Machinery and membranes Stefano Picca MD Department of

"Machinery and membranes" Stefano Picca, MD Department of Nephrology and Urology, Dialysis Unit “Bambino Gesù” Pediatric Research Hospital, IRCCS ROMA, Italy

MEMBRANES AND MACHINES : BASIC NEEDS IN CHILDREN Membranes: • Biocompatibility • Filtration and absorption Machines: • Accuracy and precision • Circuit low priming volume • Circuit inner pressures and resistance suitable for small catheters use
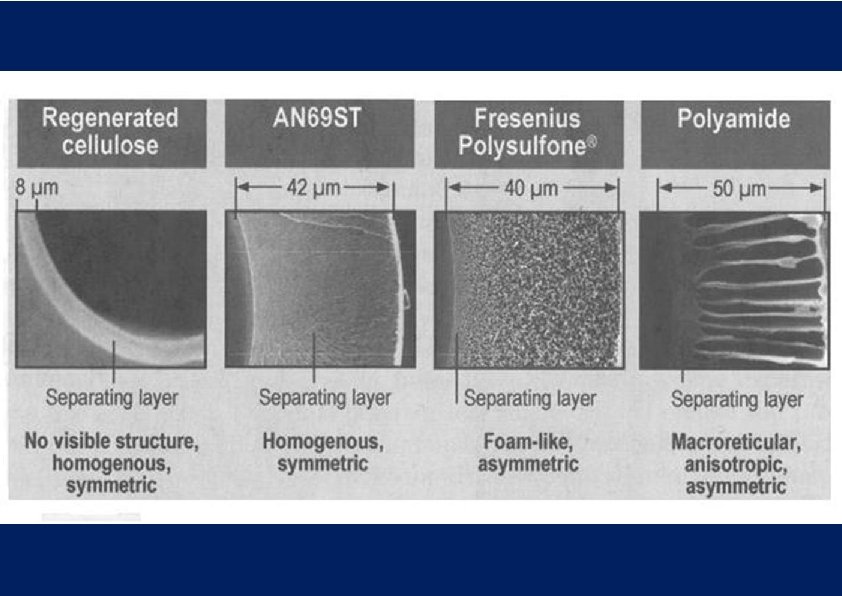
: uniform pores dimension throughout the entire membrane thickness) Asymmetric (anisotropic):")
SYNTHETIC MEMBRANES Symmetric (isotropic): uniform pores dimension throughout the entire membrane thickness) Asymmetric (anisotropic): “skin layer” + highly porous supportive layer Basically: adsorption enhanced Basically: filtration enhanced

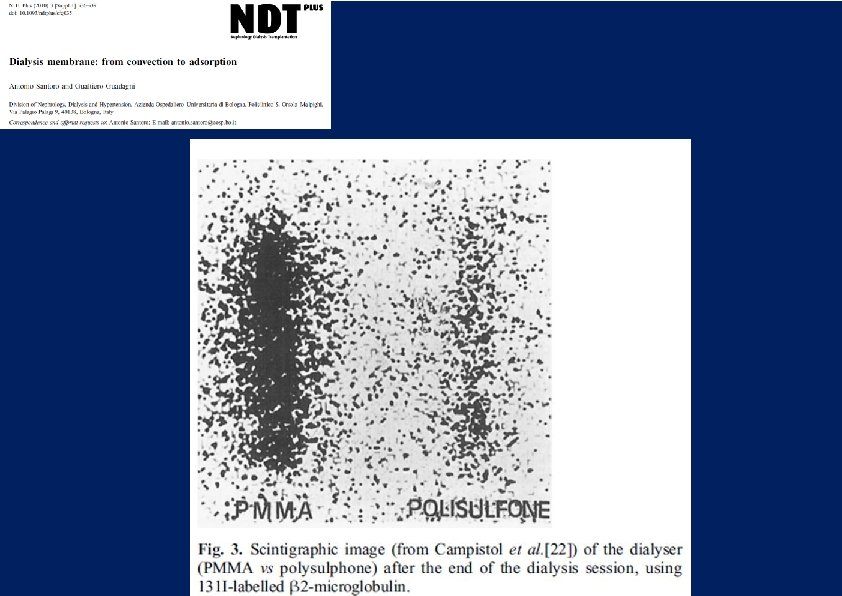
Santoro, 2010

β 2 MICROGLOBULIN REMOVAL TOTAL ABSORPTION CONVECTION Neri, 2012

REMOVAL OF SOLUTES AND MEDIATORS Filter cutoff CONVECTION/DIFFUSION ABSORPTION ß 2 microglobulin myoglobin creatinine urea sucrose ionic compounds 101 inulin IL-8 Vit B 12 102 IL-6 albumin IL-1 103 TNF 104 105 MW (Daltons)

