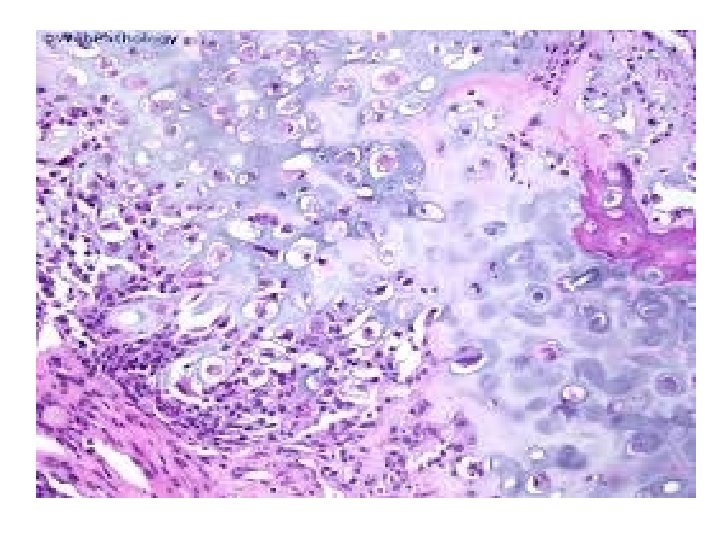
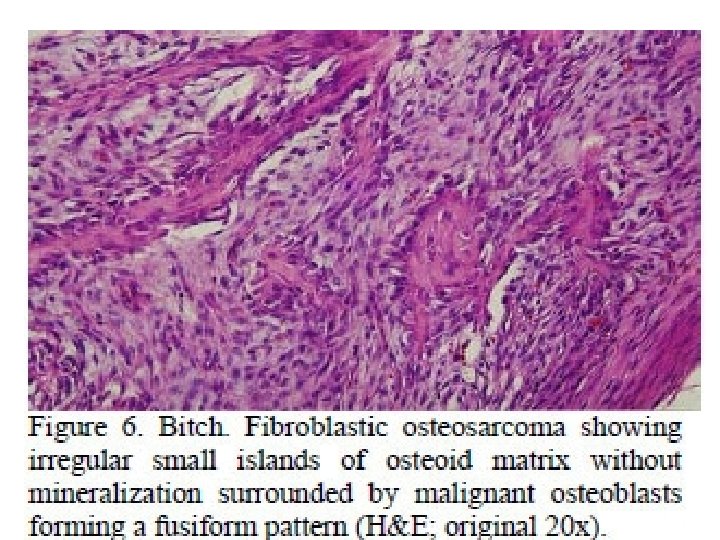
Types - OSTEOBLASTIC - CHONDROBLASTIC - FIBROBLASTIC

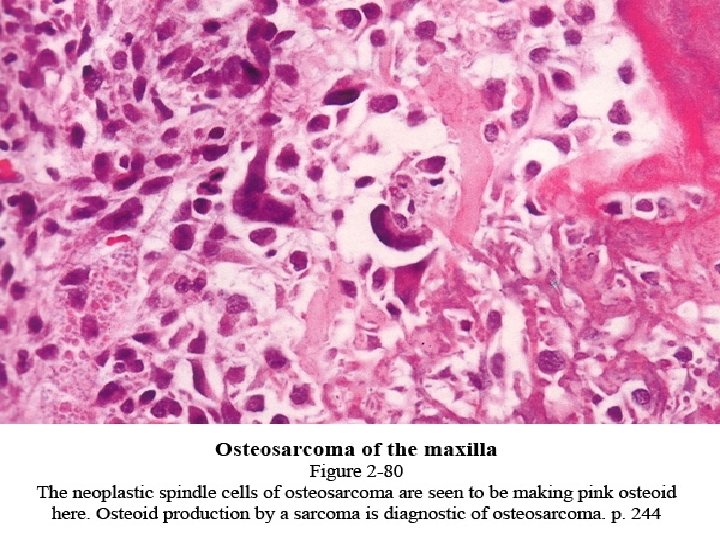
• Proliferation of atypical osteoblasts and its precursors. • Tumor Osteoid • Stromal cells spindle shaped, atypical, irregular nuclei • Conventional type classified based on predominant cell H/P

Treatment & Prognosis • Surgery • Chemotherapy • osteosarcoma is one of the few that actually begin in bones and sometimes spread (or metastasize) elsewhere, usually to the lungs or other bones.

