Major Histocompatibility complex OR MHC HLA genes MHC

Major Histocompatibility complex OR MHC
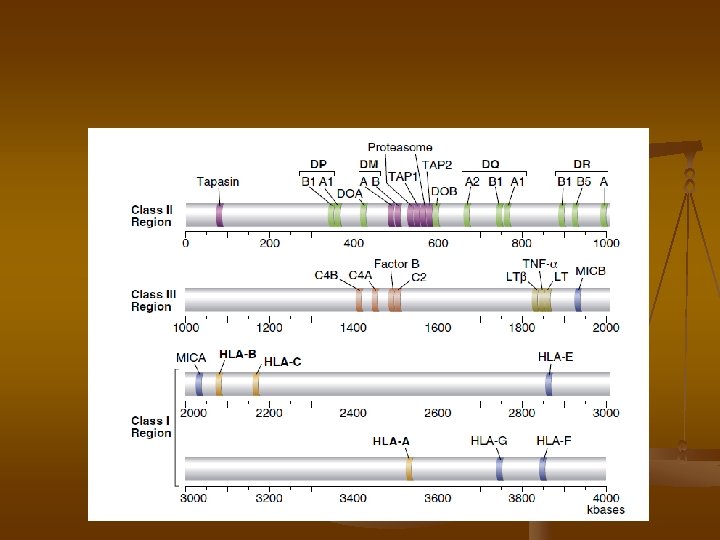

HLA genes MHC locus n n On human chromosome 6 and mouse chromosome 17 HLA class III. are soluble molecules as complement, TNF, HSP and Many other proteins involved in antigen presentation

MHC –I structure


 These are")
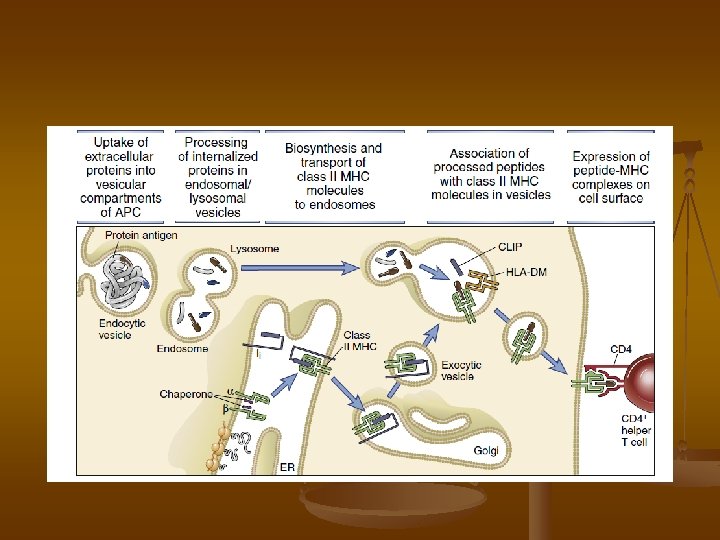
n n HLA-G ( a role in Ag recog. by NK cells) These are present on fetal cells at the maternal-fetal interface and are credited with inhibiting rejection by maternal CD 8 T cells by protecting the fetus from identification as foreign, which may occur when paternally derived antigens begin to appear on the developing fetus HLA-H (involved in iron metabolism) HLA-DM that facilitates the loading of antigenic peptides into class II MHC molecules. HLA-DO molecules, which are expressed only in the thymus and on mature B cells, have been shown to serve as regulators of class II antigen processing

More interesting facts n n Erythrocytes will adsorb some Class I antigens (B 7, A 28, B 57…. ) HLA B most polymorphic system and studies have shown is most significant followed by A and then C

ﻭ ﺑیﻤﺎﺭیﻬﺎ HLA ﺍﺭﺗﺒﺎﻁ Some HLA alleles occur at a much higher frequency in people suffering from certain diseases than in the general population. Such a comparison allows calculation of an individual’s relative risk (RR). n The diseases associated with particular MHC alleles include: autoimmune disorders, certain viral diseases, disorders of the complement system, some neurologic disorders, and several different allergies. frequency of disease in the allele+ group RR = frequency of disease in the allele - group n

HLA and diseases

It has not yet been possible to show the molecular mechanisms underlying disease association with particular HLAmolecule(s). This is because of several reasons. First, it has often been difficult to unequivocally ascertain the primary disease-risk HLA gene(s) because of the existence of extended linkage disequilibrium (LD) within the HLA region. Moreover, HLA-associated diseases can be the result of the combination of different HLA molecules expressed at various loci (class-I and/or class-II) rather than the result of one HLA variant only. Second, the situation has been complicated by the fact that nearly all HLA-associated diseases are multifactorial polygenic diseases in which particular HLA allele(s), in combination with other genetic variants and environmental factors, is involved in disease susceptibility. Third, in most cases, disease-relevant autoantigen(s) are largely unknown, which prevents a thorough three-dimensional analysis of HLA–peptide interactions. Last, human autoimmune diseases are phenotypically extremely heterogeneous, in terms of clinical presentation, age at onset, association with other autoimmune disorders, and severity or rapidity of evolution, and it is likely that different alleles, or allelic combinations at different loci, will predispose to different forms of the disease.

