Malaria By Mohamed Abd El Maksoud MD Tropical

Malaria By Mohamed Abd El Maksoud MD Tropical Medicine
 and aria (air) – it")
Backgroud The name comes from the Italian mal (bad) and aria (air) – it was originally thought the disease was spread by the damp air from swamps. The link between the disease and the Anopheles Mosquito was first made by Ronald Ross, a Scottish army doctor, working in India.

q q q Malaria is endemic throughout most of the tropics. Of the approximately 3. 4 billion people worldwide who are exposed annually, 1. 2 billion are at high risk The World Health Organization (WHO) states that there were 198 million cases of symptomatic malaria in 2013

Difinition Malaria is an acute and chronic disease caused by obligate intracellular protozoa of the genus Plasmodium, which contains 4 human species. P. falciparum (malignant malaria). P. vivax (benign tertian malaria). P. ovale (ovale tertian malaria). P. malariae (quartan malaria).

In Egypt, P. vivax is the commonest type and the female anopheles (pharoensis or sergenti) is the commonest vector.

Transmission 1 -Bite of an infected female Anopheles mosquito � Risk of transmission is increased through exposure in rural areas at the end of the rainy season 2 -Rarely: blood transfusion shared needle use Congenital from mother to fetus

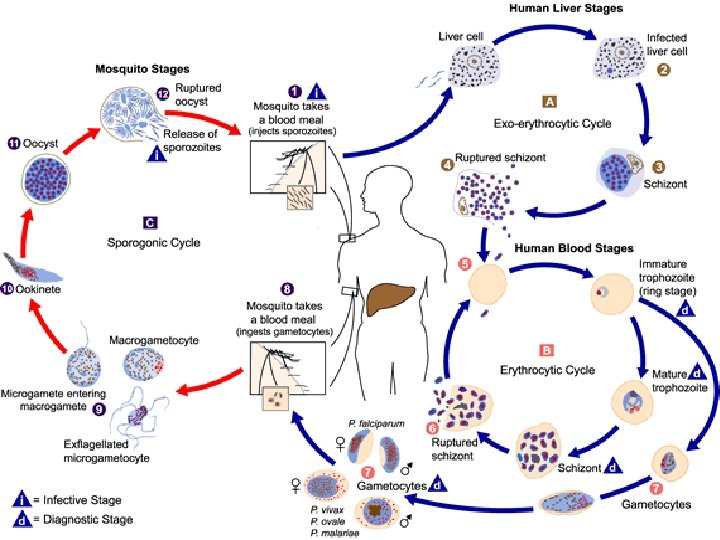
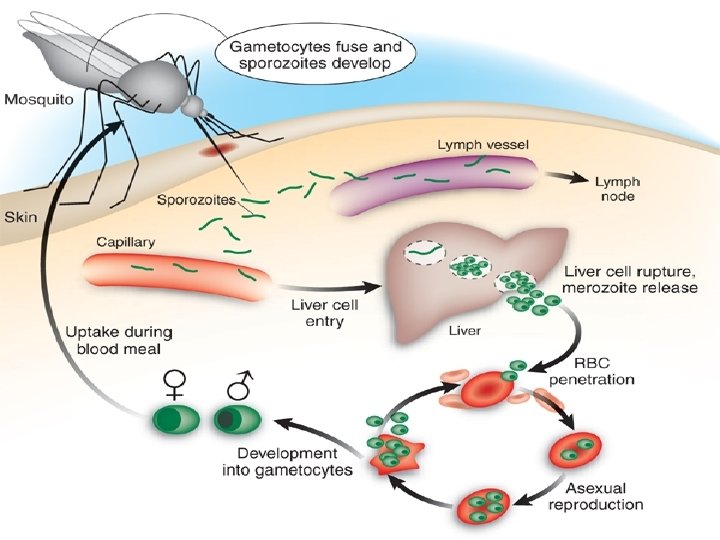
Life cycle The life cycle is complex and involves mainly 2 cycles: Human cycle Anopheline cycle • Occurs in man (liver & • Occur in female RBCs) anopheles. • The parasites multiply by • The parasites multiply an asexual method called sexually by method called schizogony or merogony sporogony ends by in which the nucleus and formation of sporozoit. cytoplasm divide into merozoites