KAPOSI SARCOMA/ ANGIORETICULOENDOTHELIOMA
![CLINICAL FEATURES • 4 clinical presentation of the lesion: • CLASSIC • ENDEMIC [LYMPHADENOPATHIC]](http://slidetodoc.com/presentation_image_h/9e6243fa7f5daf13e376c7ff437192f8/image-46.jpg "CLINICAL FEATURES • 4 clinical presentation of the lesion: • CLASSIC • ENDEMIC [LYMPHADENOPATHIC]")
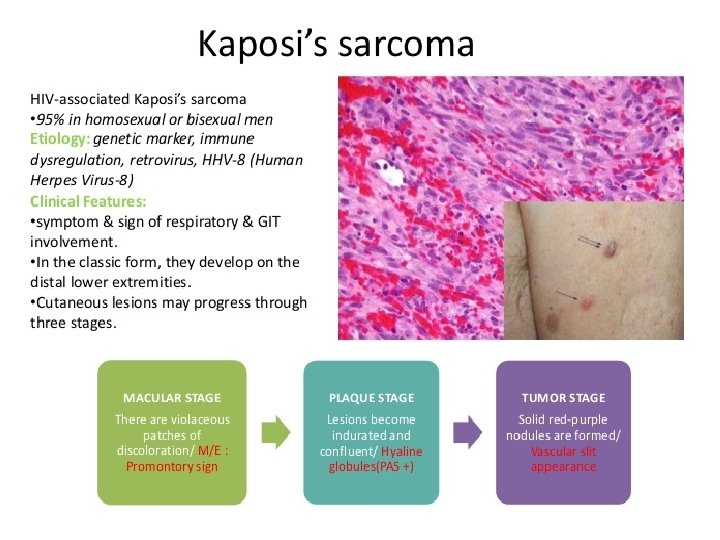
CLINICAL FEATURES • 4 clinical presentation of the lesion: • CLASSIC • ENDEMIC [LYMPHADENOPATHIC] • IMMUNOSUPPRESSION – ASSOCIATED • AIDS RELATED FLAT , BLUE, RED, PURPLE PLAQUES LATER EXOPHYTIC, ULCERATED LYMPH NODE & SALIVARY GLAND
 • Cutaneous blue red nodule develops on lower extremities , with regressing")
CLASSIC (CHRONIC) • Cutaneous blue red nodule develops on lower extremities , with regressing and newly forming. • Oral lesion appear as bluish nodule of the palatal mucosa.

• ENDEMIC: • Young African children are affected with local/generalized enlargement of lymph nodes. • Minimal skin & mucosal involvement.
 • Renal transplant patients become manifested 1 or 2 years later the")
TRANSPLANTATION (IMMUNOSUPPRESSION) • Renal transplant patients become manifested 1 or 2 years later the transplantation. • Sarcomatous involvement occurs on the skin as well as internal organs, but oral lesions are rare.

AIDS related Kaposi sarcoma • It affects cutaneous and oral part. • Oral lesions appear as red or purple color plaque, either focal or diffuse. • Over a period of time lesion becomes nodular, ulcerated and exophytic. • Salivary gland lymph nodes are enlarged.

Kaposi’s Sarcoma – palate CDC

Kaposi’s sarcoma. .

Kaposi’s sarcoma. .

