LUTS assessment and management Ahmed Ibrahim Urology Department

LUTS assessment and management Ahmed Ibrahim Urology Department Peterborough City Hospital May 2019

The Burden

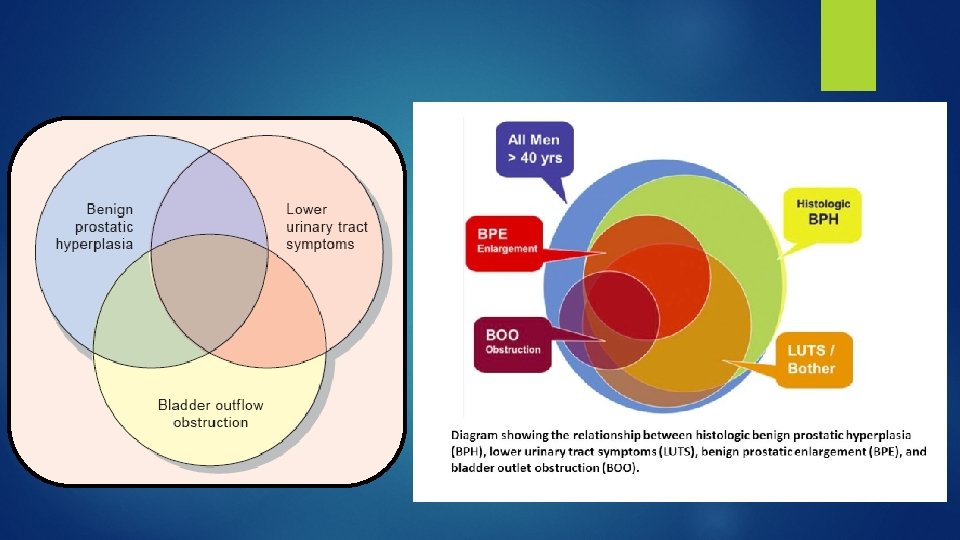
Pathophysiology

• Men with moderate-to-severe LUTS may have an increased risk of major adverse cardiac events � Gacci, M. , et al. Male Lower Urinary Tract Symptoms and Cardiovascular Events: A Systematic. Review and Meta-analysis. Eur Urol, 2016. 70: 788.

Complications

DDX

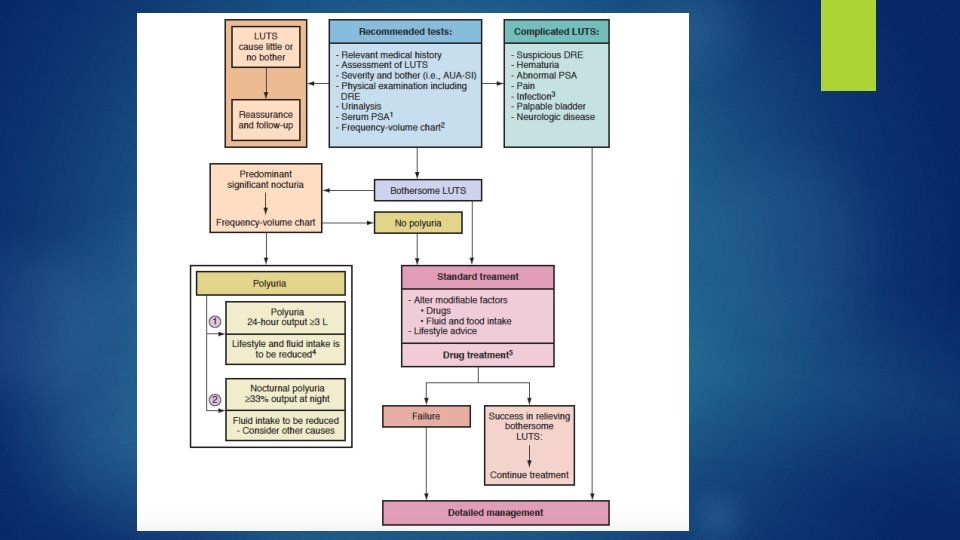
Evaluation A- History : 1 - Identify potential causes and relevant comorbidities, including medical and neurological diseases, current medication, lifestyle habits. � 2 - Address the patient’s concerns : § Prostate cancer ? § Progression ? § AUR ? § Therapeutic options ? Ø 3 - Self-completed validated symptom questionnaire : IPSS , FVC , IIEF. �
 questionnaire � This questionnaire contains seven symptom questions and")
International Prostate Symptom Score (IPSS) questionnaire � This questionnaire contains seven symptom questions and one quality of life (Qo. L) question. “mildly symptomatic” (1 -7 points) “moderately symptomatic” (8 -19 points) “severely symptomatic” (20 -35 points). � Limitations • The IPSS is not suitable to assess incontinence and post-micturition symptoms. • The IPSS questionnaire does not differentiate bother caused by each separate symptom.

