Male genital system MALE GENITAL SYSTEM PENIS SCROTUM




")
")

 – Inflammation")


 – EPIDEMIOLOGY • UNCOMMON –")


 • Superficial dermatophyte")











 – Seminomas (50%) –")
 GERM CELL PRECURSOR GONADAL DIFFERENTIATION TOTIPOTENTIAL DIFFERENTIATION (NONSEMINOMA)")








- Slides: 38
Male genital system
MALE GENITAL SYSTEM • PENIS • SCROTUM, TESTIS, & EPIDIDYMIS • PROSTATE
PENIS • MALFORMATIONS • INFLAMMATORY LESIONS • NEOPLASMS
MALFORMATIONS OF THE PENIS Abnormal location of urethral orifice along penile shaft – Hypospadias (ventral aspect) • Most common (1/250 live male births) – Epispadias (dorsal aspect)
Hypospadias (ventral)
Epispadias (dorsal)
HYPOSPADIAS AND EPISPADIAS – May be associated with other genital abnormalities • Inguinal hernias • Undescended testes – Clinical consequences • Constriction of orifice • Urinary tract obstruction • Urinary tract infection • Impaired reproductive function
INFLAMMATORY LESIONS OF THE PENIS • Sexually transmitted diseases • Balanitis (balanoposthitis) – Inflammation of the glans (plus prepuce) – Associated with poor local hygiene in uncircumcised men • Smegma – Distal penis is red, swollen, tender • +/- Purulent discharge
INFLAMMATORY LESIONS OF THE PENIS • PHIMOSIS – PREPUCE CANNOT BE EASILY RETRACTED OVER GLANS – MAY BE CONGENITAL – USUALLY ASSOCIATED WITH BALANOPOSTHITIS AND SCARRING – PARAPHIMOSIS (TRAPPED GLANS) • URETHRAL CONSTRICTION
INFLAMMATORY LESIONS OF THE PENIS • FUNGAL INFECTIONS – CANDIDIASIS • ESPECIALLY IN DIABETICS • EROSIVE, PAINFUL, PRURITIC • CAN INVOLVE ENTIRE MALE EXTERNAL GENITALIA
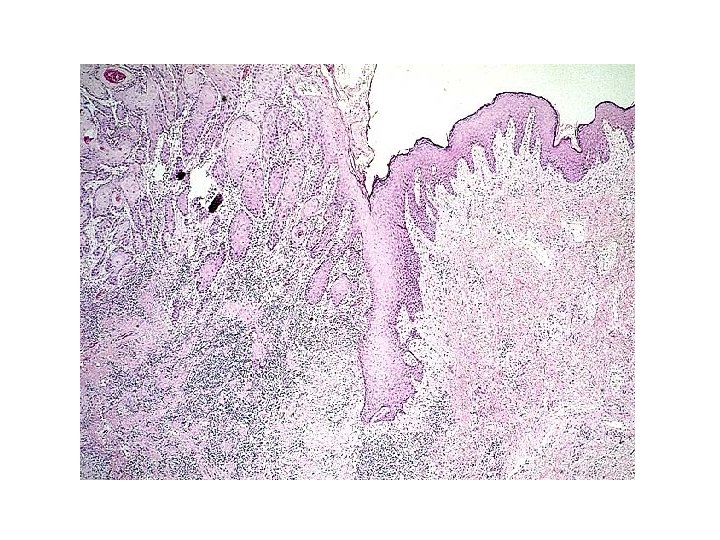
NEOPLASMS OF THE PENIS • SQUAMOUS CELL CARCINOMA (SCC) – EPIDEMIOLOGY • UNCOMMON – LESS THAN 1 % OF CA IN US MEN • UNCIRCUMCISED MEN BETWEEN 40 AND 70 – PATHOGENESIS • POOR HYGIENE, SMEGMA, SMOKING • HUMAN PAPILLOMA VIRUS (16 AND 18) • CIS FIRST, THEN PROGRESSION TO INVASIVE SQUAMOUS CELL CARCINOMA
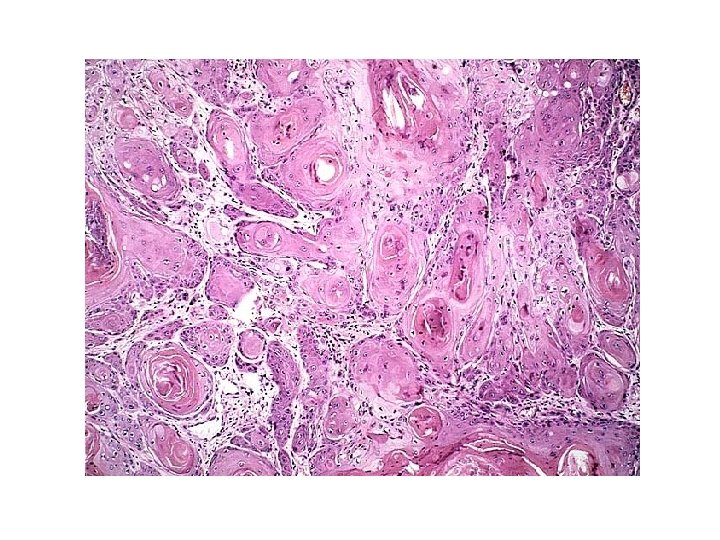
Squamous Cell Carcinoma
SCC OF THE PENIS • Clinical course – Usually indolent – Locally invasive – Has spread to inguinal lymph nodes in 25% of cases at presentation – Distant mets rare – 5 yr survival • 70% without ln mets • 27% with ln mets
LESIONS INVOLVING THE SCROTUM • Inflammation – Tinea cruris (jock itch) • Superficial dermatophyte infection • Scaly, red, annular plaques, pruritic • Inguinal crease to upper thigh • Squamous cell carcinoma – Historical significance – Chimney sweeps used to have this
LESIONS INVOLVING THE SCROTUM • Scrotal enlargement – Hydrocele - most common cause • Accumulation of serous fluid within tunica vaginalis • Infections, tumor, idiopathic – Hematocele – Chylocele • Filiariasis - elephantiasis – Testicular disease
Hydrocele
LESIONS OF THE TESTES • CONGENITAL • INFLAMMATORY • NEOPLASTIC
