LYMPHOMAS Dr Zahida Qasim MBBS DCP M PHIL
 Associate Prof. Pathology")
LYMPHOMAS Dr. Zahida Qasim MBBS, DCP, M. PHIL (Hematology) Associate Prof. Pathology

Lymphomas • Lymphomas are heterogeneous group of diseases caused by malignant lymphocytes • Arising mainly from lymph nodes or other lymphoid tissue • In their course may infiltrate bone marrow and rarely peripheral blood (lymphoma in leukemic phase).

Lymphomas • All lymphoid neoplasms arise from single transformed cell - monoclonal. • Most lymphoid neoplasms (80 -85%) are of B cell origin • T cell neoplasms comprise 15 -20 % • Tumors of NK cells are very uncommon

ALL CLL Lymphomas MM naïv e B-lymphocytes Lymphoid progenitor AML Hematopoietic stem cell Myeloid progenitor Plasm a T-lymphocytes cells Myeloproliferative disorders Neutrophils Eosinophils Basophils Monocytes Platelets Red cells

B-cell development CLL stem cell lymphoid progenitor mature naive B-cell germinal center B-cell MM progenitor-B ALL memory B-cell pre-B immature B-cell DLBCL, FL, HL plasma cell

Lymphoma Hodgkin’s lymphoma Non Hodgkin’s lymphoma

Key 2 UHS: Q 5, Pg 23


Risk factors for Lymphomas • Immunosuppression or immunodeficiency • Connective tissue disease • Family history of lymphoma • Infectious agents (Particularly viral infections) • Ionizing radiation

Clinical manifestations: • Can present at any age, Rare in children, Bimodal peak common (3 rd decade and elderly) • Male to female ratio 2: 1 • Most patients present with painless, non-tender , asymmetrical , firm , discrete and rubbery enlargement of superficial LN. Cervical LN. . 60 -70% Axillary LN. . 10 -15% Inguinal LN. . . 6 -12%

Cervical Lymphadenopathy in a case of Hodgkin’s Lymphoma

§ Clinical splenomegaly occurs during the course of disease in 50% cases §. Involvement of mediastinum is seen in 6 – 11%. § Liver involvement may also occur. § Extra-nodal sites relatively uncommon except in advanced disease • Marrow infiltration……. Bone marrow failure.

§ Constitutional symptoms are prominent in patients with widespread disease. These include: § Fever. . . . In about 30% cases (is continuous or cyclic) § Pruritus. . . occurs in around 25% cases (often severe) § Alcohol induced pain in areas where disease is present (occurs in some patients) § Other constitutional symptoms include weight loss, profuse sweating, (specially at night), weakness, fatigue, anorexia and cachexia

Difference between Key to UHS, Q 16, Page 28 Hodgkin’s lymphoma Non Hodgkin’s Lymphoma • Localized to single group of lymph nodes (cervical & Mediastinal) • RS cells present • Contagious spread • Fever • Mesenteric nodes and Waldeyer’s nodes rarely involved • Extranodal involvement rare • Usually responds to treatment • Involvement of multiple peripheral lymph nodes • RS cells absent • Spread is not contagious • No fever. • Mesenteric nodes and Waldeyer’s nodes commonly involved • Extranodal involvement common • Response to treatment is not good/bad prognosis

Diagnosis: 1. Hematological and Biochemical findings • Normocytic and normochromic anemia …. common • Eosinophilia is common • 1/3 rd of patients have leukocytosis. • Advanced disease……. . leucopenia and loss of cell mediated immunity • Platelet count normal or increased in early stages/ decrease in later stages. • ESR and C-reactive proteins …. . Usually raised (are useful markers in monitoring disease progress) • Serum LDH is raised in 30 -40% of cases • Elevated levels of transaminases may indicate liver involvement

2. Diagnosis confirmed on Trephine Biopsy (bilateral trephine biopsy may be required in some cases) 3. Radiological: • Chest X-Ray • CT Thorax, Abdomen, Chest , Pelvis 4. Special tests : • MRI • Bone scan • Gallium scan • PET Scan • Lymphangiography

Clinical staging of Hodgkin and Non-Hodgkin Lymphoma Key to UHS, Q 2, Pg 21 Ann Arbor modified by Cotswolds • Stage I: Involvement of single lymph node region(1) or involvement of single extra lymphatic organ or tissue (1 E) • Stage II: Involvement of two or more lymph node regions on same side of diaphragm (II) or involvement of limited contiguous extra lymphatic organ(IIE) • Stage III: Involvement of lymph node regions or structures on both sides of diaphragm(III) which may include spleen (IIIS), limited contagious extra lymphatic organ (IIIE) or both (IIIES) • Stage IV: Involvement of extra nodal site(s) with or without lymphatic involvement A. Asymptomatic B. Symptomatic (B symptoms) X. Bulky disease ( > 1/3 widening of mediastinum, > 10 cm max. dimension of nodal mass) E. Extranodal involvement

Staging of lymphoma Stage III Stage IV A: absence of B symptoms B: fever, night sweats, weight loss

Prognosis: Key to UHS, Q 7, Page 23 • Prognosis depends upon stage: Stage I & II have better prognosis while stage III & IV have bad prognosis. • Risk factors for poor prognosis are: • Age greater than 60 • Late-stage disease • Elevated LDH levels • Impaired performance status • Bone marrow involvement
")
Hodgkin lymphoma Thomas Hodgkin (1798 -1866)