B- Physical Examination � Suprapubic area. � External genitalia: Urethral discharge, meatal stenosis, phimosis � DRE � lower limbs � Neurological examination C- Urine analysis

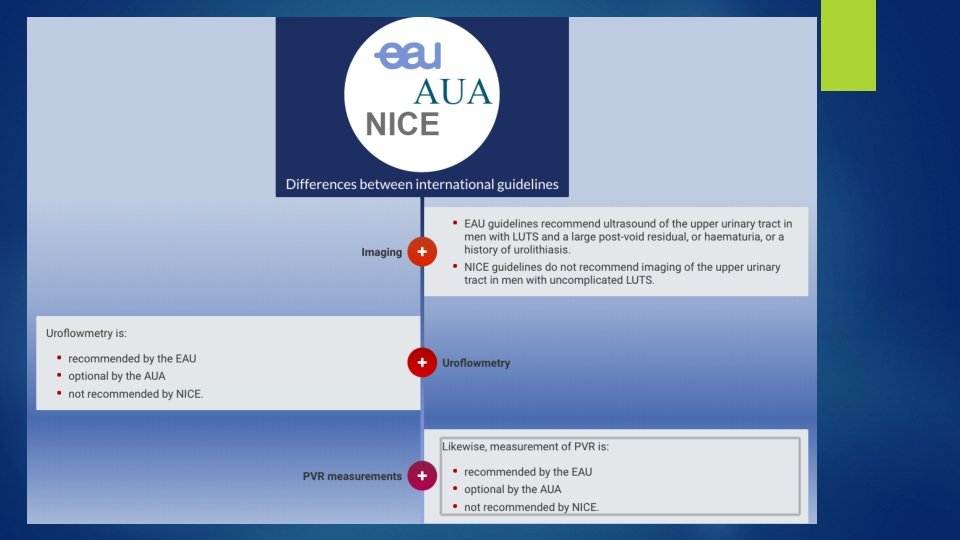
OPTIONAL � PSA �U & Es � Flow rate and PVR � Upper tract imaging � Cystoscopy � UDS

PSA With a specificity of 70%, and sensitivity of 70%, approximate age-specific criteria for detecting men with prostate glands exceeding 40 m. L are PSA > 1. 6 ng/m. L, > 2. 0 ng/m. L, and > 2. 3 ng/m. L, for men with BPH in their 50 s, 60 s, and 70 s, respectively � Roehrborn, C. G. , et al. Serum prostate-specific antigen as a predictor of prostate volume in men with benign prostatic hyperplasia. Urology, 1999. 53: 581.

Flow rate

PVR � Monitoring of changes in PVR over time may allow for identification of patients at risk of AUR.

U & Es
 �PVR �Prostate size and shape")
Imaging �Upper tract (Hydronephrosis) �PVR �Prostate size and shape

