Lung Transplant Dave Sweet CASE n You are


 2) 3) 4) 5) 6) What diseases are currently we doing")







 2) 3) Use of time-dependent, nonproportional hazard models, equity")
")


 n And/or Pa. CO 2 >55")








 n In 1998 guideline no official recommendation. n")


 began allocating lungs")
 2) 3) Developed by multivariate modeling and approved by OPTN")





, <50 years (lung) n Smoking history less than 20 pack-years")

 How is the choice for a single vs a double lung")




 2) 3) Feel do not exclude other patient in many")


 In what situations will a lung transplant be done on bypass?")
 2) 3) 4) Most adult transplants can be done without CPB.")
 If get significant PGD it is unlikely")


 Generally what ventilator settings would you like post transplant px to")



 Generally discuss your fluid management post op. What variables are you")



Although our patient remains hemodynamically stable. Why is shock in these patients")

 and vasopressors n STAT ECHO (TEE) n Notify the Surgeon")


 What is your differential for early respiratory failure in the lung")
 2) 3) 4) 5) 6) 7) DDx: Reperfusion injury")
 2) 3) 4) Risk factors: Preop pulmonary htn Rt")
 Briefly describe Reperfusion injury, Primary Graft failure. What can we do")




 2) 3) Pathogenesis: Variety of perturbations implicated. Factors")

 2) 3) How can we help prevent ischemiareperfusion injury?")






















 Initiated after 0 -2 days")













: 70% of graft recipients are dx by 5")


")
 n Conversion from cyclosporin to tacrolimus may stabilize")
Could this be infectious? Where in the complications timeline to infectious etiologies")
















 died during their ICU admission. n 16/27 (59%) receiving MV died. n")