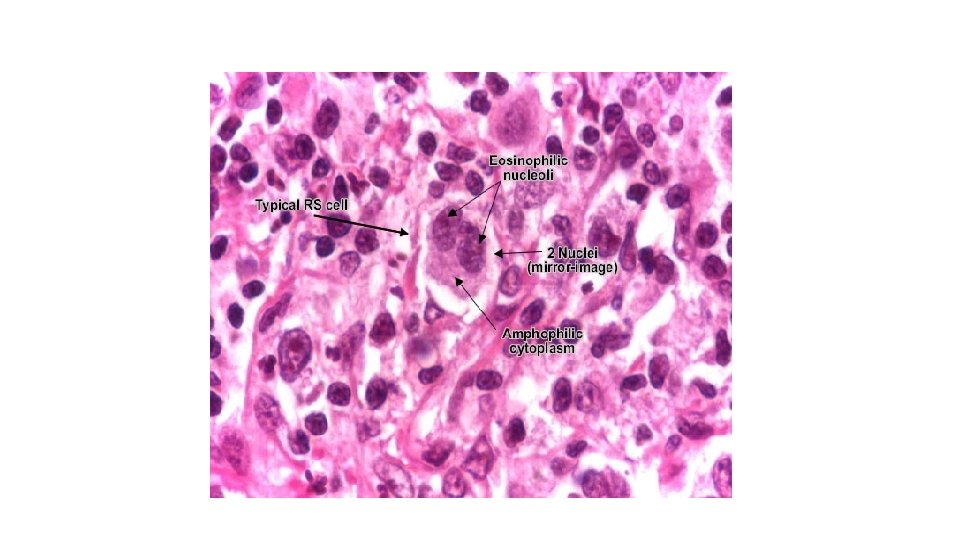
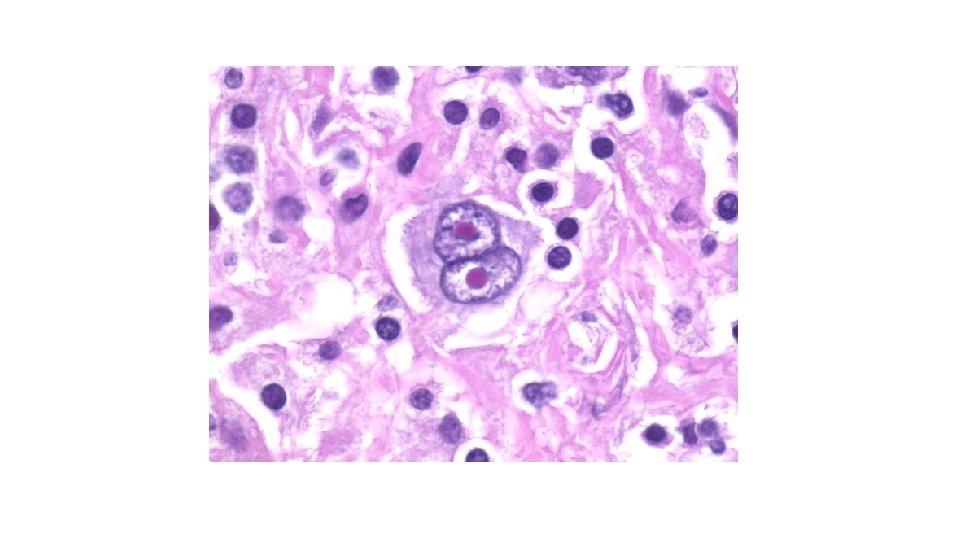
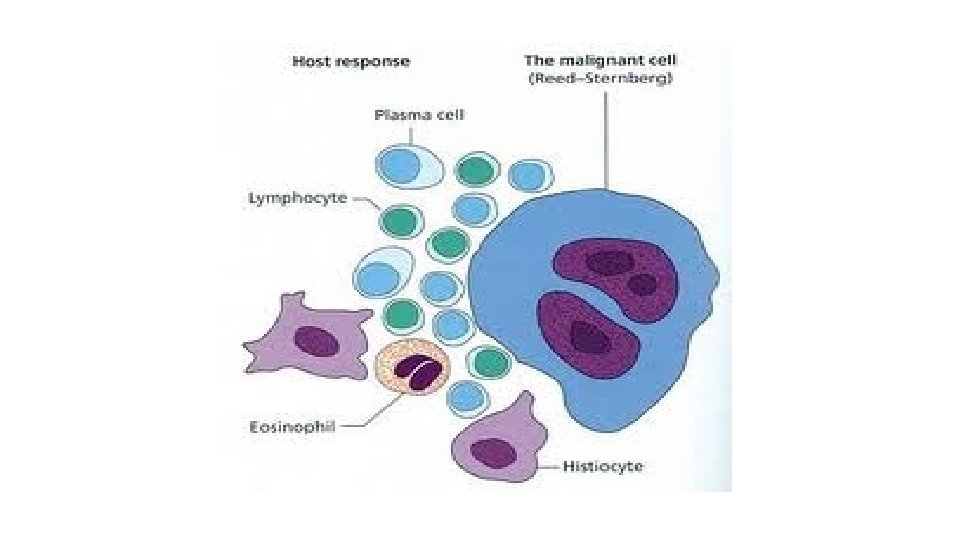
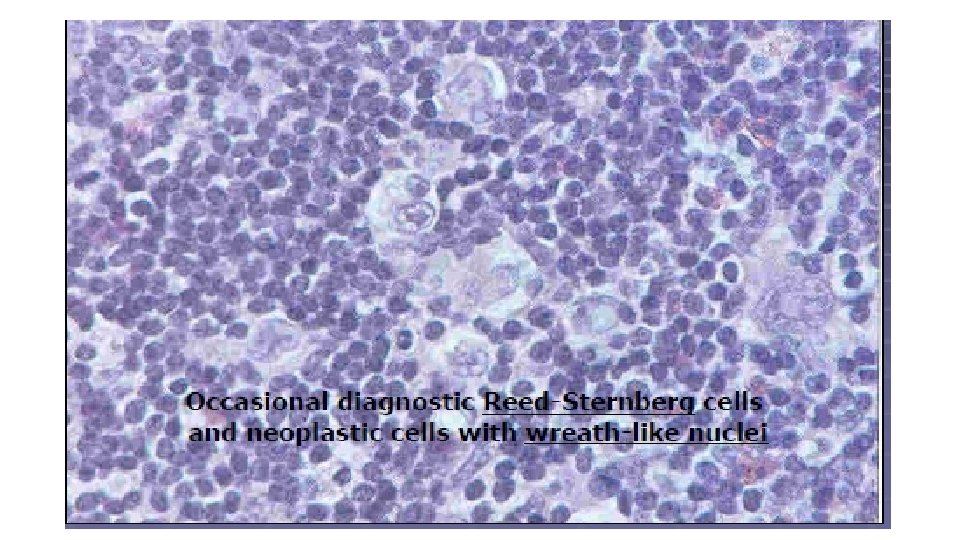
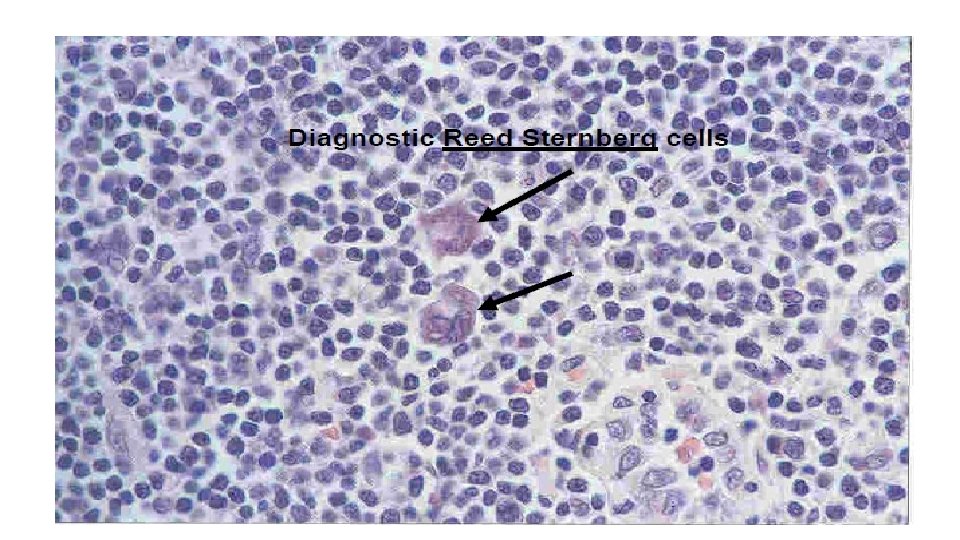
HODGKINS’ LYMPHOMA Key to UHS, Q 2, Page 21 Ø Hodgkin’s lymphoma is a malignant lymphoma which is Key to UHS, Q 7, Page 23 recognized by the presence of its pathagnomonic cell labelled as “Reed Sternberg cell”, along with inflammatory cells which are reactive. Reed - Sternberg cell is a relatively large cell that typically have a bilobed nucleus(Owl Eye) with prominent eosinophilic nucleoli which are mirror images of eachother separated by a clear space from a thickened nuclear membrane.