Cystoscopy

UDS

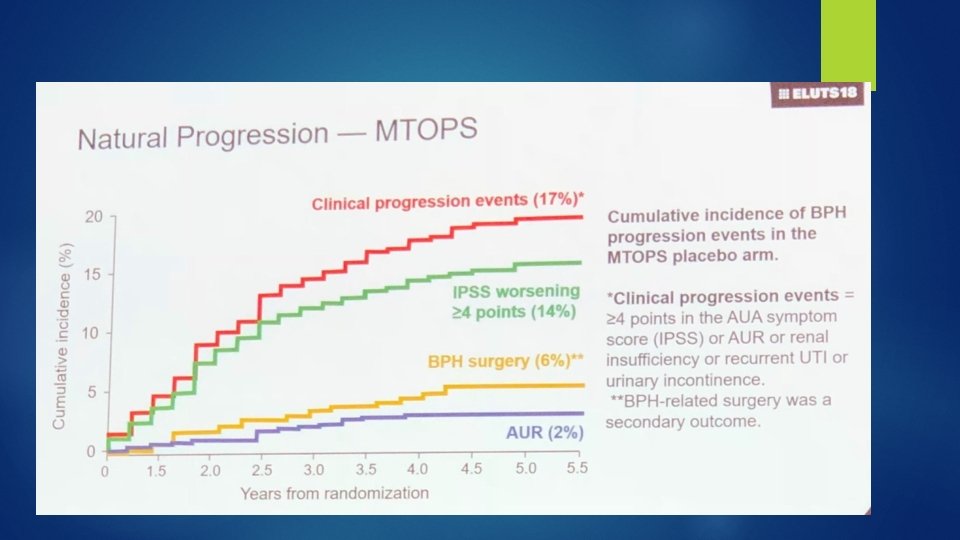
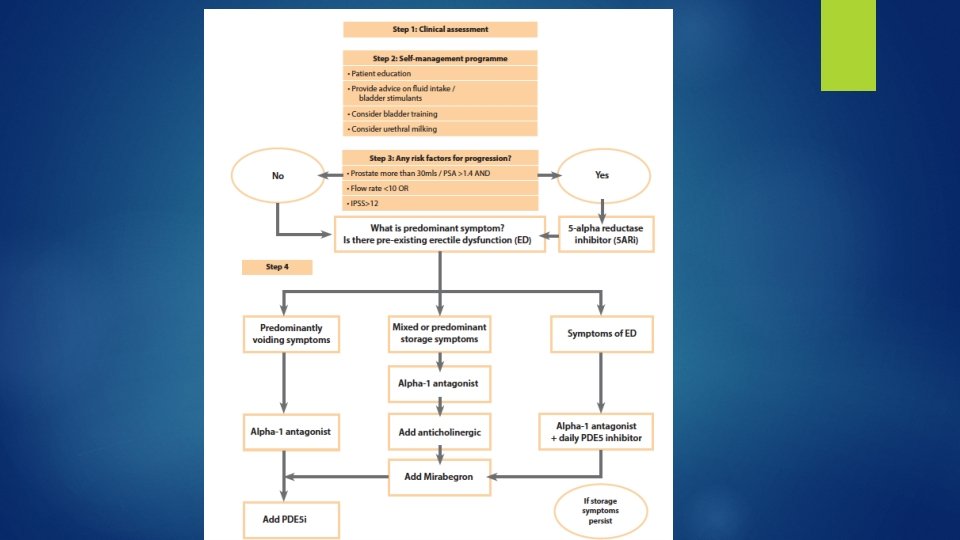
Progression �� � 1. The risk factors for progression prostate size of greater than 30 g. 2. PSA of greater than 1. 4. 3. Either an IPSS of more than 12 or a Qmax of less than 10 mls/sec. � Clinical progression of BPH 1. (IPSS) increase ≥ 4 points. 2. acute urinary retention (AUR). 3. 4. 5. urinary incontinence. renal insufficiency recurrent UTIs

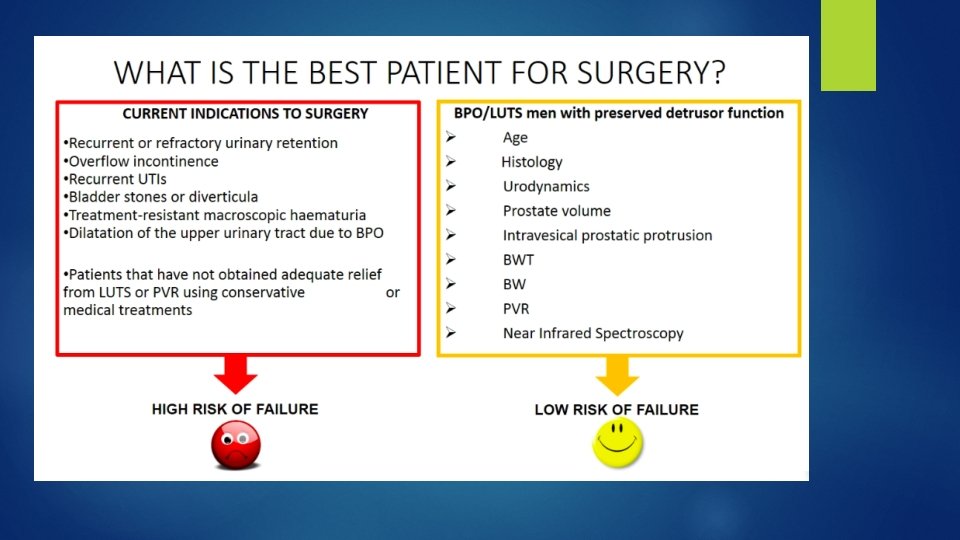
Non-invasive tests in diagnosing bladder outlet obstruction � Detrusor/bladder wall thickness � Bladder weight � IPP : Intra Prostatic Protrusion � Doppler US � prostate volume/height � near-infrared spectroscopy � penile cuff test