Asexual cycle -Infection of the man occurs through sporozoit inoculated in the skin through bite of female anopheles. Two cycles occur: - • In the liver (Exoerythrocytic) • In Red cells (Erythrocytic). (Exo-erythrocytic (Erythrocytic The sporozoites inoculated in the skin circulate in blood and washed out into liver cells within 30 m -They get rounded inside the liver cells forming trophozoite which enlarge and its nucleus divides into thousands of particles each become surrounded by part of cytoplasm forming thousands of merozoites. This stage is called "Schizont". -The liver cells which get enlarged and schizont rupture releasing merozoites into blood sinusoids. -The merozoites thus released: 1)Some are histotrapic and infect new liver cells forming another exoerythrocytic cycle (2 ry tissue phase. This phase is the cause of "True relapse in" malaria 2)Some other merozoites are erythrotropic and infect red cells initiating erythrocytic cycle. The merozoites of 1 ry and 2 ry tissue phase will invade red cells -Vacule appears in cytoplasm of each merozoite producing ring stage or "young trophozoite". -The parasites feeds on the hemoglobin of red cell and enlarge in size. This stage is called "old trophozoite". -The parasite enlarges in size and its nucleus divide into particles 8 -18. Each will acquired part of cytoplasm forming merozoites. The cytoplasm not sharing in merozoite formation is called residual body. This stage is called "Schizont". -The schizont ruptures releaseing merozoites, residual body and pigments into circulation a)Appearance of typical symptoms of malaria The time needed for schizont to mature is 2 -3 d so, symptoms or paroxysm occur by 3 rd or 4 th d according to species b-Some of merozoites will invade new red cells to repeat the erythrocytic cycle, while others begin sexual cycle forming gametocytes Merozoites designed to form gametocytes enter red cell and enlarge forming: *Male gametocyte

Sexual cycle 1 -Gametocyte formation occurs as a part of the erythrocytic cycle. 2 -When a female anopheles feeds on a diseased patient, it will ingest all forms which become digested except gametocytes. 3 -In the stomach of the anopheles, the gametocytes undergo certain changes which are: a)Microgametocytes: -Its nucleus divide into 8 particles. -Pseudopodia are thrown from its cytoplasm. -One nuclear particles will migrate to each pseudopodium. This is called "exflagellation". -The 8 pseudopodia will detached forming microgametes. b-Macrogametocytes: Its nucleus undergoes reduction division and forms only one macrogamete. 4 -Fertilization occurs between macrogamete and one of microgametes forming zygote. 5 -The zygote forms ookinete oocyst. 6 -The nucleus of oocyst divides into thousands of particles each will acquire piece of cytoplasm forming sporozoites. This stage is called sporocyst. 7 -The sporocyst ruptures and sporozoites are carried to salivary glands.

True relapse in malaria: It is reinvasion of blood cells after periods of totally absence of parasites from the blood. Occurs only in P. vivax and p. ovale. Mechanism Some sporozoites become dorminant in the liver cells, these sporozoites are called hypnozoites which in response to internal or external stimuli start a process of schizogony again resulting in re invasion of erythrocytes by the merozoites. Sporozoites of p. malariae and p. falciparum do not share this dormancy phenomena.

P. falciparum Is the most dangerous of the malaria parasites Infects cells of all ages Causes malignant tertian malaria Parasitemia levels are extremely high (Up to 65% of erythrocytes infected) Infected RBCs can attach to uninfected RBCs, forming rosettes, Rosettes can close venules

P. vivax Much more motile than other plasmodium spp. Causes benign tertian malaria Prefer to invade young red cells Cannot penetrate mature red cells � Merozoites can only penetrate RBCs with mediated receptor sites � Receptor sites are genetically determined, conferring resistance A defining characteristic of P. vivax is development of hypnozoites relapse of malarial infection

P. Malariae Has an affinity for mature or older red cells Causes quartan malaria Symptoms appear 18 and 40 days after infection Parasitemia levels are low

P. Ovale Rarest of the four malaria parasites Causes tertian malaria Prefer to invade young red cells Symptoms appear 12 and 18 days after initial infection Difficult to diagnose due to its similarity to P. vivax