Key to UHS, Q 2, Page 21 Reed – Sternberg Cell High power view of lymph node Biopsy showing two multinucleate Reed – Sternberg cells, one with a characteristic “Owl Eye” appearance, surrounded by lymphocytes, histiocytes and eosinophils. Markers are CD 15 & CD 30.
 • Hodgkin")
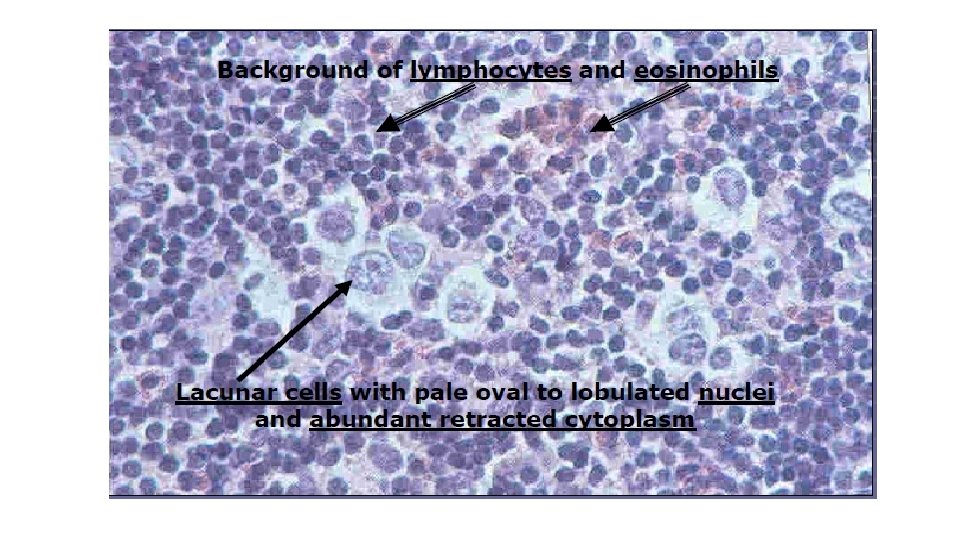
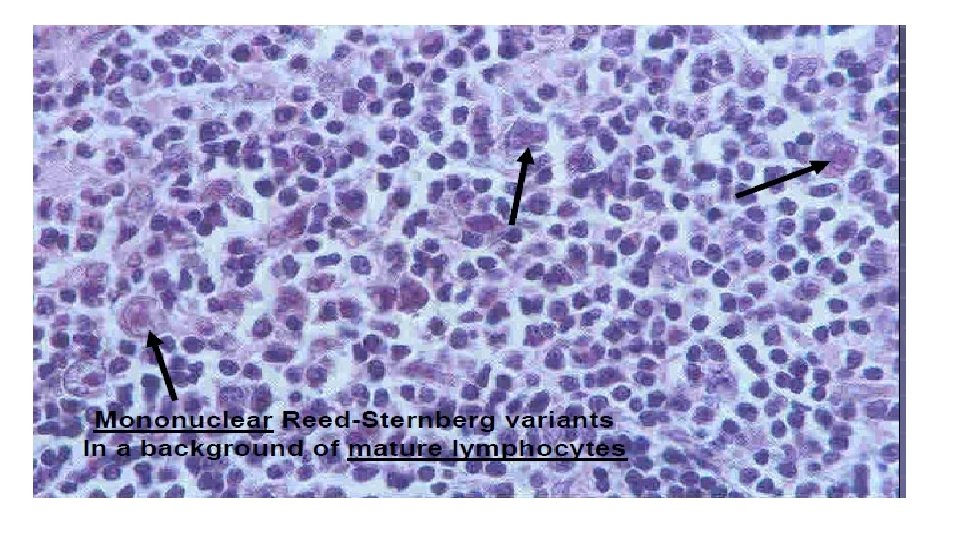
Diagnostic Malignant cells*** • Classic Reed-Sternberg RS cell (CD 15, CD 30) • Hodgkin cell HC • Lacunar cell LC • Lympho-histiocytic L&H or popcorn cell