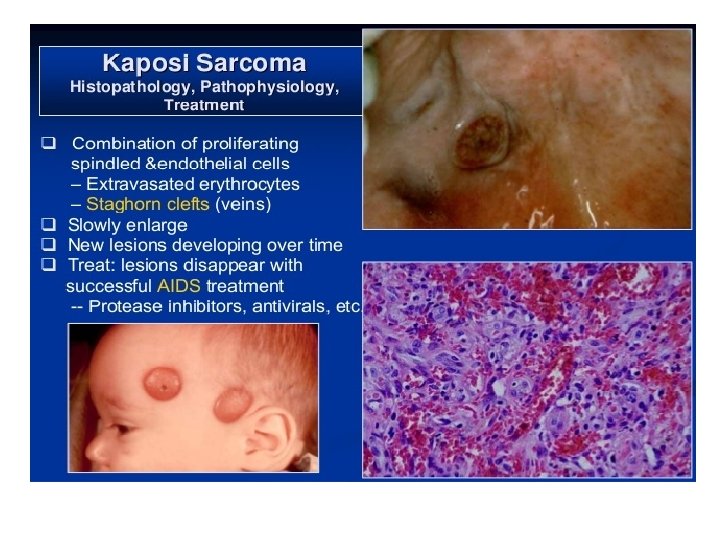
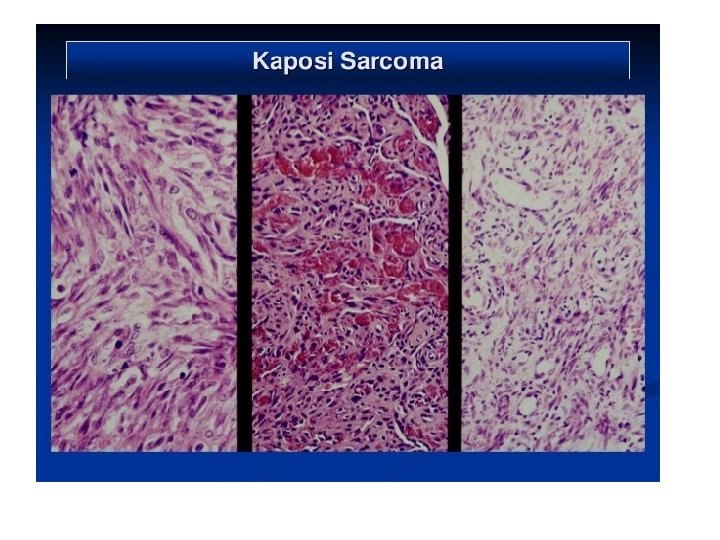
HISTOPATHOLOGICAL TYPES PATCH STAGE PLAQUE STAGE NODULAR STAGE

PATCH STAGE • PROLIFERATION OF VEINS & CAPILLARIES • SLIT LIKE VESSELS AROUND PRE EXISTING BLOOD VESSELS. • PLUMP ATYPICAL ENDOTHELIAL CELLS • MONONUCLEAR LYMPHOCYTES • MAST CELLS, ERYTHROCYTES • HEMOSIDERIN PIGMENTS • Perivascular proliferation of spindle cells with minimal atypia
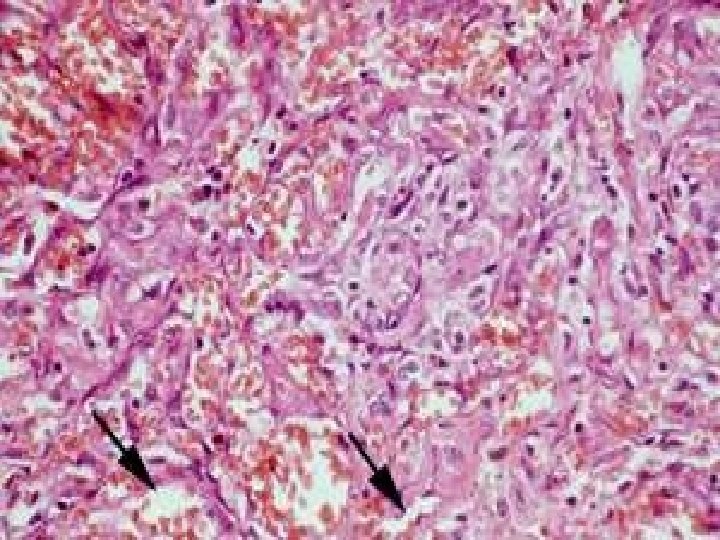

