Malignant hematopoiesis 1 Myeloproliferative disorders Emanuel Neas necascesnet
 Myeloproliferative disorders Emanuel Nečas necas@cesnet. cz")


 n lymphoid")







")

 A B B C D")




 Polycythemia vera rubra Chronic myeloid")

 Myeloproliferative Disorders – common features Acquired mutation in a hematopoietic stem cell n")
")
 MDS is a myeloproliferative disease, used to be called „preleukemia“ It")
 bone marrow Normal bone marrow Dysplastic bone marrow")
 a form")

")




 Cumulative survival 1. 0 0. 8 0. 6 0.")
 Phlebotomy Chlorambucil 53 82 Total number")
 75% PFCP 50% Normal EEC 25%")





 Must exclude other causes of bone marrow fibrosis")
")

 chromosome causes a majority of cases of CML The ABL and BCR")




 suppresses")





, several forms (myelogenous, myeloblastic are synonyms")
")


")
 - 8 clinical forms")

")
")


")
 _ M 3 Normal bone marrow APL – promyelocytes do")

_M 3 ATRA = all-trans retinoic acid overcomes defect of RARα")
 is the only „causative therapy“ for")

- Slides: 79
Malignant hematopoiesis (1) Myeloproliferative disorders Emanuel Nečas necas@cesnet. cz
Introduction
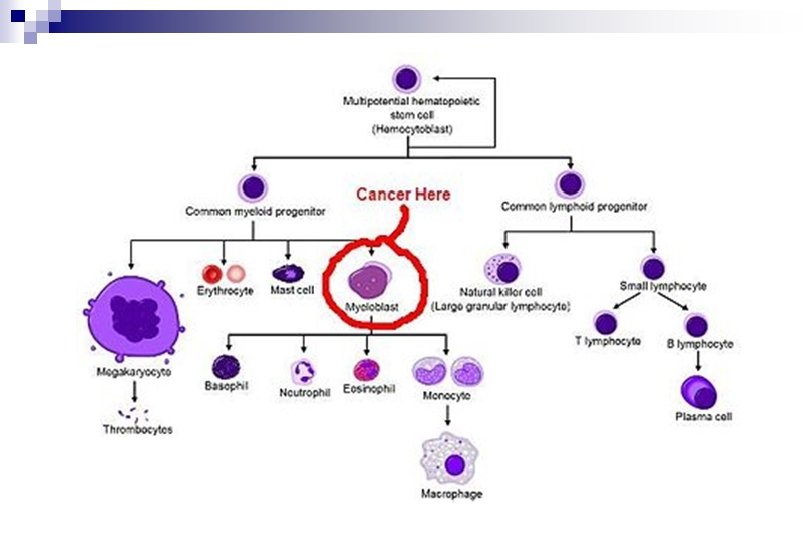
Myelopoiesis and Lymphopoiesis
Myelopoiesis and Lymphopoiesis n myeloid cells (erythropoiesis, granulocytopoiesis, monocytopoiesis, thrombocytopoiesis _ megakaryocytes) n lymphoid cells (B-lymphopoiesis, T-lymphopoiesis, NK-lymphopoiesis)
n Myeloproliferative disorders n Lymfoproliferative disorders
n Myeloproliferative disorders - chronic - acute n Lymfoproliferative disorders - chronic - acute
Lymphoproliferative diseases can also have a form of a solid tumor, a lymphoma. Though seemingly localized to a lymphoid tissue outside the bone marrow, it is considered to be a systemic disease involving (infiltrating) the bone marrow regularly.