Pathophysiology The pathophysiology of malaria results from: 1 - Destruction of erythrocytes. 2 - Liberation of the parasites & erythrocytes material into circulation and host reaction to these events. 3 - Erythrocytes sequesteation in microcirculation of vital organs interfering with microcirculatory flow (P. falciparum)
 which mediate paroxysm symptoms")
1 -Toxicity cytokines Malaria parasite release cytokines (e. g TNF) which mediate paroxysm symptoms (Fever, malaise, shivering) 2 -Sequestration the process where erythrocyte containing P. falciparum adhere to microvascular endoth. (cytooadherance), thus disappear from circulat. Occur in venules of vital organs (brain, heart liver, kidney, intestine ) Sequestration and resetting phenomina lead to obstruction of microcirculation
High MW parasites-derived protein termed P. falciparumerythrocyte membrane protein I.")
3 -Cytoadherance Mediated by: a)High MW parasites-derived protein termed P. falciparumerythrocyte membrane protein I. b)Altered cell membrane components 4 -Rosetting Erythrocyte containing mature parasites also adhere to uninfected erythrocyte leading to formation of rosettes. Rosetting in p. falciparum is associated with cerebral malaria.

5 -Deformability As the parasite matures inside the erythrocyte, the normally flexible biconcave disc becomes more spherical and rigid. 6 -Permeability There is mild generalized increase in systemic permeability in severe malaria 7 -Immunological processes
Non specific symptoms (influenza-like) : Headache, muscular pain, lethargy, lassitude. 2)Fever (paroxysm):")
Clinical Maifestation 1)Non specific symptoms (influenza-like) : Headache, muscular pain, lethargy, lassitude. 2)Fever (paroxysm): Ruptured schizont release pyrogens secretion by leucocytes fever Classical stages of fever: Each paroxysm has 3 successive stages. a-Cold stage: (1 -2 hours) b-Hot stage: (2 -4 hours) c-Sweating stage: - (2 -4 hours) cytokines
 Sense of sever coldness with rigors. Skin is cold")
a-Cold stage: (1 -2 hours) Sense of sever coldness with rigors. Skin is cold and blue. pulse is rapid & weak b-Hot stage: (2 -4 hours) The patient feel very hot. Intense headache, thirst Face, hand, skin, are congested. Pulse is full and rapid. Temp. is high for few hours then begin to falls.
 The patient sweat. Temp. falls rapidly to normal. Patient")
c-Sweating stage (2 -4 hours) The patient sweat. Temp. falls rapidly to normal. Patient are exhausted a tend to sleep and become symptom free until the next attack. Paroxysm occur every: 24 h → (p. falciparum) 3 rd day (48 h) → tertian M (p. vivax) 4 th day (72 h) → quaratan M (p. malariae)
Anaemia: Hemolytic in type. Most marked in p. falciparum due to. a- Higher parasitemia")
3)Anaemia: Hemolytic in type. Most marked in p. falciparum due to. a- Higher parasitemia b- It attack all ages of erythrocytes even unparasitized RBCs 4)Splenomegaly: The spleen enlarged in all forms of acute M. 2 ry hypersplenism (in repeated attaks)
Jaundice: Hemolytic, hepatcellular, cholestatic. Deep jaundice occur in P. falciparum 6)Malarial dysentery: Occur in")
5)Jaundice: Hemolytic, hepatcellular, cholestatic. Deep jaundice occur in P. falciparum 6)Malarial dysentery: Occur in P. falciparum. Due to intest. infarction 2 ry to intest. sequstration

7 -Relapse: Occurs in P. vivax and p. ovale. Occur weak, month or years after the 1 ry infect. Results from maturation of persistent hypnozoites in liver. 8)Recrudesence: Occurs in P. falciparum and P. Malariae. It is renewed manifestation of M. with appearance of parasitaemia. Small number of erythrocytic parasites survived the development of host antibodies and multiply explosively again and induce a clinical attack of malaria.
Malaria In pregnancy a)In areas of intense transmission: Usually asymptomatic 1 - Anaemia. 2")
9)Malaria In pregnancy a)In areas of intense transmission: Usually asymptomatic 1 - Anaemia. 2 - Reduction in birth weight b)In areas with less transmission. Symptomatic disease occur -Mothers at risk of developing severe falciparum infection esp. in 2 nd & 3 rd trimester. Reduction in birth weight& Fetal loss Maternal mortality is high. Pulmonary edema and hypoglycemia are common
Malaria in children: In infancy: Severe falciparum M is rare, when it occurs ,")
10)Malaria in children: In infancy: Severe falciparum M is rare, when it occurs , mortality is high. In childhood: Predominant manifestation of severe M is cerebral malaria. Coma, convulsion. Severe anaemia. Lactic acidosis. Hypoglycemia. Aspiration pneumonia is a lethal sequel.