PLAQUE STAGE • • • INCREASED CAPILLARIES DILATED VASCULAR CHANNELS ATYPICAL SPINDLE CELLS EXTRAVASATED ERYTHROCYTES ABUNDANT HEMOSIDERIN CELLS WITH HYPERCHROMATIC NUCLEI, MODERATE PLEOMORPHISM, CHRONIC INFLAMMATORY CELL INFILTRATION
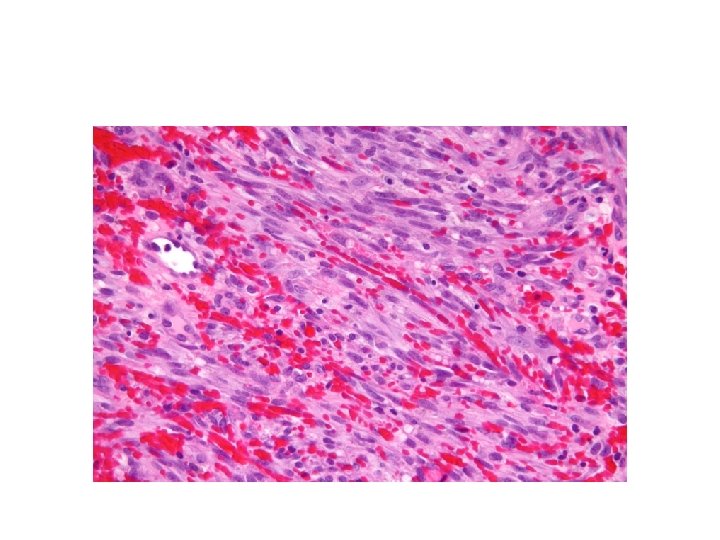

NODULAR STAGE
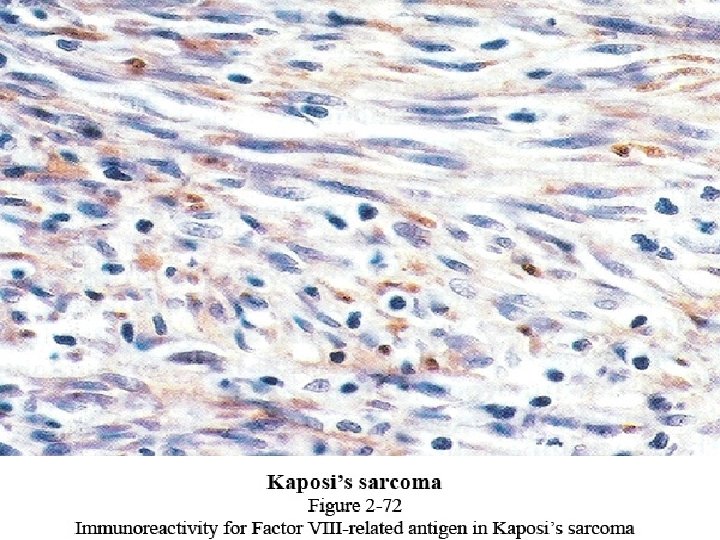

Kaposi’s sarcoma. .

Ewings sarcoma/Round cell sarcoma

Radiographic features • Irregular diffuse radiolucency. • Layers of new subperiosteal bone production leads to ‘’onion skin’’ appearance.

• ‘’Sun ray/sun burst’’ appearance due to osteophyte formation.

Histopathology • Sheets of small round cells with little stroma. • Cells are small and round in shape with scanty cytoplasm, large round nuclei with dispersed chromatin & hyperchromatism. • The cells are arranged in filigree pattern.

Multiple myeloma
? Multiple myeloma (MM) is characterized by the neoplastic proliferation of")
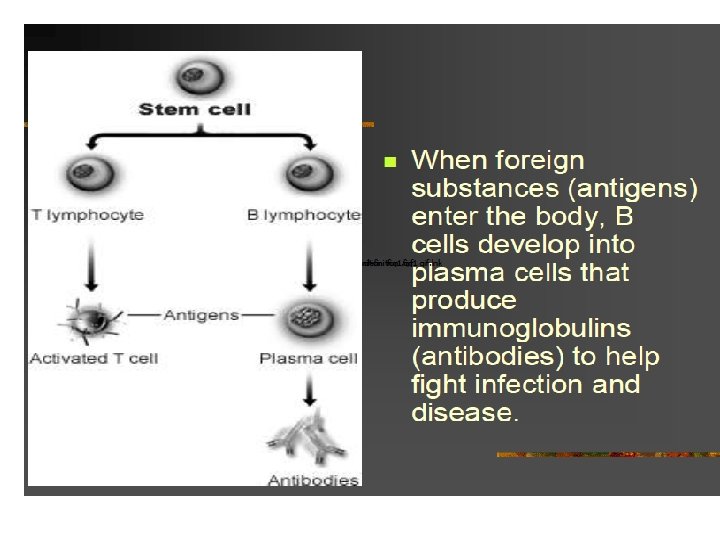
What is MM(multiple myeloma)? Multiple myeloma (MM) is characterized by the neoplastic proliferation of a single clone of plasma cells producing a monoclonal immunoglobulin.