A single leukemic stem cells starts the disease. The disease then spreads throughout the body.
Malignant hematopoiesis n n is usually monoclonal is usually systemic
Normal hematopoiesis is polyclonal
Origin of the normal polyclonal hematopoiesis is in embryogenesis A B B C D E F G H F
Malignant hematopoiesis is monoclonal (examples: acute myeloid leukemia; AML)
Xp. Xm female somatic cells Xp. Xm Embryogenesis Xp. Xm random X-inactivation Xm Xp Clonal Event Xp Xp Xm Xp Xp Xm Xm Xm
Malignant monoclonal hematopoiesis is caused by mutations (F´cell clone) A B B C D E F G H F´
Treatment eliminates or supresses the malignant clone and normal polyclonal hematopoiesis usually resumes Possible therapy outcomes n remission n successful treatment (complete remission) n residual disease n relaps
A pathological dominant clone may start from a mutated hematopoietic stem cell but not necessarily. A mutated progenitor cell may be a source of a dominant malignant clone as well.
Normal bone marrow and CML, AML, CLL CML AML CLL
Chronic myeloproliferative disorders
Chronic myeloproliferative diseases n n n Myelodysplastic syndrome (MDS) Polycythemia vera rubra Chronic myeloid leukemia (CML) Essential throbocythemia Idiopathic Myelofibrosis/or Agnogenic Myeloid Metaplasia Chronic lymphocytic leukemia (CLL) …is lymphoproliferative disease
Myeloproliferative Disorders
(Chronic) Myeloproliferative Disorders – common features Acquired mutation in a hematopoietic stem cell n Clonal hematopoiesis n Proliferation of granulocytes, red cells and/or platelets n Splenomegaly (variable) n Bone marrow fibrosis (variable) n
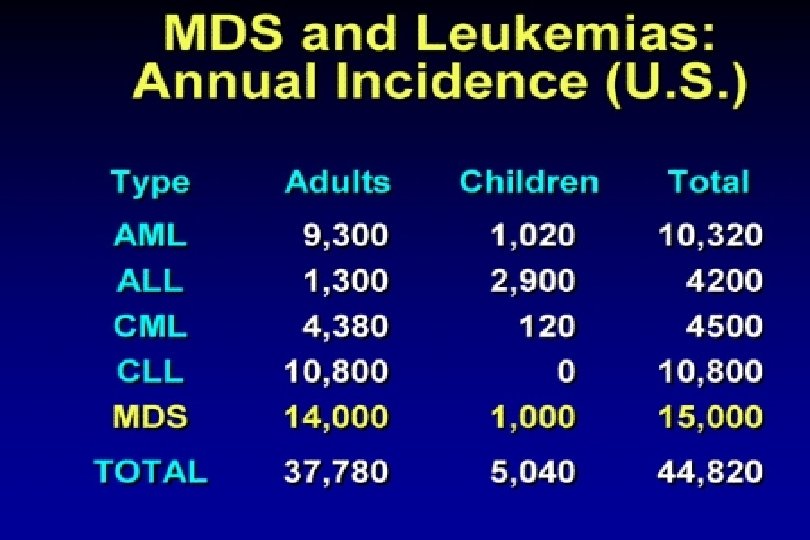
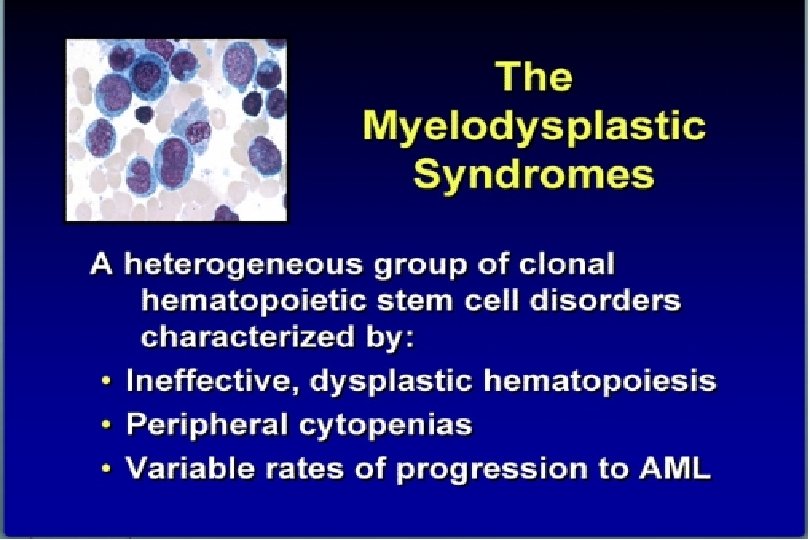