- Slides: 141
Lung Transplant Dave Sweet
CASE n You are currently the fellow working at VGH and as you come in Monday morning the charge nurse tells you that there are several transplants going on today including a lung transplant and that we are holding a bed. You have several resident working with you that are very excited and they start firing questions off….
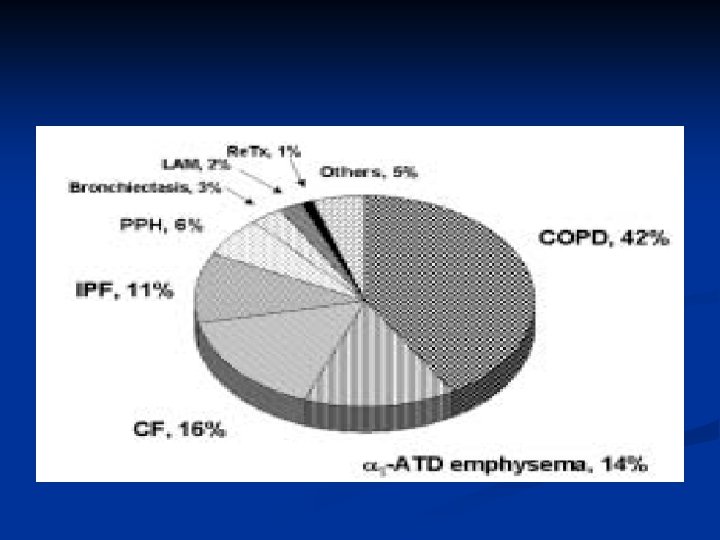
CASE n 1) 2) 3) 4) 5) 6) What diseases are currently we doing lung transplants for? Alpha 1 -antitrypsin CF COPD IPF (UIP and occ NSIP) IPAH (including Eisenmengers) Sarcoidosis
CASE n What are the general goals for determining the appropriateness of a lung transplant in a individual patient?
General Principles Need to consider the natural history and prognosis of primary disease and weigh against projected survival post transplant. n Ultimate goal= n Obtain max mileage from native lung, conferring a greater overall survival time with new lung. n Avoiding death on the waiting list. n
General Principles Consider quality of life while on waiting list compared to quality of life with new lung. n Traditionally, looked at the median 2 -year posttransplant survival rate and compared this to projected survival with underlying condition. n When former=longer…. patients are transplant candidates. n
General Principles 2 year survival rate is not arbitrary number. Two reasons why used. 1) Average waiting time is around 2 yrs. 2) Based on disease the first month mortality varies greatly. …. . but then the mortality decreases relatively linearly. This will compensate for this. n
CASE n Do the survival rates for different diseases vary post transplant? What is the generally quoted first month mortality?
CASE First month mortality quoted as 7% to 24%
CASE n Which diseases are thought to have the greatest survival advantages? Which diseases are questionable?
Survival advantage? n n 1) 2) 3) Use of time-dependent, nonproportional hazard models, equity points, and crossover points. Survival benefit demonstrated with: CF IPAH Critical Care Aspects of Lung Transplantation. Journal of Intensive Care Med 19(2); 2004
Survival advantage? However, also raised questions about any survival benefit for px with 1) COPD 2) Eisenmener syndrome But in addition to survival, quality of life also needs to be taken into consideration. ie) COPD px changes in quality-adjusted lifeyears may be sufficient to justify transplantation. n
Survival advantage?
CASE n What are the indications for lung transplantation for these various diseases based on the ATS 1998 consensus statement?
Indications COPD n FEV 1< 25% (without reversibility) n And/or Pa. CO 2 >55 and/or elevated PAP with progressive deterioration n Preference to those px with: - elevated Pa. CO 2 with progressive deterioration - require long term oxygen therapy. n Nathan et al. Lung Transplantation: Disease-Specific Considerations for referral. Chest 2005; 127: 1006 -1016
Indications Interesting……the level of subjective dyspnea my be a better predictor of mortality than FEV 1. n ie) grade IV dyspnea= stopping to take a breath during 100 yrd walk. - median survival of 3 yrs, which is comparable to 3 yr posttransplant survival rate (61%) n In contrast, FEV 1<35% pred had a median survival of 5 yrs. n
Indications Currently several other models being investigated which incorporate a number of diff parameters such as the BODE index. n Body weight, Obstruction, Dyspnea level, Exercise tolerance. n Score out of 10. n 7 -10=80% mort at 52 months (transplant cand) n <7= 5 yr mort of <50% (not transplant cand) n
Indications IPF: n Divided now into UIP and NSIP n UIP=When diagnosed should be referred!!! n Traditionally, break points at FVC of 60 -70% and DLCO of 50 -60% are indicative for poor outcome. Very inconsistent. n
Indications Other models look at DLCO and HRCT scan to help predict mortality (May see in future!) n Also, one of the most sensitive markers may be desaturation to less than 89% during a 6 min walk. n If able to maintain sats may be able to defer transplant referral. n