Pathology Multiple myeloma is characterized by excessive numbers of abnormal plasma cells in the bone marrow and overproduction of intact monoclonal immunoglobulin (Ig. G, Ig. A, Ig. D, or Ig. E) or Bence. Jones protein (free monoclonal κ and λ light chains). Hypercalcemia, anemia, renal damage, increased susceptibility to bacterial infection, and impaired production of normal immunoglobulin are common clinical manifestations of multiple myeloma. It is often also characterized by diffuse osteoporosis, usually in the pelvis, spine, ribs, and skull.

Plasma Cell

Incidence • MM occurs in all races and all geographic locations • African Americans and blacks from Africa is two to three times the risk in whites • Risk is lower in Asians from Japan and in Mexicans • Slightly more frequent in men than in women (1. 4: 1)

Age • MM is a disease of older adults • The median age at diagnosis is 66 years • Only 10 percent of patients are younger than 50 years • Only 2 percent of patients are younger than 40 years

Risk factors: • Radiation exposure • Occupational exposure(agricultural, rubber plant, chemical, paper and leather workers) • Chemical exposure to benzene, formaldehyde, hair dyes, paint sprays, and asbestos.

Clinical Presentations • Old age group, 60 -65 years • M>F • Bone involvement: axial skeleton, ribs, skull, pelvis, femur bone. • Clinical signs & symptoms: • Bone pain, anemia, lytic bone lesions, hypercalcimia.

Oral manifestation Mandible bone > maxilla Ramus - angle- molar region Pain , swelling & expansion of the jaw. Extra skeletal lesions may resemble gingival lesions. • Extension of the disease to the lymph nodes, skin, viscera. • •

Radiographic features • Punched out areas in a variety of bones like vertebrae, ribs, skull, jaws, ends of long bones.

Lytic Bone Lesion

Multiple Myeloma = M-CRAB • • • Monoclonal protein Calcium Renal failure Anemia Bone pain with lytic lesions
 • Reversal of albumin-globulin ration resulting in increase")
Laboratory findings • Hyperglobulinemia (monoclonal gammopathy) • Reversal of albumin-globulin ration resulting in increase in total serum protein. • Bence jones protein in the urine. • It is unusual protein which coagulates when it is heated at 40 -60 degrees, disappears when it is boiled, and reappears when it is cooled. • Anemia

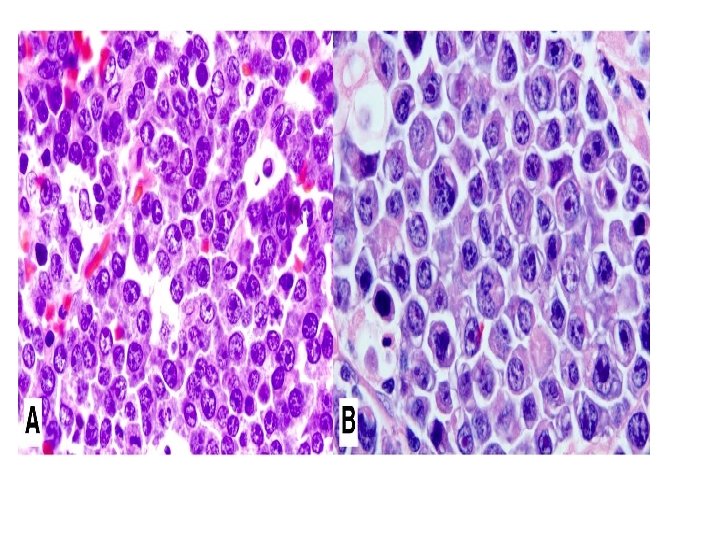
Histopathology • Plasma cells arranged in sheets, exhibiting cart wheel or check board pattern. • Perinuclear halo is seen. • Russell bodies are common.