RS cell and variants Classic RS cell lacunar cell Popcorn cell

Reed-Sternberg Cell Popcorn cell variant • Described 1898 Sternberg, 1902 Reed
 EBV? loss of apoptosis cytokines germinal centre")
A possible model of pathogenesis Transforming event(s) EBV? loss of apoptosis cytokines germinal centre B cell RS cell inflammatory response

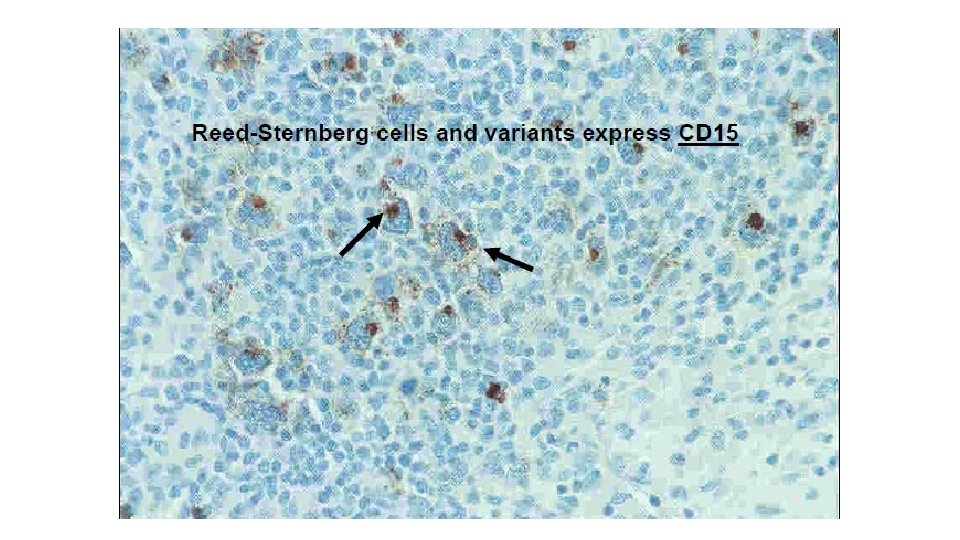
Key to UHS, Q 2, Page 21 Histological subtypes of Hodgkin’s Lymphoma: Key to UHS, Q 6, Page 23 Key to UHS, Q 16, Pge 28 A. Classical Hodgkin’s lymphoma (CHL) • Nodular Sclerosis (NS) (CD 15+, CD 30+), EBV – • Mixed Cellularity (MC) (CD 15+, CD 30+), EBV 70% + • Lymphocytic Rich (LR) (CD 15+, CD 30+), EBV 40% • Lymphocytic Depletion (LD) (CD 15+, CD 30+), EBV most+ B. Nodular Lymphocytic Predominance CD 20+, (CD 15 -, CD 30 -, EBV –) (NLP)