Indications NSIP: n True NSIP have much better prognosis and majority will not need transplant. n Subgroup which may require include: 1) DLCO <35% and/or a dec in DLCO of >15% have shown to have mortality similar to UIP with median survival of 2 yrs. n
Indications CF: n FEV 1 <30% or n Rapid progressive resp deterioration with FEV 1 >30% (inc hosp, rapid fall in FEV 1, massive hemoptysis, inc cachexia) n Room air Pa. CO 2 >50 or Pa. O 2 <55. n Woman whose condition is deteriorating rapidly. n
Indications IPAH: n Medical management has improved greatly. n 1990= 10. 5% of all lung transplants. n 2001=3. 6% of all lung transplants. n Should exhaust all medical management before consider transplant. n
Indications NYHA class III or IV after 3 months of IV epoprostenol have 2 yr survival of 46% and should be considered for transplant. n NYHA class I and II= 93% and not candidate. n
Indications Sarcoidosis (common disease, rare transplant) n In 1998 guideline no official recommendation. n Need to have stage IV. Advanced fibrotic changes, honey-combing, hilar retraction, bullae, cysts, and emphysema. n Also reasonable when FVC<50% and/or FEV 1 <40%. n
CASE n n After you clearly describe the answers to the above questions your staff speaks up and asks you if you are familiar with the Lung Allocation Score (LAS). What is the LAS? Why was it designed?
LAS In Canada we determine how organs or allocated by: n Size of patient n ABO matching (Not HLA matching) n Time on the list. n Kozower et al. The impact of the lung allocation score on short-term transplant outcomes: A multicenter study. J thorac Cardiovasc Surg 2008; 135: 166 -77
LAS In the US: n Organ procurement and transplantation network (OPTN) began allocating lungs in 1990 based on size, blood type and amount of time candidate had spent on waiting list. n 1995, minor change when 3 months credit given to IPF px to offset their inc mortality. (Not done in Canada) n To better list px according to medical urgency and expected benefit the LAS was developed.
LAS n n 1) 2) 3) Developed by multivariate modeling and approved by OPTN in 2004. Implemented in May 2005. Three main objectives are: Reduce deaths on transplant list Inc transplant benefit for lung recipients Ensure efficient and equitable allocation of organs
LAS Gives a score between 1 -100. n Weighted combination of predicted risk of death during the following year on the waiting list and the predicted likelyhood of survival during the first year after transplant. n
CASE n Is there any evidence that it is working?
n n n n First year of implementation compared to previous year. 170 in each group. Dec in waiting times (680 to 445 days). Dec death on waiting list (74 to 51… 30%) Determined that there was a switch with inc in IPF px and dec in COPD and CF. Inc in primary graft dysfunction (14. 1 to 22. 9%). Inc in ICU stay (5. 7 to 7. 8 days). Hosp mort and 1 yr survival were similar.
n n n Concluded that the LAS is doing what it was designed to do. Reason why inc in PGD is likely due to higher number of retransplants and IPF which both are established risk factors for PGD. When controlled for Dx, the rates of PGD were no longer different. This also explains the inc in ICU stay, mech vent. Most important…. . no change in mortality.
Donor criteria? Less than 20% of organ donors possess lungs suitable for transplantation
Age <40 years (heart-lung), <50 years (lung) n Smoking history less than 20 pack-years n Arterial partial oxygen pressure of 140 mm Hg on a fraction of inspired oxygen (FIO 2) of 40% or 300 mm Hg on an FIO 2 of 100% n Normal chest x-ray Sputum free of bacteria, fungi, or significant numbers of white blood cells on Gram and fungal staining n Bronchoscopy showing absence of purulent secretions or signs of aspiration n Absence of thoracic trauma n Human immunodeficiency virus negative n