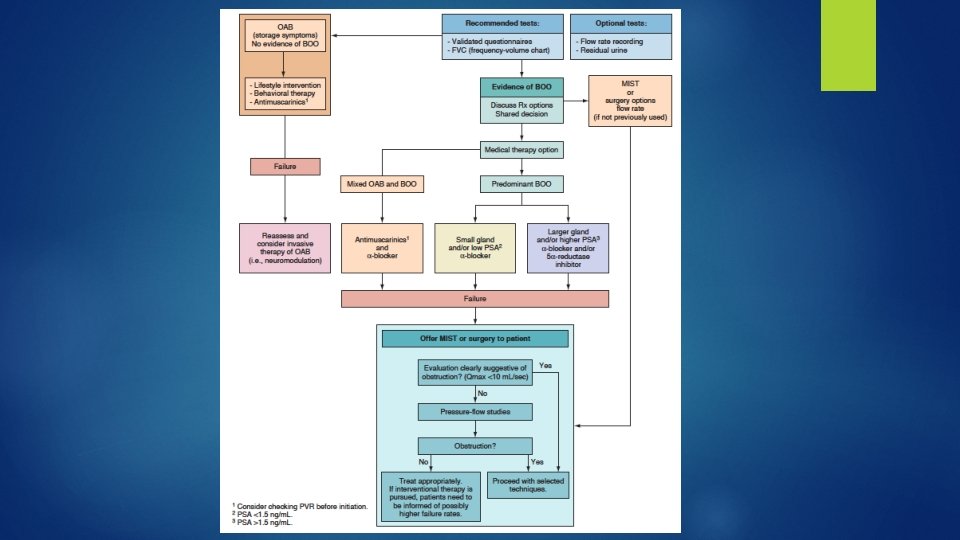
EAU
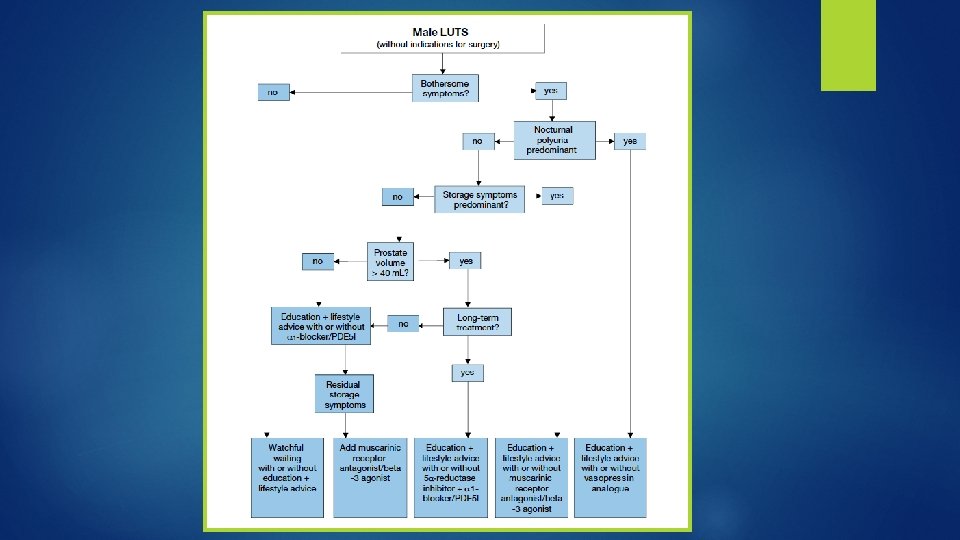