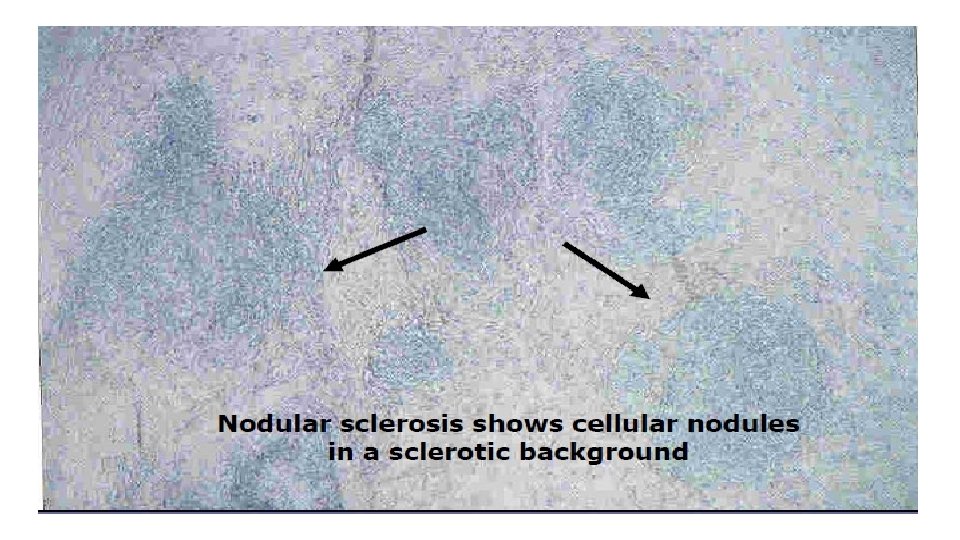
Nodular sclerosis HL Key to UHS, Q 14, Page 28 § Multiple nodules • Fibrous bands (collagen bands extend from node capsule to encircle nodules of abnormal tissue). • Lacunar cells (Variant of RS cell) is often found • The cellular infiltrate may be of lymphocyte predominant, mixed cellularity or lymphocyte depleted type. • Eosinophilia is common

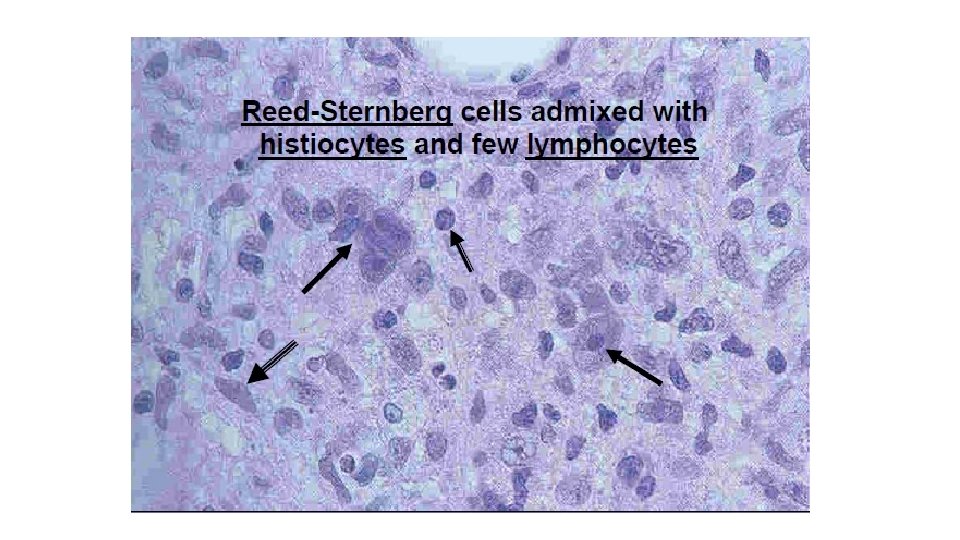
Mixed Cellularity Key to UHS, Q 14, Page 28 Key to UHS, Q 16, Page 28 • Classic RS cells some lacunar or Hodgkin’s cells • Diffuse cellular infiltrate of mature lymphocytes, histiocytes, eosinophils, neutrophils and plasma cells • Hodgkin’s cells are = CD 15 + CD 30 +
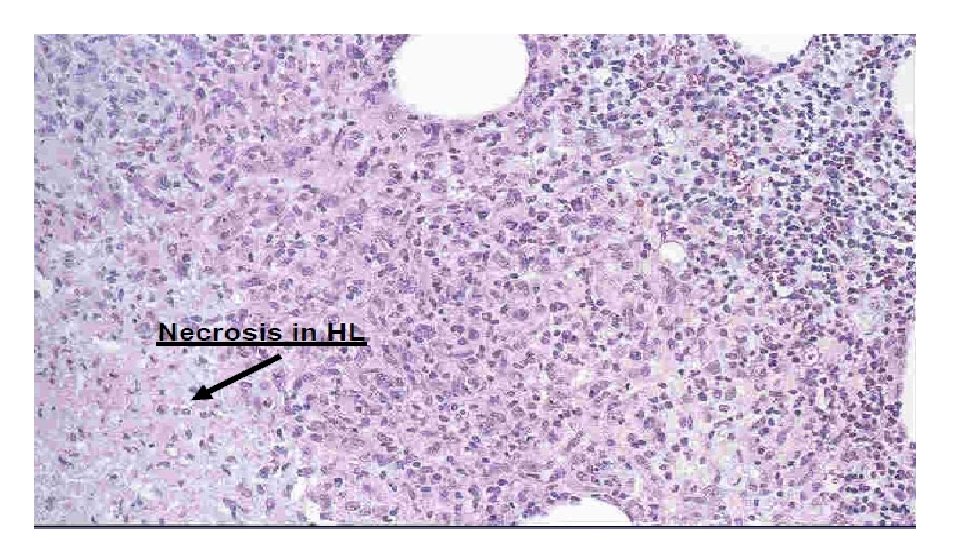