Defining the Role of the MHC in Autoimmunity n n n The mechanisms underlying MHC association in autoimmune disease are not clearly understood. One long-held view suggests a breakdown in immunological tolerance to self-antigens through aberrant class II presentation of self or foreign peptides to autoreactive T lymphocytes. Thus, it seems likely that specific MHC class II alleles determine the targeting of particular autoantigens resulting in disease-specific associations. Other hypotheses have also been offered to account for a direct role of particular MHC alleles in disease susceptibility. In some rare cases, certain allelic forms of MHC genes can encode molecules that are recognized as receptors by viruses or bacterial toxins, leading to increased susceptibility in the individuals who inherit these alleles

The existence of an association between an MHC allele and a disease should not be interpreted to imply that the expression of the allele has caused the disease. The relationship between MHC alleles and development of disease is more complex, partly thanks to the genetic phenomenon of linkage disequilibrium. If, for example, DR 4 contributes to risk of a disease and it also occurs frequently in combination with HLA-A 3 because of linkage disequilibrium, then A 3 would incorrectly appear to be associated with the disease In the case of HLAB 57 and AIDS progression, the allele has been linked more directly to disease. It is believed that this class I allele is particularly efficient at presenting important components of the virus to circulating Tc cells, leading to increased destruction of virally infected cells and delayed disease progression.
 n Indeed, 90– 95% of patients with AS are positive for")
ankylosing spondylitis (AS) n Indeed, 90– 95% of patients with AS are positive for HLA-B 27 compared with less than 10% of healthy subjects, which confers B 27 a high relative risk.

n n The basis for HLA-B 27 association with AS remains unknown. Three theories have been proposed. In the first one – the ‘arthritogenic peptide theory’ – HLA-B 27 would present a microbial peptide epitope and elicit a cytotoxic T lymphocytes response against it, part of which would cross-react with a self antigen epitope leading to autoimmune injury. In the ‘misfolding’ theory, the natural tendency of HLA-B 27 molecules to misfold and accumulate in the endoplasmic reticulum (ER) would induce ER stress, resulting in induction of proinflammatory cytokines. In the last ‘surface homodimer’ theory, covalent B 27 heavy chains homodimers expressed at the cell surface might play an mmunomodulatory role and disturb the normal development of HLA class I-mediated responses.
 n n CD is a complex disorder of the small intestine")
Celiac disease (CD) n n CD is a complex disorder of the small intestine caused by an inappropriate immune response to ingested wheat gluten and similar proteins of rye and barley. It is characterized by villous atrophy, crypt hyperplasia, and lymphocyte infiltrates of the epithelium and lamina propria, which in turn lead to nutrient malabsorption and/or chronic diarrhea. Its estimated prevalence is high (about 1%) , and its only current treatment is a lifelong exclusion of gluten from the diet. CD has a strong genetic component, as illustrated by a monozygotic twin concordance of nearly 90% compared with 10% in first-degree relatives. A significant proportion of the genetic predisposition comes from HLA genes, which are estimated to account for about 50% of the genetic risk. More than 90% of CD patients express the HLA-DQ 2 molecule, and most of the remaining patients carry DQ 8. Thus, HLADQ 2 and HLA-DQ 8 are necessary, but there are not sufficient to predispose to CD (most DQ 2 - or DQ 8 -positive individuals remain healthy)

n The principal disease triggering component of wheat gluten belongs to a family of closely related proline- and glutamine-rich proteins called gliadins. In sharp contrast with virtually all other dietary proteins, prolinerich gliadins are strongly resistant to proteolysis by gastric, pancreatic, and intestinal brush border membrane enzymes so that long gliadin peptides can build up to high concentrations in the small intestine. When genetically predisposed individuals who express. HLA-DQ 2 or DQ 8 are exposed to certain gliadin epitopes, these epitopes are presented on the surface of antigen presenting cells in the lamina propria, which in turn stimulate proliferation of gliadin-specific CD 4 T cells in the mucosa.
- Slides: 27