Treatment � WW / Behavioral and dietary modifications � Medical therapy � Phytotherapy � Minimally � Surgery invasive surgery

WW � Education � Reassurance � Life style / Diet � Medication � Periodic review monitoring
 � 5α-reductase inhibitors �")
Medical therapy � α 1 -Adrenoceptor antagonists (α 1 -blockers) � 5α-reductase inhibitors � Muscarinic receptor antagonists / B 3 agonists � Phosphodiesterase 5 inhibitors � Desmopressin / Diuretics � Combination thearpy

α 1 -blockers

5α-reductase inhibitors

Anti Muscarinic / B 3 Agonists � The short-term data suggest that combination of antimuscarinic and αblocker therapy is safe with minimal risk of retentioni n carefully selected men. � It would seem advisable to avoid treating men with a substantial residual urine (200 m. L or more in most studies)

PDE 5 Is � ED and BPH share common risk factors � Suggested pathogenetic factors include impaired NO and c. GMP signaling, autonomic adrenergic overactivity and prostate / pelvic ischemia from atherosclerosis.

Surgical treatment of LUTS � The incorporation of medical management and new technologies has changed which treatment options are selected for the treatment of LUTS and BPH.

� postoperative complications and patients discharged with a catheter were more common in 2008 than 1988
: intraurethral catheter with a")
Minimally Invasive Therapy � 1 - Transurethral microwave thermotherapy (TUMT): intraurethral catheter with a cooling system. prostatic heating and coagulative necrosis. � 2 - High intensity focused ultrasound (HIFU) transrectal probe is used. GA or heavy intravenous sedation is required. � 3 -Transurethral radiofrequency needle ablation (TUNA) transurethral needle delivery system � 4 - Water-induced thermotherapy(WIT) : is anothermalbased therapy for BPO that aims to produce heat-induced coagulative necrosis using heated water. 45 -minute OP procedure with topical lidocaine jelly.

5 - Prostatic stents � Permanent stents are biocompatible, allowing for epithelialisation. Temporary stents do not epithelialise and may be either biostable or biodegradable � are associated with significant complications such as migration , encrustation, infection and chronic pain.

The TIND is a nickel-titanium alloy, or nitinol, device which is placed transurethrally into the prostatic urethra to exert outward pressure on the obstructive prostatic lobes for 5 days prior to removal.

PAE � Complications: 1. Irritative symptoms. 2. Hematuria 3. Postembolization syndrome 36% 4. Major complications < 1% : Bladder Ischemia , Persistent Perineal pain.

Intra-prostatic injections � Various substances have been injected directly into the prostate in order to improve LUTS, these include Botulinum toxin-A (Bo. NT-A), NX-1207 and PRX 302. � The primary mechanism of action of Bo. NT-A is through the inhibition of neurotransmitter release from cholinergic neurons. Bo. NT-A also appears to act by modulating the neurotransmissions of sympathetic, parasympathetic and sensory nerve terminals in the prostate, leading to a reduction in growth and apoptosis of the prostate. � A recent meta-analysis showed no differences in efficacy compared with placebo and concluded that there is no evidence of clinical benefits in medical practice.
 � PUL involves the transurethral placement of small permanent intraprostatic")
Urolift (prostatic urethral lift) � PUL involves the transurethral placement of small permanent intraprostatic implants , Under LA , day-case setting. � Advantages: ability to treat LUTS due to BPH whilst preserving both erectile and ejaculatory functions. � At 3 years, the mean total IPSS was significantly improved by 41. 1%, quality of life (Qo. L) by 48. 8%, and Qmax by 53. 1%. � 10. 7% patients originally randomized to PUL required surgical reintervention for treatment failure within the first 3 years. � Not inferior to TURP and HOLEP in improving IPSS, Qo. L or Qmax. Superior to TURP in regards to Complications. � A limitation of Uro. Lift procedure is that it had been recommended for the treatment of obstructing lateral prostate lobes, but not for obstructing prostatic median lobe.
 � The Rezum system utilizes (WAVE) to ablate prostatic")
convective water vapor energy (WAVE) � The Rezum system utilizes (WAVE) to ablate prostatic tissue � Office or hospital setting using oral pain medication. Applicable to all prostate zones including the median lobe and prostate volumes greater than 30 cm 3. � The procedure lasts up to 20 minutes. � It is consists of a portable generator and a single-use disposable delivery device which is introduced into the body through the urethra and is guided to the prostate using a telescopic lens. � RF energy is produced by the generator and this heats up water outside of the body to generate vapour or steam. The steam is then delivered to the prostate. � WAVE was shown to provide rapid and durable improvements in LUTS whilst preserving erectile and ejaculatory function.