Severe malaria Definition of severe falciparum malaria by WHO: 1 - Unarousable coma 2 - Convulsion 3 - Severe bleeding abnormalities 4 - Severe anaemia (normochromic, normocytic) 5 - Hypotension/shock 7 - Hypoglycaemia 8 - Haemoglobinuria 9 - Acidemia 0 - Renal failure 10 -Pulmonary oedema/ARDS

CEREBRAL MALARIA Dif: Unrousable coma in patients with falciparum M. (no response to painful stimuli) The most prominent feature of severe falciprum M Clinical features: 1 -The patient is febrile, warm, dry, unrousable. 2 - Anaemia (profound in children) 3 -Sinus tachycardia. 4 -Eye: Pupils: mid sized & reactive Fundus: retinal hage 5 -Resistance to hand flexion. 6 -Positive Babiniski sign 7 -Cranial nerves abnormalities ( rare) 8 -Muscle tone may or ↓↓ or normal.

Complication of malaria 1 -Black water fever: Acute condition caused by p. falciparum infection Ch. by fever, hemoglobulinuria, bilriubinuria, oliguria or even anuria. (port wine or coca colored urine ) It is due to severe intra vascular hemolysis renal ischemia ATN C/P: Fever , Rigors , Vomiting , Jaundice.

3 -Hypotension: High COP, low systemic vascul. resist. , low Bl. P Sudden hypotension and shocked may occur, "algid malaria". Orthostatic hypotension is common 4 -Acute pulmonary oedema: Developed at any time during severe falciparum M More in pregnant women & rare in children. 5 -Acute renal failure:
:")
Chronic complications of malaria. I Immune disorders in malaria 1 -Malarial nephrosis (Quartan nephropathy): An intractable nephrotic syndrome with p. malariae infection Antigen–antibody complex is bound firmly to the glomerular basement membrane. Clinical features: 1 -Asymptomatic proteinuria. 4 -Anaema 2 -Nephrotic syndrome 5 Hepatosplenomegaly 3 -Renal failure Treatment: 1 -Anti malarial do not prevent progression.

2 -Hyper-reactive malarial splenomegaly "Tropical splenomegaly syndrome" Dif: Marked splenomegaly in P. falciparum infection. Pathology: 1 - Splenomegaly with normal architecture. 2 - Lymphocytes infiltration of hepatic sinusoids 3 - Kupffer cell hyperplasia. 4 - Hypersplenism→ anaemia, leucopenia, thrombocytopenia 5 - Hypergamaglobulinaemia & high titers of Ig. M.

Clinical features: 1 - Abdominal swelling 2 - Dragging pain in the abdomen. 2 - Acute left sided abdominal pain suggests splenic infarction. 3 - Liver is also enlarged. 4 - Anaemia & pancytopenia (hypersplenism). Treatment: 1 -Antimatarial → spleen &liver return to normal. 2 -Splenectomy in case of hypersplenism

3 -Immunosuppressive effects 4 -Burkitt’s lymphoma: The immunosuppressive effects of malaria may account for the tendency of the Epstein–Barr virus to produce Burkitt’s lymphoma

DIAGNOSIS OF MALARIA I-Clinical diagnosis: Malaria is suspected in every patient in endemic area with: a) PUO b) Typical periodicity c) Splenomegaly (most clinical sign) II-Direct method: Blood film: Thin or thick film stained by Giemsa or leishman's stain to see different stage inside RBC

III-Indirect methods: 1 -Therapeutic test: Non subsidence of symptoms after administ. of anti M. drugs for 3 days → not malaria. 2 -Serology: Not used in acute attack. Antibodies may be detectable for several years after the last attack of malaria. The most frequently used is indirect fluorescent antibody test (IFAT), ELIZA
 technique: The parasitized erythrocytes have different specific")
IV-New methods: 1 -Quantitative buffy coat (QBC) technique: The parasitized erythrocytes have different specific gravity from unparasitized red cells and can be looked for in a particular segment of blood in a centrifuged capillary tube. 2 -Dipstick methods: The parasite antigens are detected by placing drop of blood on a dipstick impregnated with antibody. 3 - PCR:

Prophylaxis of malaria for travelers Suppressive prophylaxis -Chloroquine, proguanil, mefloquine, and doxycycline, -They are only effective at killing the malaria parasite once it has entered the erythrocytic stage (blood stage). -Therefore have no effect until the liver stage is complete. -So, must be taken for four weeks after leaving the area of risk. Causal prophylaxis -Primaquine, Atovaquone-proguanil -They target blood stages of malaria, and initial liver stage -So, can be stopped 7 days after leaving the area of risk

Mefloquine: used widely because it has a long half-life -one tablet 250 mg /week for two weeks prior to travel -one tablet / week during travel - one tablet for 4 weeks upon return home Doxycycline: for individuals unable to tolerate mefloquine and for those traveling to areas where there is mefloquine resistance. -one to two days before travel -continued for 4 weeks after return home. The adult dose is 100 mg once a day. contraindicated in pregnant women and children < 8 years.
 must be taken daily. -two days before travel")
Atovaquone-proguanil 250 mg atovaquone/100 mg proguanil) must be taken daily. -two days before travel -continued during travel -seven days after return home Chloroquine 300 mg once weekly. Pyrimethamine 25 -50 mg twice a week. -start one week before travel -continue for at least 4 weeks after leaving the endemic area. Fansidar If chloroquine resistant P. falciparum is expected one tablet weekly should be added to any of the above regimen.

TREATMENT OF MALARIA Uncomplicated Medication P. vivax , P. ovale Chloroquine: sensitive 1000 mg salt oral loading dose followed by 500 mg salt orally at 6 h, 24 h, and 48 areas Followed by Primaquine 52. 6 mg salt orally every day for 14 d Chloroquineresistant areas Quinine 625 mg salt orally 3 times a day for 7 d plus doxycycline, tetracycline, or clindamycin Followed by Primaquine

Uncomplicat Medication ed P . falciparum Chloroquine- Chloroquine 1000 mg salt oral loading dose followed by 500 mg salt sensitive orally at 6 h, 24 h, and 48 h area Chloroquine- First line resistant Atovaquone-proguanil 250 mg/100 mg, 4 adult tablets orally every day for 3 d area OR Artemether-lumefantrine 20 mg/120 mg, 4 tablets oral starting dose, followed by 4 tablets orally 8 h later, followed by 4 tablets orally twice a day for 2 d OR Quinine 625 mg salt orally 3 times a day for 7 d plus Doxycycline or Tetracycline or Clindamycin Second line: Mefloquine

Treatment of Severe Malaria First line Artesunate : 2. 4 mg/kg IV at 0 h, 12 h, 24 h, and 48 h, then once per day if IV still nessessary plus Atovaquone-proguanil, doxycycline, clindamycin, or mefloquine Second line Quinidine : Loading dose of 10 mg/kg salt IV over 1 -2 h followed by 0. 02 mg/kg/min salt continuous infusion for 24 h Once improved, switch to oral quinine plus Doxycycline or Tetracycline or Clindamyci

MCQ The most dangerous type of plasmodium malaria is: a. P. vivax b. P. ovale c. P. falciparum d. P. malariae

The main method of transmission of malaria is: a. The bite with an infected female anopheles b. Blood transfusion c. Congenital transmission from mother to fetus through placenta. d. Organ transplantation

Which of the following statement regarding malarial nephrosis are not true? a. Is due to antigen antibody reaction bound firmly to the glomerular basement membrane b. Caused by P. falciparum c. Typically associated with nephtoyic syndrome, anaemia, hepatosplenomegaly d. Antimalarial does not prevent progression

Which of the following statement regarding relapse in malaria is not true: a. It is reinvasion of blood cells after periods of totally absence of parasites from blood. b. Occur week, month or year after primary infection c. Occurs only in P. vivax and p. ovale. d. Results from multiplication of small number of erthrocytic parasites which survived the development of the host antibodies.

Which of the following statement regarding black water fever is not true? a. Is due to acute tubular necrosis resulting from severe intra vascular hemolysis. b. Characterized by hemoglobulinuria, bilriubinuria, oliguria. c. Caused by p. malariae infection d. Clinically characterized by fever , rigors , vomiting , jaundice.

The first line of treatment of P. falciparum in chloroquine resistant area is : a. Mefloquine b. Chloroquine c. Primaquine d. Artemether-lumefantrine
- Slides: 51