Myelodysplastic syndrome (MDS)
Myelodysplastic syndrome (MDS) MDS is a myeloproliferative disease, used to be called „preleukemia“ It has several forms. There is decreased number of „myeloid“ cell in the blood (anemia, granulocytopenia, thrombocytopenia = pancytopenia)
Normal and dysplastic (MDS) bone marrow Normal bone marrow Dysplastic bone marrow
Dysplastic bone marrow in the RAEB (refractory anemia with excess of blasts) a form of the MDS
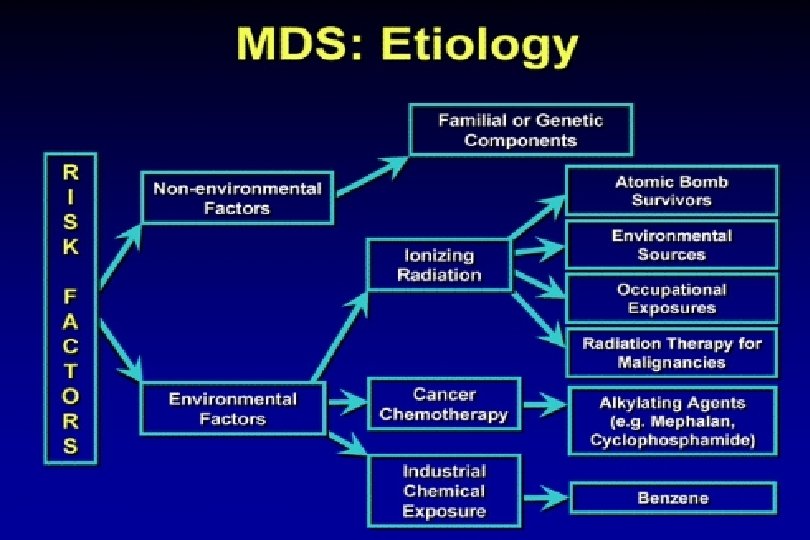
MDS – etiopathogenesis and conversion into AML Altered immune response Altered marrow stroma Oxidative stress Age Altered cytokine response Radiation Increased apoptosis Stem cell mutation T-cell attack Clonal myelopoiesis Clonal evolution Ineffective haemopoiesis Chemicals Additional mutations/epigenetic changes AML
Polycythemia vera rubra („primary polycythemia“, Disease Vasquez-Osler)
Polycythemias Hct 43% 53%
Polycythemia Vera • An acquired mutation of hematopoietic single stem cell The nature of the disease causing mutation not known till 2005 – most cases have mutation in • the JAK 2 tyrosinkinase
Polycythemia vera, Essential trombocythemia, Idiopathic myeolofibrosis
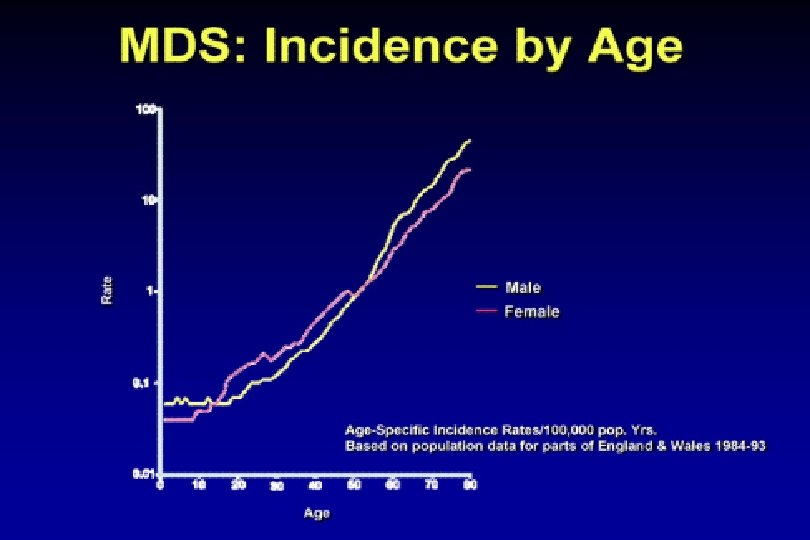
Frequency, % Incidence of Polycythemia Vera Age
Cumulative Survival on Study (PV) Cumulative survival 1. 0 0. 8 0. 6 0. 4 Phlebotomy Chlorambucil 0. 2 32 P 0. 0 0 100 200 300 400 500 Time in weeks 600 700 800
Polycythemia vera causes of death (expressed as percentage) Phlebotomy Chlorambucil 53 82 Total number deaths 32 P 79 Total 214 Thrombosis 17. 2 13. 5 44. 2 Hemorrhage 0. 0 4. 3 3. 8 8. 1 Leukemia/Lymphoma 1. 5 20. 6 11. 5 33. 6 Cancer 4. 5 9. 9 9. 6 24. 0 Spent/MF 0. 7 2. 1 1. 3 4. 1 Other 15. 7 7. 8 10. 9 34. 4