Aquablation � Aquablation is a water ablation therapy combining image guidance and robotics for the removal of prostatic tissue. � high-velocity saline stream selectively ablate prostatic glandular tissue while sparing collagenous structures such as blood vessels and capsule. � The extent and depth of ablation was predetermined by endoscopic and TRUS guidance. � All aquablation treatments were performed under general / Spinal anaesthesia. � Mean procedural time was 48 min with an aquablation treatment time of 8 min. � The ablated tissue is aspirated through ports in the handpiece and can be used for histology. Haemostasis can be achieved by cautery or by inflating a Foley balloon catheter inside the prostatic cavity. Catheter time 2 -4 days.

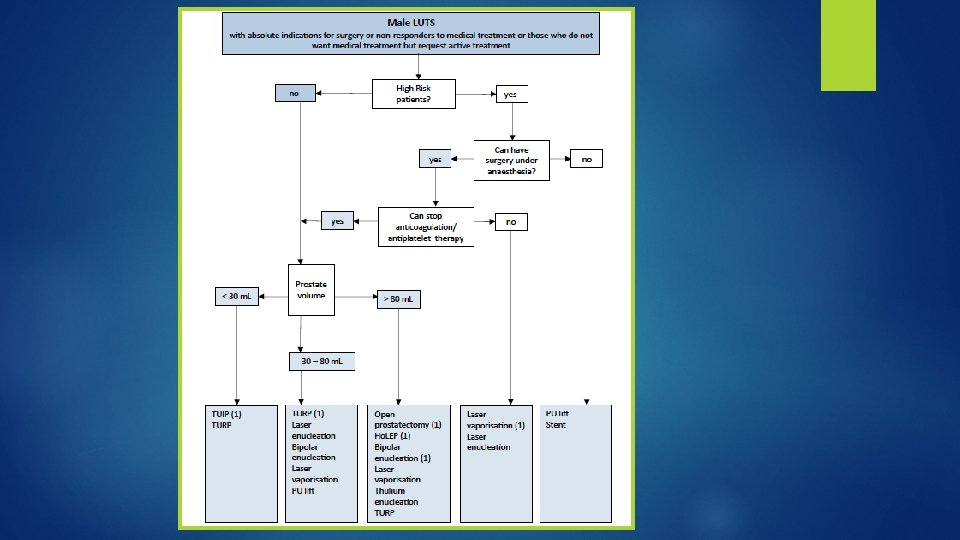
TUIP � TUIP shows similar efficacy and safety to TURP for treating moderateto-severe LUTS secondary to BPO in men with prostates < 30 m. L. without large median lobe. � No case of TUR-syndrome has been recorded, the risk of bleeding requiring transfusion is negligible and retrograde ejaculation rate is significantly lower after TUIP, but the reoperation rate is higher compared to TURP.