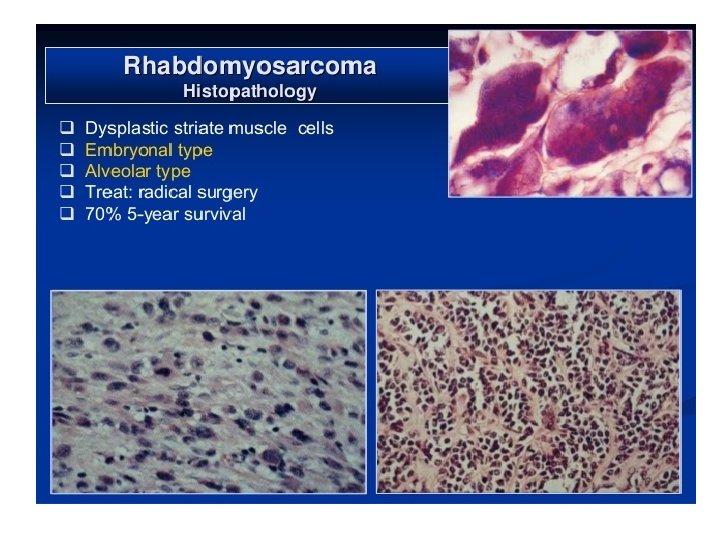
• Malignant tumor of striated muscle. • Derived from primitive mesenchyme, which can give skeletal muscle differentiation. • Four sub types: • Embryonal • Botroid • Alveolar • pleomorphic

Embryonal rhabdomyosarcoma • It is observed in children • Site: head & neck, genitourinary region.

Botryoid rhabdomyosarcoma • Site: bladder, prostate, vagina • Maxillary sinus, nasopharynx, middle ear. Alveolar Rhabdomyosarcoma: Age: 5 -58 years Site: extremities, 18% in head and neck region

• • • Pleomorphic Age: older age group Site: extremities Common symptoms: Pain and swelling Abnormal phonation, dysphagia, cough, deviation of the jaw.

Histopathology • Embryonal: • Eosinophilic spindle cells arranged in interlacing fascicles. • Round eosinophilic cells with small nucleus, granular eosinophilic cytoplasm. • Broad elongated eosinophilic cells with cross striations. • Small round spindle cells with dark staining nuclei.
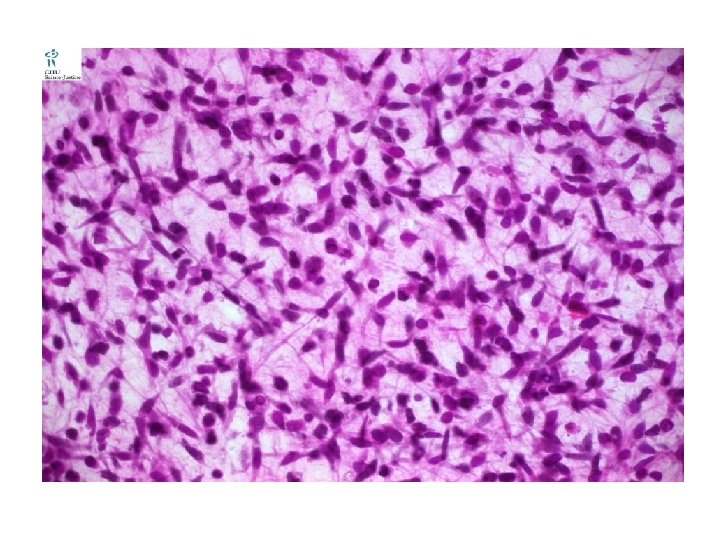