Sensitivity of BFU-E to Epo 100% PV (EEC) 75% PFCP 50% Normal EEC 25% 0% 0 30 60 125 EPO (m. U/ml) 250 3000
Essential thrombocytemia
Essential Thrombocythemia n Platelet count in excess of 600, 000 per mm 3 n Marked megakaryocytic hyperplasia n Abundant platelet clumps
Essential Thrombocythemia n No cytogenetic abnormalities n Splenomegaly seen in fewer than 50% n Morbidity: Thrombotic and/or bleeding problems
Essential Thrombocythemia n No cytogenetic abnormalities n The same mutation in the JAK 2 kinase as causes Polycythemia vera is present in some patients
Idiopathic Myelofibrosis/ Agnogenic Myeloid Metaplasia
Idiopathic Myelofibrosis/ Agnogenic Myeloid Metaplasia (AMM) Must exclude other causes of bone marrow fibrosis ¨ “Spent phase” of PV or ET ¨ CML ¨ Hairy cell leukemia ¨ Lymphoma ¨ Metastatic cancer
Chronic myleoid leukemia (CML)
Chonic Myelogenous Leukemia n n n Proliferation of granulocytes All stages of granulocyte maturation in peripheral blood Platelets may be elevated Polycythemia is rare Splenomegaly, may be massive Invariable transformation to acute leukemia
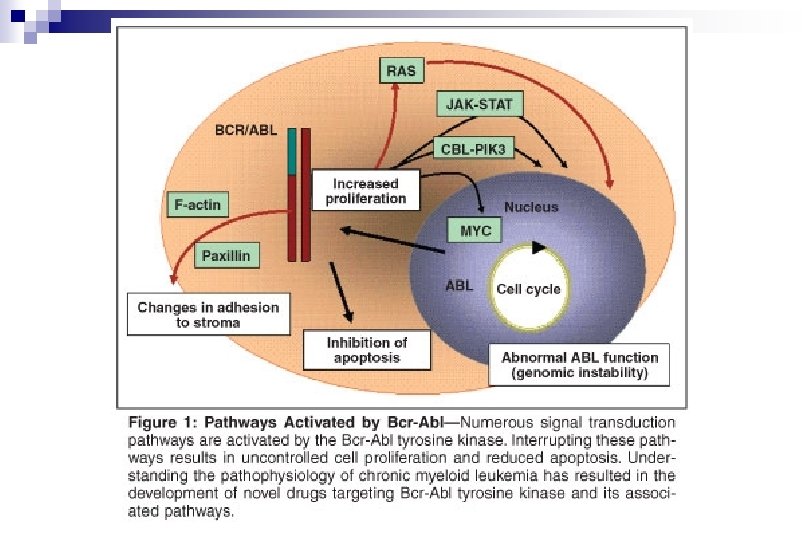
Philadelphia (Ph-) chromosome causes a majority of cases of CML The ABL and BCR genes reside on the long arms of chromosomes 9 and 22, respectively. As a result of the (9; 22) translocation, a BCR-ABL fusion gene is formed on the derivative chromosome 22 (Philadelphia chromosome).
Abnormal BCR-ABL fuse gen and BCR-ABL proteinkinase
Ciba-Geigy started to develop inhibitors of tytrosinkinases 30 years ago
Imatinib binds to BCR/ABL kinase instead of ATP
Přežití nemocných s CML při různé léčbě
„Targeted“ therapy – aimed at the biological cause of a disease Imatinibem (Gleevec) suppresses cells belonging to mutated tumor clone – but does not get rid-off the body of the cause (all mutated cells).