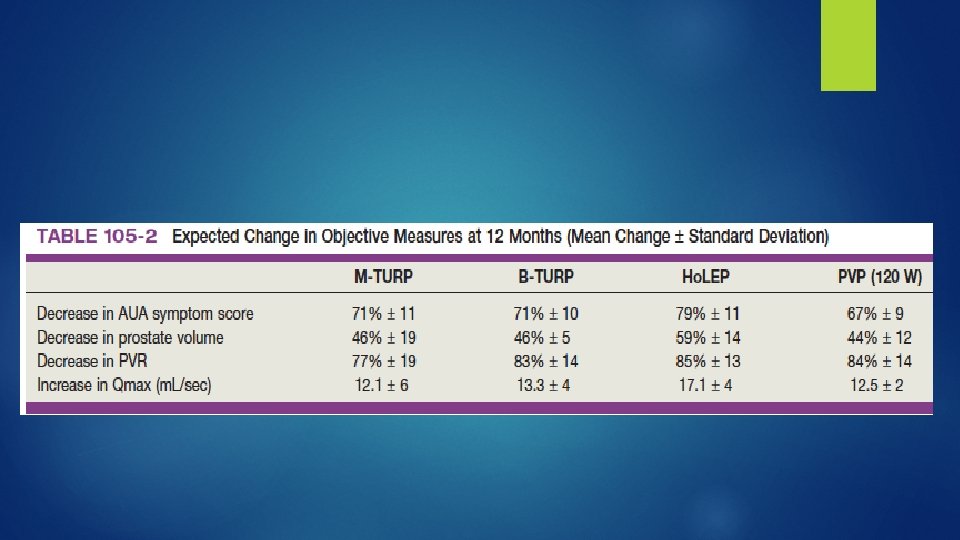
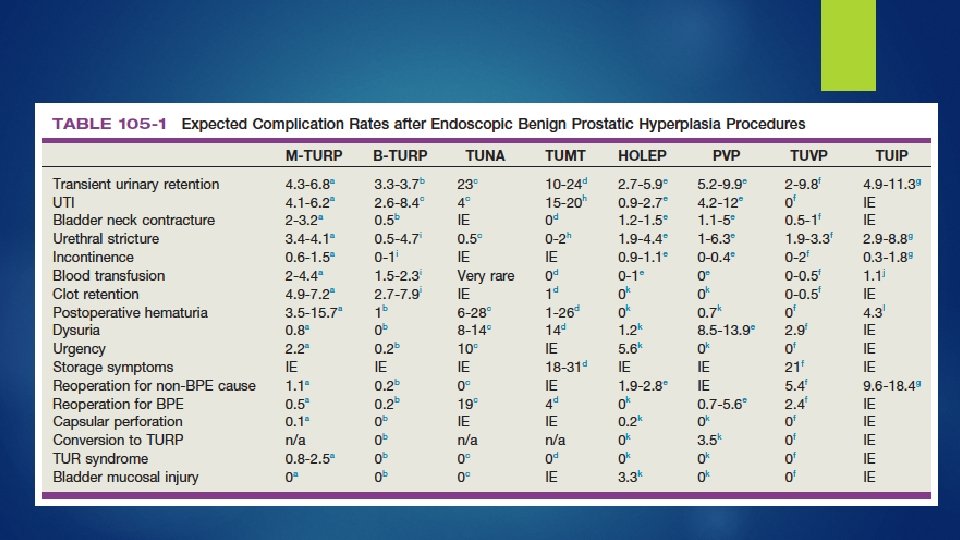
TURP � � � TURP is the current standard surgical procedure for men with prostate sizes of 30 -80 m. L and bothersome moderate-to-severe LUTS secondary of BPO. 20 contemporary RCTs with a maximum follow-up of five years, TURP resulted in a substantial mean Qmax improvement (+162%), a significant reduction in IPSS (-70%), Qo. L score (-69%), and PVR (-77%) Failures were associated with DUA rather than re-development of BPO Peri-operative mortality 0. 1% , TUR syndrome 1. 1% and morbidity 11. 1%. bleeding requiring transfusion 2%. In a large-scale study of 20, 671 men, the overall re-TURP was 2. 9%, 5. 8% and 7. 4% at one, five, and eight years follow-up, respectively. Re-operation was more common after TUIP (18. 4%) than after TURP (7. 2%)
")
M-TURP / B-TURP � RCTs with mid- to long-term follow-up (up to 60 months) show no differences in efficacy parameters. � Early pooled results concluded that no differences exist in short-term urethral stricture/BNC rates, but B-TURP is preferable due to a more favourable peri-operative safety profile (elimination of TURsyndrome; lower clot retention/blood transfusion rates; shorter irrigation, catheterisation, and possibly hospitalization times)
 � minimal direct tissue contact (hovering technique).")
Bipolar transurethral vaporisation of the prostate (B-TUVP) � minimal direct tissue contact (hovering technique). � Early pooled results concluded that no significant differences exist in short-term efficacy (IPSS, Qo. L score, Qmax and PVR) between plasmakinetic B-TUVP and TURP � B-TUVP has a lower short-term major morbidity compared to TURP
 � (TUEB) has emerged as an alternative prostatic enucleation")
Transurethral enucleation with bipolar (TUEB) � (TUEB) has emerged as an alternative prostatic enucleation procedure for BPH using the standard bipolar electrosurgical unit and the bipolar resection sheath with a modified TUEB electrode. � This allows for a reduced initial cost of investment and limits costs. The need for a morcellator can be cut down if the enucleated lobes are kept attached to the bladder neck and resected into small chips and evacuated. � TUEB is easier than learning holmium laser enucleation of the prostate. It would also be easier to convert a TUEB procedure to TURP if nonprogress or complications are encountered during the initial learning curve. � In a recent meta-analysis comparing (TUEP) with transvesical open prostatectomy, the authors have found similar functional outcomes and a favorable perioperative outcome profile concerning hemoglobin level drop, catheter period, irrigation length, need for blood transfusion, and hospital stay.
 � is a pulsed solid-state laser")
Holmium laser enucleation of the prostate (Ho. LEP) � is a pulsed solid-state laser that is absorbed by water and water-containing tissues. Tissue coagulation and necrosis are limited to 3 -4 mm, which is enough to obtain adequate hemostasis. � In a meta-analysis of studies comparing Ho. LRP with TURP no difference in symptom improvement could be detected at six or twelve months post-operatively.
 vaporisation of the prostate � Laser energy is")