Cryptorchidism and testicular atrophy • Failure of testicular descent • Epidemiology – About 1% of males (at 1 yr) – Right > left, 10% bilateral • Pathogenesis – Hormonal abnormalities – Testicular abnormalities – Mechanical problems
Atrophic testes secondary to cryporchidism
Cryptorchidism and testicular atrophy • Clinical course – When unilateral, may see atrophy in contralateral testis – Sterility – Increased risk of malignancy (3 -5 x) – Orchiopexy • May help prevent atrophy • May not eliminate risk of malignancy
Other causes of testicular atrophy • • Chronic ischemia Inflammation or trauma Hypopituitarism Excess female sex hormones – Therapeutic administration – Cirrhosis • Malnutrition • Irradiation • Chemotherapy
Inflammatory lesions of the testis • Usually involve the epididymis first • Sexually transmitted diseases • Nonspecific epididymitis and orchitis – Secondary to uti • Bacterial and non-bacterial – Swelling, tenderness – Acute inflammatory infiltrate
Inflammatory lesions of the testis • Mumps – 20% of adult males with mumps – Edema and congestion – Chronic inflammatory infiltrate – May cause atrophy and sterility • Tuberculosis – Granulomatous inflammation – Caseous necrosis
TESTICULAR NEOPLASMS • Epidemiology – Most important cause of painless enlargement of testis – 5/100, 000 males, whites > blacks (us) – Increased frequency in siblings – Peak incidence 20 -34 yrs – Most are malignant – Associated with germ cell maldevelopment • Cryptorchidism (10%) • Testicular dysgenesis(xxy)
TESTICULAR NEOPLASMS • Pathogenesis – 95% arise from germ cells • ISOCHROMOSOME 12, i(12 p), IS A COMMON FINDING • Intratubular germ cell neoplasms – Rarely arise from sertoli cells or leydig cells • These are often benign – Lymphoma • Men > 60 yo
WHO CLASSIFICATION OF TESTICULAR TUMORS • One histologic pattern (60%) – Seminomas (50%) – Embryonal carcinoma – Yolk sac tumor – Choriocarcinoma – Teratoma • Multiple histologic patterns (40%) – Embryonal ca + teratoma – Choriocarcinoma + other – Other combinations
HISTOGENESIS OF TESTICULAR NEOPLASMS (PEAK INCIDENCE) GERM CELL PRECURSOR GONADAL DIFFERENTIATION TOTIPOTENTIAL DIFFERENTIATION (NONSEMINOMA) SEMINOMA (40 -50 Y) TROPHOBLASTIC DIFFERENTIATION CHORIOCARCINOMA (20 -30 Y) h. CG + EMBRYONAL CA (UNDIFFERENTIATED) (20 -30 Y) YOLK SAC DIFF YOLK SAC TUMOR (< 3 Y) AFP + SOMATIC DIFFERENTIATION TERATOMA (ALL AGES) MATURE IMMATURE MALIGNANT TX
Seminoma, with focal hemorrhage and necrosis
Normal testicular tissue
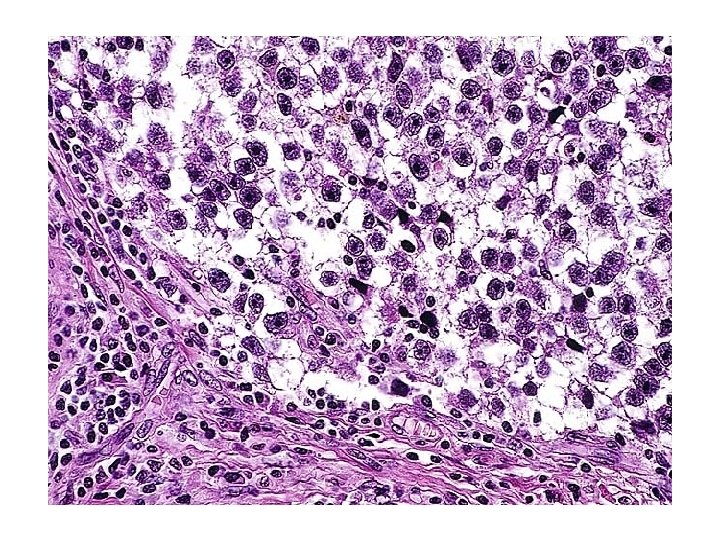
Seminoma
Seminoma Syncytiotrophoblast
Dermoid Cyst
Immature Teratoma With Embryonal Carcinoma
Clinical course • Usually present with painless enlargement of testis • May present with metastases – Nonseminomas (more common) • Lymph nodes, liver and lungs – Seminomas • Usually just regional lymph nodes • TUMOR MARKERS (hcg AND AFP) • Treatment success depends on histology and stage – Seminomas very sensitive to both radio- and chemotherapy
Thank You