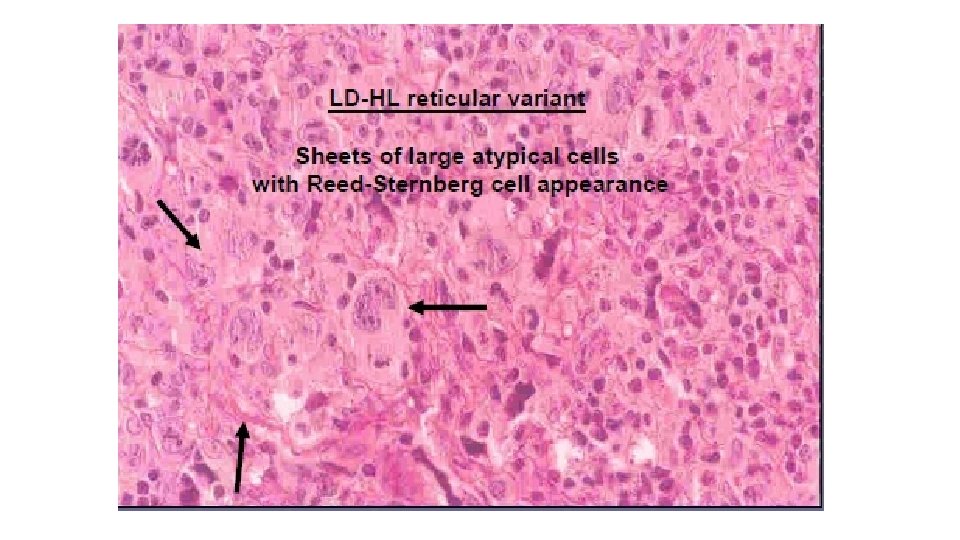
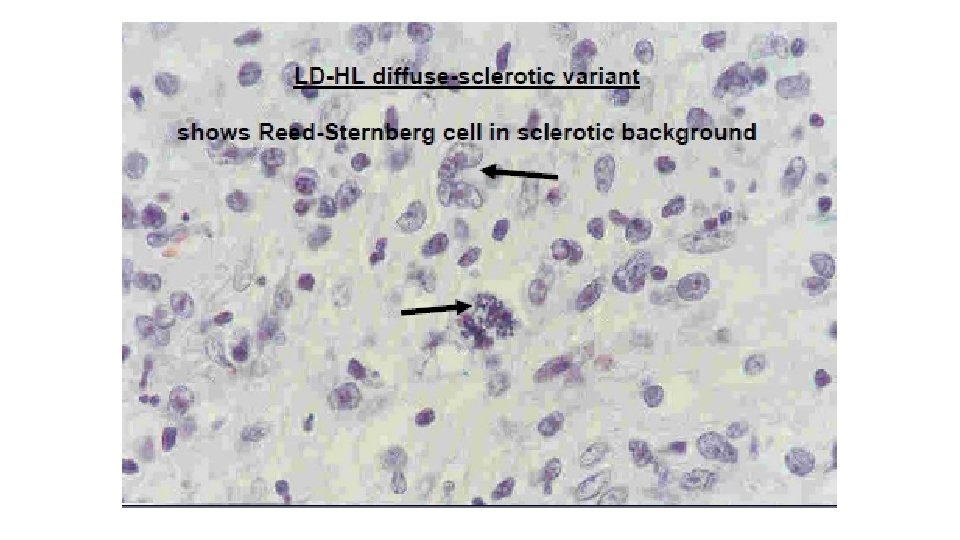
Lymphocytic depleted HL • Hypocellular infiltrate • Diffuse fibrosis or necrosis/ Reticular pattern • Large numbers of Reed-Sternberg cells • Paucity of inflammatory cells. • Lymph node may be replaced by disordered connective tissue with scanty lymphocytes Key to UHS, Q 14, Page 28