Greenlight laser (The Potassium-Titanyl. Phosphate KTP) vaporisation of the prostate � Laser energy is absorbed by haemoglobin, but not by water. Vaporisation leads to immediate removal of prostatic tissue, relief of BPO, and reduction of LUTS. � Laser vaporisation of the prostate using the 80 -W KTP and the 120 -W LBO laser (PVP) demonstrated higher intra-operative safety with regard to haemostatic properties when compared to TURP. Perioperative parameters such as catheterisation time and hospital stay are in favour of PVP, whereas operation time and risk of reoperation are in favour of TURP. Short-term results for the 80 -W KTP laser and mid-term results for the 120 -W LBO laser were comparable to TURP.
, vaporesection")
Thulium : YAG LASER prostatectomy � Different applications, ranging from vaporisation (Thu. VAP), vaporesection (Thu. VARP), and enucleation (Thu. LEP). � Laser enucleation of the prostate demonstrates high intra-operative safety with regard to haemostatic properties when compared to TURP. Short-term results are comparable to TURP. � Laser vapoenucleation of the prostate using a Tm: YAG laser (Thu. VEP) seems to be safe in patients receiving anticoagulant or antiplatelet therapy. � Peri-operative parameters like catheterisation time and hospital stay are in favour of thulium lasers. Long-term results are similar to TURP.
. • TURP not technically possible (e.")
Open prostatectomy Indications • Large prostate (>100 g). • TURP not technically possible (e. g. limited hip abduction). • Failed TURP (e. g. because of bleeding). • Urethra too long for the resectoscope to gain access to the prostate. • Presence of bladder stones which are too large for endoscopic cystolitholapaxy, combined with marked enlargement of the prostate. � Contraindications • Small fiibrous prostate. • Prior prostatectomy in which most of the gland has been resected or removed; this obliterates the tissue planes. • Carcinoma of the prostate.
.")
� Open prostatectomy mortality has decreased significantly during the past two decades(< 0. 25%). The estimated transfusion rate is about 7 -14% Long-term complications include transient urinary incontinence (up to 10%), BNC and urethral stricture (about 6%)
 and robot-assisted simple prostatectomy")
Minimal invasive simple prostatectomy � Includes laparoscopic simple prostatectomy (LSP) and robot-assisted simple prostatectomy (RASP). � Both LSP and RASP are performed using different personalised techniques, developed based on the transcapsular (Millin) or transvesical (Freyer) techniques of OP. An extraperitoneal approach is mostly used for LSP, while a transperitoneal approach is mostly used for RASP. � Minimal invasive simple prostatectomy seems comparable to OP in terms of efficacy and safety, providing similar improvements in Qmax and IPSS.

Summary � It's difficult to project one procedure as the standard of treatment either because of insufficient good quality evidence, surgeon's expertise or variability of patient preferences. � the choices of surgical approach (open or endoscopic and energy source-electrocautery versus laser) are technical decisions based on the patient's prostate size, the individual surgeon's judgment and the patient's comorbidities.
- Slides: 60