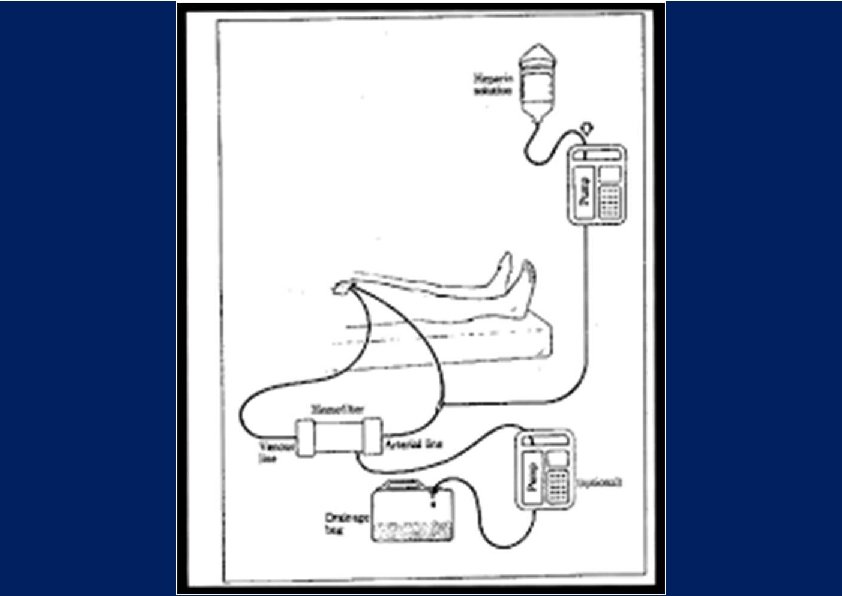
CAVH, 1984 • CVVH: needs: • increase blood flow • manage fluid balance
= error up")
• Error up to 12. 5% • 2 pumps (pre-post filter)= error up to 25%

The real innovation: the load-cell Equaline® Amicon, 1991

Baxter BM 25 Baxter Aquarius Baxter- Gambro Prismaflex
, a high-flux polysulfone 0. 045 m 2 filter")
• Two operating syringes (1), a high-flux polysulfone 0. 045 m 2 filter (2), a heparin syringe (3), pumped dialysate (4), a pressure transducer (5) and an airdetector (6), and self-primes with 4. 3 ml of heparinised saline, giving a minimum operating volume of 9. 3 ml • 5 to 12. 5 ml aliquots of blood from a single-lumen central venous line, passes and returns it across a dialysis filter, and then back to the baby. • At a blood flow rate of 20 ml/min, this processes 5 ml of blood each minute. The circuit has ultrafiltration from 0 to 60 ml/h is precisely controlled in 3. 2 μl steps by differential syringe movements.
: external pump!!!")
Pediatric Nephrology 2016 101 circuits over 12 children Preinfusion replacement (30 ml/kg/h): external pump!!! Specifications: • PRIMING VOLUME 33 ml • Filter 0. 12 m 2 • Qb 10 -40 ml/min • UF pump 0 -500 ml/h


Blood flow and pressure into the blood pump segment of the arterial line are not those measured by the machine 180° 120° flow volume Courtesy of Medtronics-Bellco, modified

OPBG EXPERIENCE -12 neonates -About 32 sessions -50% times 0. 075 m 2 -Weight range 2. 1 -3. 5 kg -CVVH 100% pre -Qb 5 -14 ml/min -Q rep 20 -30 ml/kg/h -NETQuf 10 -20 ml/h -Vasc access 6. 5 F, 4 F or two 20 -24 G cannulas Courtesy of Z. Ricci, modified
 Circuit blood priming volume")
INFANT CRRT CIRCUITS: PRISMAFLEX ® vs CARPEDIEM®: Operational Characteristics (CVVH) Circuit blood priming volume Blood flow rate resolution Blood pressures range: art/ven Max fluid loss/ session (max 24 h) Ultrafiltration (UF) rate (based on FF=20%) UF rate supervision Gravimetric weight supervision accuracy Fluid gravimetric control: max deviation from UF rate and scale control Prismaflex HF 20® (0, 20 m 2) 59 ml 10 -100 ml/min 2 ml -250 +450 ± 15 mm. Hg No limit 120 -1200 ml/h (up to 2500/h) TMP alarm ≤ 7 g ± 20 g immediate (i. e. : clamped bag) or 60 ml/last 3 hrs Gain/loss control Carpediem® (0, 25 m 2) 41 ml 2 -50 ml/min 1 ml -400 + 100 mm. Hg 1000 ml 0 -600 ml/h 20% of Qb 1 g ± 20 g (for exchange< 2 L Carpediem® (0, 147 m 2) 33 ml - - 0 -240 ml/h - - - Carpediem® (0, 075 m 2) 27 ml - - 0 -150 ml/h - - - THE «REAL» DIFFERENCES (i. e. : CLINICAL CONSEQUENCES): Pro-PRISMAFLEX®: Pro-CARPEDIEM®: • In CVVHD: not bound to the CVVH filtration fraction • No mandatory need for blood priming of circuit • Very low and accurate Qb: if malfuncioning CVC…