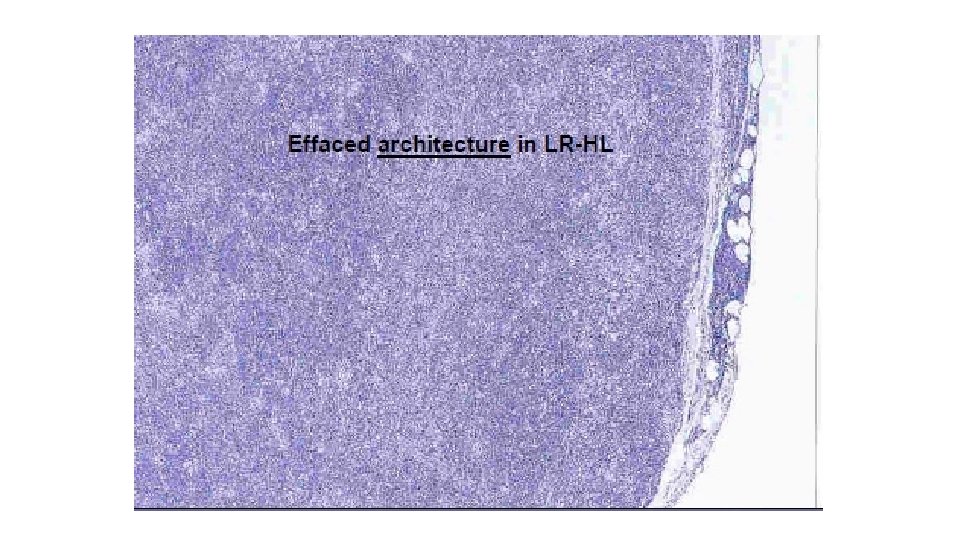
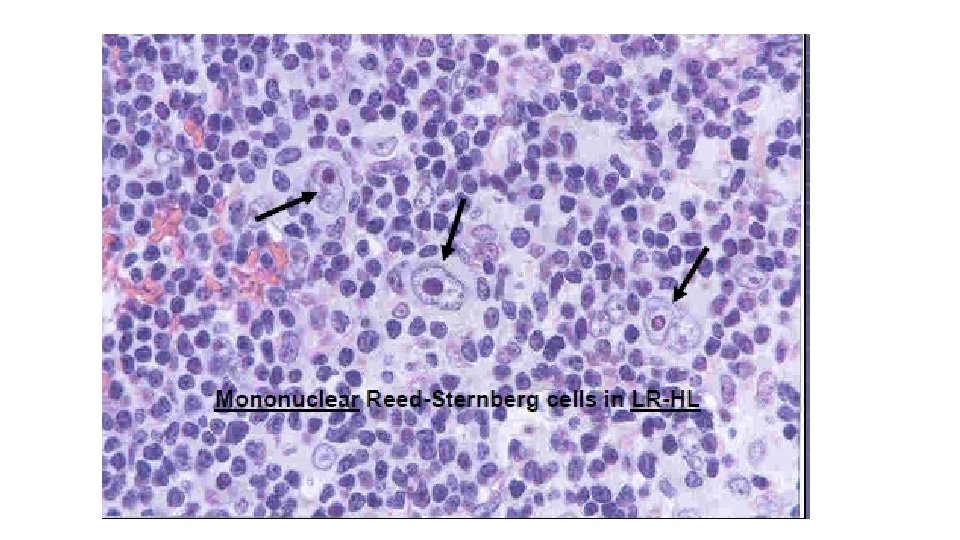
Lymphocytic Rich HL Key to UHS, Q 14, Page 28 Scanty RS cells , multiple small lymphocytes with eosinophils and plasma cells. • Nodular or Diffuse cellular proliferation • Infrequent RS cells