CASE n You learn that the patient is a 58 yo male with severe COPD. Other PMHx includes a NSTEMI 8 yrs prev, HTN, hypercholesterolemia. Pre-op ECHO results show good biventricular fxn with PAS=33 mm. Hg via TRJ. Pre-op cath results show clean coronaries and right heart cath confirms the right sided pressures. Preop PFT show a PEV 1 of 25% and moderate to severe airtrapping. They are doing a single right lung transplant and no plan for bypass.
CASE n 8) How is the choice for a single vs a double lung transplant made? In what situations is a double lung preferred?
Single vs Double? Based on numerous factors such as: n Disease n Age n Comorbidities n Institutional biases n Organ availability n Emergency of procedure n
Single vs Double? Majority done in Canada are single lung transplants. n First isolated single lungs were done for pulmonary fibrosis and this continues to be the norm. n COPD originally thought not possible to receive single lung transplants. n First done in 1989 by Mal and colleagues n Critical Care Aspects of Lung Transplantation. Journal of Intensive Care Med 19(2); 2004
Single vs Double? n n Currently a standard throughout the country. Specifically, in COPD if px is of shorter stature and older do better. Pulmonary HTN= single or double but if choose single expect to have more difficulty in first few days. Many centers mandate only bilateral. Bilateral transplants are mandatory for px with CF and bronchiectasis. Critical Care Aspects of Lung Transplantation. Journal of Intensive Care Med 19(2); 2004
Single vs Double? n n Bilateral lung transplants for mycetomas or other chronic fungal or mycobacterial infections Many larger centers are now favoring bilateral transplants. Specifically the Duke University Medical Center. Critical Care Aspects of Lung Transplantation. Journal of Intensive Care Med 19(2); 2004
Single vs Double? 1) 2) 3) Feel do not exclude other patient in many cases. If single lung is “marginal” for transplant, taking both will provide adequate function. Early post-op management is easier with bilateral
Single vs Double? Additionally, in 225 px who survive 6 months. n Single lung transplant (as compared to bilateral) was a significant risk for BOS in multivariate Cox model (HR=2. 08, p=0. 001) n ? If immunologic advantages of bilateral ? n Hadjiliadis D et. al. Chest 2002; 122: 1168 -1175.
Single vs Double? n n n A recent review of the United Network of Organ Sharing lung transplant database of 2260 transplants for emphysema compared single vs double lung transplants. No difference in 30 day mortality but long term survival data favored bilateral lung transplants for individuals <60 yrs of age. Bilat were older and more women. ? How to interpret? Meyer et al. J heart Lung Transplant 2001; 20: 935 -941.
Case n 9) In what situations will a lung transplant be done on bypass? Why if done on bypass is it relevant to post-op management?
Bypass? n 1) 2) 3) 4) Most adult transplants can be done without CPB. A number of specific situations will necessitate CPB. Primary or secondary pulmonary htn are most safely done on bypass. Px with CF likely have such voluminous purulent secretions that independent ventilation is impossible. During bilateral transplant early graft dysfxn of the first transplanted lung (reperfusion) preventing single lung vent. If native lung is unable to sustain patient with single lung ventilation.
Bypass? Why relevant to post-op care? 1) If get significant PGD it is unlikely the patient can be supported on single lung ventilation. 2) Bypass is a significant risk factor for PGD!! n Most recent large study by Dalibon, which reviewed 140 LT, confirmed that CPB was associated with longer MV, more pulm edema, more transfusions and inc early mortality!! Dalibon et. al. J Cardiothorac Vasc Anesth 2006; 20: 668 -672.