Pleomorphic: Spindle cells in a haphazard arrangement. Nuclei is oval or elongated with chromatin. Bizarre cell, racquet cell, strap and ribbon cells. • Cytoplasm is eosinophilic with vacules. • •
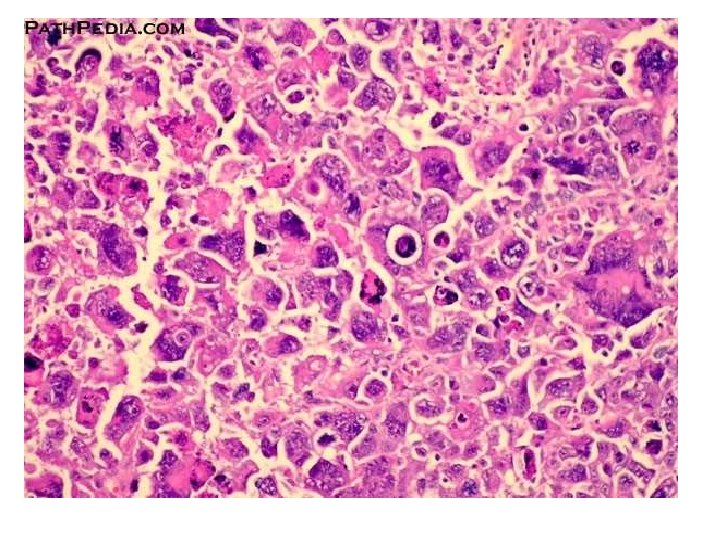
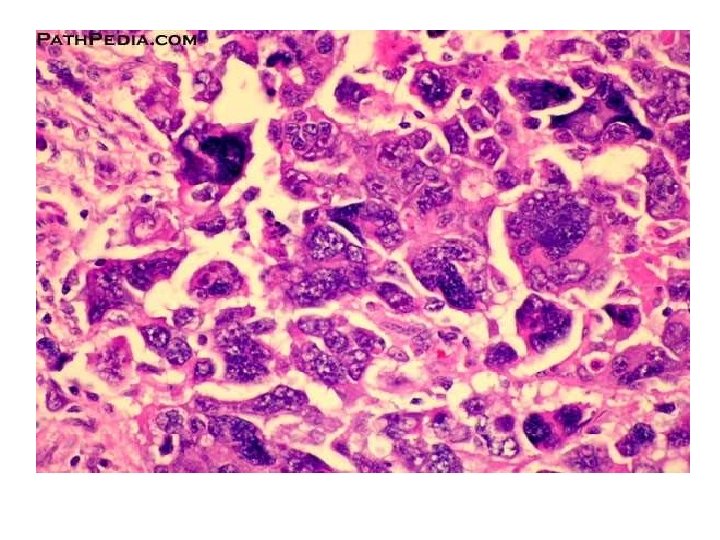

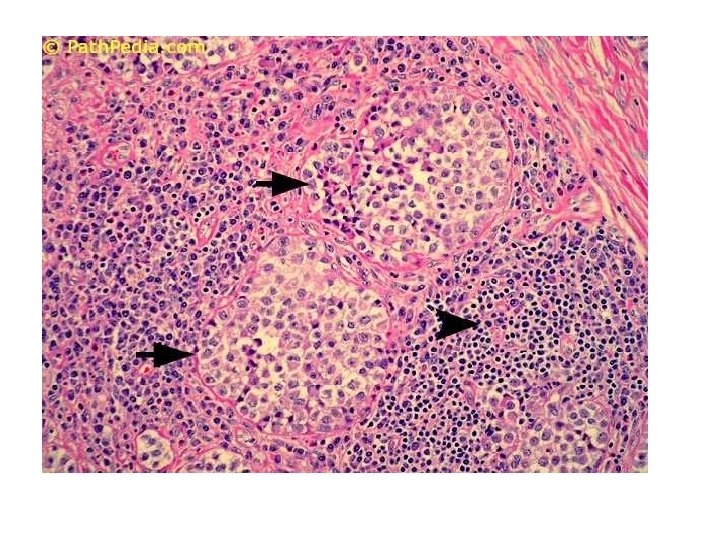
• Alveolar: • Small poorly differentiated round and oval cells aggregated into clusters. • Center of the cluster shows degenerating cells, while periphery shows single layer of cells. • Multinucleated giant cells, mitotic figures are seen.

- Slides: 103