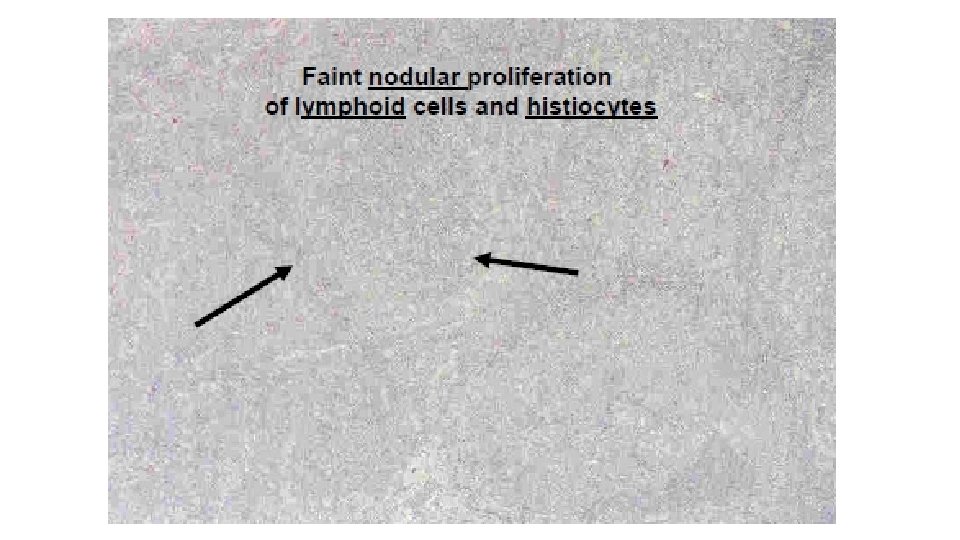
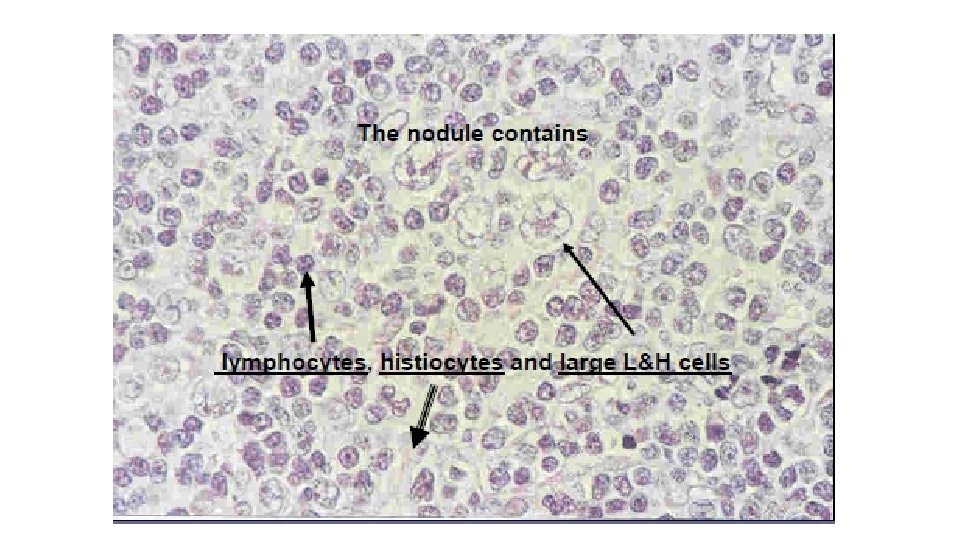
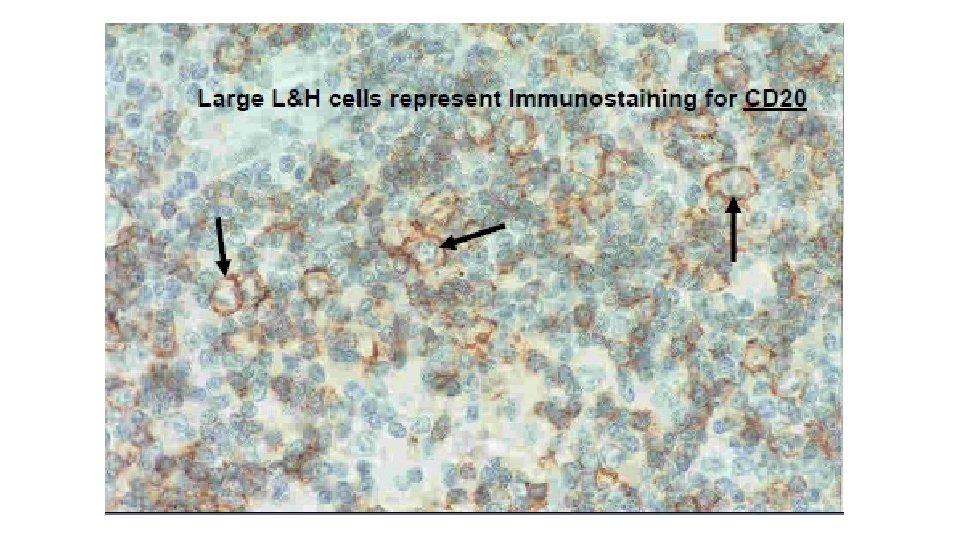
Lymphocyte Predominant Nodular HL • RS cells absent • Abnormal polymorphic B cells (lymphocytic or histiocytic ) present • CD 15 & CD 30 Negative • CD 20 +ve Key to UHS, Q 14, Page 28

SEQs: • Q. subtypes of HL? What is RS cell? Give Staging of HL& NHL. Give Histological sub types with Immunological markers of HL? • Tabulate the clinical differences b/w Hodgkin’s & Non H L? • Give causes of generalized Lymphadenopathy? Tabulate Difference between Lymphadenopathy in TB VS Lymphoma • Classify Non HL, What are Lacunar cells? • Classification of Peripheral B cell neoplasm & molecular genetics of follicular Lymphoma. • What is Burkitt’’s lymphoma?

Clinical cases: Key to UHS, Q 6, Pge 23 • Case 1: 30 y/M with 2 mon Hx of dyspnoea describes intermittent chest pain e alcohol consumption. CT chest shows mediastinal lymphadenopathy. Biopsy of the lymph node shows large binucleate cells e prominent nucleoli, lymphocytes & occasional plasma cells. 1. Dx? 2. Give histological subtypes e immunological markers.

Clinical cases: Key to UHS, Q 7, Pge 23 • Case 2: A mass lesion was detected in anterior mediastinum of a 35 year old lady on CT chest. Biopsy revealed few binucleate cells with prominent nucleoli scattered amongst a population of mixed inflammatory infiltrate. Fibrous septa were also present dividing the cellular infiltrate into nodules. 1. Dx? 2. Describe detailed morphology and discuss prognosis.

Home work: • Question 1 Key to UHS, Q 12, Page 26 • Question 2 Key to UHS, Q 18, Page 31 • Question 3 Key to UHS, Q 20, Page 32 • Question 4 Key to UHS, Q 5 (part B), Page 23

- Slides: 56