CASE n You hear that the case is finishing up. There was minimal surgical difficulty the lung was implanted using continuous 3/0 polypropylene sutures for the bronchial anastomosis (end-endtechnique), continuous 4/0 polypropylene sutures for the pulmonary vein to left atrial anastomosis, and continuous 5/0 polypropylene sutures for the pulmonary arterial anastomosis.
CASE n Unfortunately you hear that they need to do the case on bypass as they were unable to do the transplant on single lung ventilation. The overall ischemia time was 6 hours and 8 minutes for the lung. The post-transplant bronch looked pristine and the TEE looked good. The patient is brought to ICU post-op stable on AC and FIO 2 of 100% and quickly weaned to 80%. CVP=12 CI=3. 5, PA=40/18. (If the nurse said the PAWP=16…what would you say? ? )
CASE n 10) Generally what ventilator settings would you like post transplant px to be on? What about this patient? What is your general plan to wean the ventilator?
Ventilation? Many centers prefer a PC ventilation so as to limit peak airway pressures (<40) and prevent barotrauma to the brochial anastomosis. n Plat pressure should additionally be limited to less than 30 to 35 mm. Hg. n Minimize Fio 2 as quickly as possible. n Critical Care Aspects of Lung Transplantation. Journal of Intensive Care Med 19(2); 2004
Ventilation? n n This patient? Due to the very compliant native lung with potential for air trapping and the relatively stiff transplant lung…. need to be aware of balance. To begin, as long as oxygenation is not a issue. Ventilation as if to prevent air trapping in native lung. Min PEEP, adequate expiratory phase with PC. Can still use EEP to determine if airtrapping. Critical Care Aspects of Lung Transplantation. Journal of Intensive Care Med 19(2); 2004
Ventilation? n n Generally want to get off the ventilator as soon as possible. Use adequate analgesia via epidural or paravertebral (recent metaanalysis and found paravertebral block had lower rate of resp complications and side effects) …. wake and wean. If have standard PS weaning protocol it should be used as usual. Plan to have extubated in 24 to 48 hrs ideally! Davies et. al. Br J Anaesth 2006; 96: 418 -426.
CASE n 11) Generally discuss your fluid management post op. What variables are you balancing with your fluid management?
Fluid Management n n Careful fluid management is necessary to avoid substantial transplant lung edema. Usually aim for a negative fluid balance from the get go. Def aim for negative balance in the first 48 hrs. Minimal fluid and if require volume use colloid or blood. Some centers will target a CVP of <7 mm. H 20, with systemic perfusion supported by pressors. Pilcher et. al. A high CVP is associated with prolonged mech vent and inc mortality following lung transplantation. J Thoracic Cardiovasc Surg 2005; 129: 912 -918.
Fluid Management Retrospective study of 118 px. n After controlling for CV diz and vasopressors, CVP was correlated with duration of MV, with a CVP >7 also being associated with higher ICU and hosp mortality. n Unclear whether a strategy aimed at keeping CVP less than 7 would alter outcome or if a marker of severity of illness. n Pilcher et. al. A high CVP is associated with prolonged mech vent and inc mortality following lung transplantation. J Thoracic Cardiovasc Surg 2005; 129: 912 -918.
Fluid Management Obviously need to balance against the risk of renal insufficiency. n Many of these patient my have CRF…. specifically the CF px. (why? ). n Additionally cyclosporine or tacrolimus may impair renal fxn. Watch levels closely post-op. n Titrate volume to u/o. Previous many centers still using “renal dose dopamine” in this setting. No evidence. n
CASE n 12)Although our patient remains hemodynamically stable. Why is shock in these patients need to be quickly identified and diagnosed?
CASE These patients should not be shocky!! n “NEED TO MAKE DIAGNOSIS” (Dr George Isac) n Bleeding? Anastamosis? (watch CTs and hgb) n Obstructive? Anastamosis? n Cardiogenic? n Infection/sepsis? n