Lasker prize for clinical research 2009 Brian J. Druker Nicholas Lydon Charles L. Sawyers
Mutations of the ABL kinase cause resistence against imatinib
Possible outcomes of CML complete remission n residual disease n relaps n resistance to therapy n blastic conversion (AML) n
Targeted therapy with imatinib is very effective
Important events in CML outlined
Acute myeloproliferative diseases n Acute myeloid leukemia (AML), several forms (myelogenous, myeloblastic are synonyms to myeloid) n Acute lymphocytic leukemia (ALL) … is lymphoproliferative disease (lymphoblastic is a synonym to lymphocytic)
Acute myleoid leukemia (AML)
Leukemic blasts present in blood
Leukemic blasts are present in bone marrow
Karyotype of the major clone from the relapse acute myeloid leukemia (AML)
Acute Myeloid Leukemia (AML) - 8 clinical forms
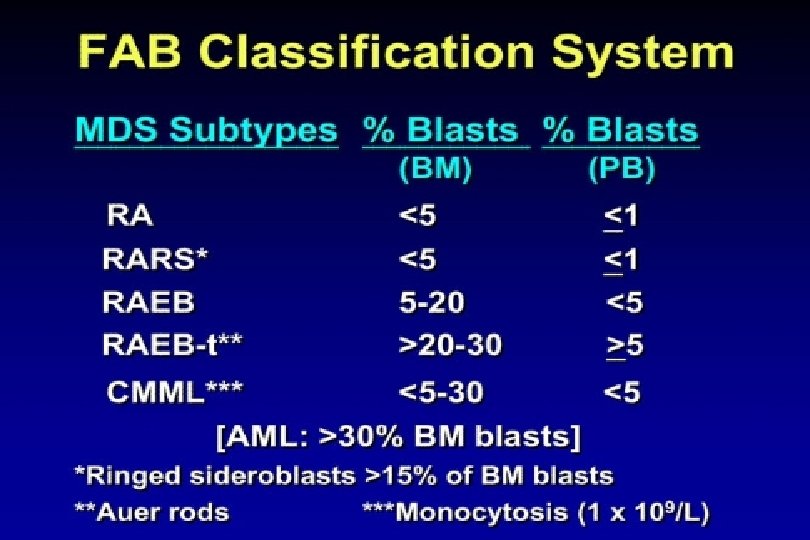
AML subgroups – FAB classification
„Ziskové“ mutace receptoru Flt 3 u akutní myeloidní leukémie (u 1/3 nemocných)
FLT 3 -ITD (internal tandem duplication)
Different AML types differ in prognosis
Flt 3 receptor mutated in 40% of AML cases
FLT 3 -ITD (internal tandem duplication)
Acute promyelocytic leukemia (APL) _ M 3 Normal bone marrow APL – promyelocytes do not mature into granulocytes
Chromosomal translocation in APL results in abnormal – PML-RARα protein
Acute promyelocytic leukemia (APL)_M 3 ATRA = all-trans retinoic acid overcomes defect of RARα protein and induces maturation of pathological promyelocytes = „targeted therapy“ induce remission of the disease
Transplantation of hematopoietic stem cells („Bone Marrow Transplantation“) is the only „causative therapy“ for AML
END OF THE LECTURE