INFANT CRRT CIRCUITS: PRISMAFLEX ® vs CARPEDIEM®: Clinical management Modalities Anticoagulation Fluid Buffer Heating Catheters Prismaflex HF 20® SCUF CVVHDF Heparin/Citrate Bicarbonate/Lactate Optional 6, 5 F 7, 5 cm Carpediem® SCUF CVVHD Heparin Lactate None 6, 5 F 4 F 20 G THE «REAL» DIFFERENCES (I. E. : CLINICAL CONSEQUENCES): Pro-PRISMAFLEX®: Pro-CARPEDIEM®: • CVVHDF control • Citrate… • Still waiting for Bicar-buffer… • Very small CVC in very small children…


TAKE HOME MESSAGE • Tremendous improvement → • Extraordinary armamentarium now available • Clinical trials to investigate relation between technical advancement and clinical outcome needed

ACKNOWLEDGEMENTS • All Dialysis Unit nurses • Stu Goldstein, Tim Bunchman and Claudio Ronco for precious advices and friendship through the years.

Dialysis Unit, “Bambino Gesù” Pediatric Hospital Roma, Italy. Doctor: S. Picca Headnurse: V. Bandinu Nurses: N. Avari D. Ciullo P. Iovine P. Lozzi L. Stefani P. Vicerè Nurse Coordinator: M. D’Agostino
FILTERS IN NEWBORNS AND CHILDREN: PAST AND PRESENT MANUF. FILTER SURF. (m 2) MEMBR.")
HEMO(DIA)FILTERS IN NEWBORNS AND CHILDREN: PAST AND PRESENT MANUF. FILTER SURF. (m 2) MEMBR. PRIMING (ml) Gambro-Hospal Miniflow 10 0. 045 AN 69 3. 5 Amicon, then Minntech Minifilter 0. 07 Polysulfone 6 0. 075 Polysulfone 27. 2 (circuit) 0. 147 Polysulfone 33. 5 (circuit) 0. 245 Polysulfone 41. 5 (circuit) Bellco Carpediem 1 Bellco Carpediem 2 Bellco Carpediem 3 Baxter-Gambro HF 20 0. 2 Polyarylethersulfone (PAES) 60 (kit) Baxter-Edwards HF 03 0. 3 Polysulfone 38 Baxter-Gambro ST 60 0. 6 AN 69 93 (kit) Baxter-Edwards HF 07 0. 7 Polysulfone 54 Baxter-Gambro ST 100 1. 0 AN 69 149 (kit)

The Alaris Pump module’s instrument accuracy is +/- 5% at rates between 1 and 999 m. L/hr

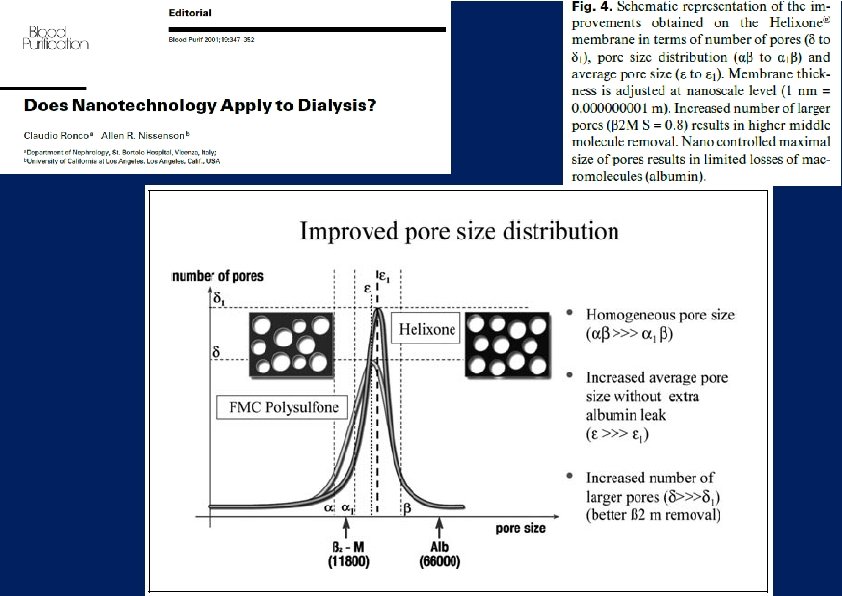
Basis of the Nanostructure of membrane pores Old Synthetic Membranes Other membrane Dead end pore Stenotic pore Improved Synthetic Membr Skin layer Conventional pores: ragged, tortuous below surface Mix of small and large pores Nanocontrolled Membrane Standardized pore structure Nanocontrolled pores: smooth, cylindrical: less resistance

ABSORPTION Electrical Binding Mechanical binding In both cases, absorption depends on: • Qb • Quf • Qd • Surface • Initial concentration Neri, 2012
- Slides: 32