CASE Judicious resuscitation (colloid) and vasopressors n STAT ECHO (TEE) n Notify the Surgeon n ? Mobilize ECMO early? n Is their a benign reason why they may be requiring increasing vasopressor support? n
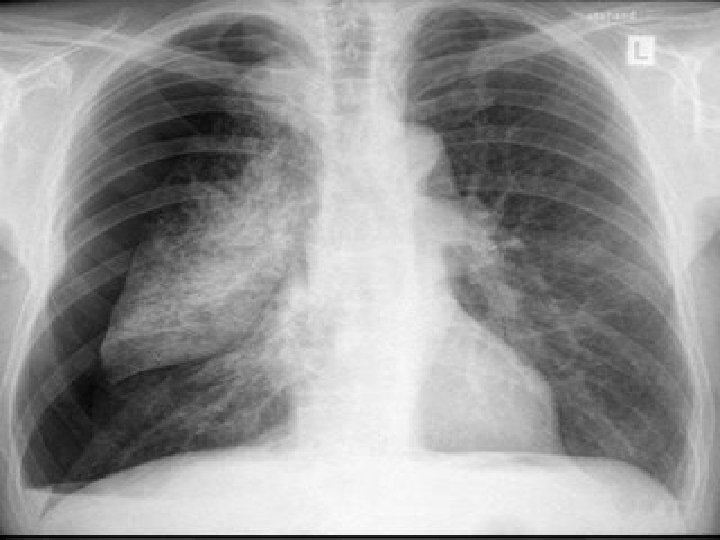
CASE n After initially settling the patient in and continuing on your rounds the RT approaches you and states that the FIO 2 requirements are back up to 100% after a brief period at 50% and hypoxia is becoming an issue. A stat CXR was done.
CASE
CASE n 13) What is your differential for early respiratory failure in the lung transplant? What are the risk factors for early respiratory failure?
Early Respiratory Failure n 1) 2) 3) 4) 5) 6) 7) DDx: Reperfusion injury (55%) Periop cardiovascular(MI, arrhythmia, CHF) /haemorrhagic (36%) Anatomic complications Infectious (bacterial and CMV) Rejection (hyperacute=rare and acute=common) Pneumothorax PE Chatila el. al. Resp failure after lung transplant. Chest 2003; 123: 165 -173.
Early Respiratory Failure n 1) 2) 3) 4) Risk factors: Preop pulmonary htn Rt vent dysfunction Prolonged ischemic time CPB Chatila el. al. Resp failure after lung transplant. Chest 2003; 123: 165 -173.
CASE n 14) Briefly describe Reperfusion injury, Primary Graft failure. What can we do to help prevent Reperfusion injury before and after the transplant? How do you manage it? (specifically in our patient? )
Ischemia-Reperfusion Injury Typically manifests in the first 72 h after transplant. n Development of airspace disease, progressive hypoxemia, and inc in pulmonary pressures (reflective both epithelial and endothelia injury) n When Pa. O 2/Fi. O 2 ratio below 200, termed primary graft failure. n Granton, J. Update of early resp failure in the transplant recipient. Current Opinion in Critical Care 2006; 12: 1924.
Ischemia-Reperfusion Injury Recent 2004 publication identified several risk factors: n CPB n BMI >25 kg/m 2 n Immediate elevated PAS n Trend in oxygenation index over 24 hrs n Elevated APACHE II n Sekine et al. J Heart Lung Transplant 2004; 23: 96 -104
Ischemia-Reperfusion Injury n n Additionally, a review of 7 French transplant centers and 752 px over 12 yrs. Found graft ischemic time associated with the Pa. O 2/Fi. O 2 ration measured at 6 hrs. 30 day mortality was associated with a lower Pa. O 2/Fi. O 2 ratio at 6 hrs. Identified cold ischemic time of 330 min (5. 5 hr) as distinguishing between px who had a uncomplicated course vs those who did not. (Max accepted is 6 -8 hrs) Thabu et al. Am J Respir Crit Care Med 2005; 171: 786 -791. Oto et al. J Thorac Cardiovasc Surg 2005; 130: 180 -186.
Ischemia-Reperfusion Injury n n n Ischemia-Reperfusion Injury also associated with long-term consequences. Retrospective cohort study of 255 LT px. Christie et al reported a 30 day mort of 63. 3% compared to 8. 8% in px with and without reperfusion injury. Median hosp was longer (47 vs 15 days) Mech vent longer (15 vs 1 day) Lower exercise capacity as assessed by 6 min walk distance at 12 months. Christie et al. Chest 2005; 127: 161 -165.
Ischemia-Reperfusion Injury n n n 1) 2) 3) Pathogenesis: Variety of perturbations implicated. Factors relating to: Donor Method of graft preservation Effects of reperfusion following period of ischemia
Ischemia-Reperfusion Injury n The Lungs may be made susceptible from cytokinemediated damage in px with elevated ICP and compounded following cold preservation of the grafts. De Perrot et al. Am J Respir Crit Care Med 2003; 167: 490 -511
Ischemia-Reperfusion Injury n n 1) 2) 3) How can we help prevent ischemiareperfusion injury? Can divide into: Pre-transplant interventions Peri-surgical interventions Post-surgical interventions
Ischemia-Reperfusion Injury
Ischemia-Reperfusion Injury Pre-Surgical interventions: n Preservation solution…specifically a lowpotassium dextran solution provides superior preservation over high potassium preservation solutions. n In addition, nitric oxide added to the flush during harvest provides a preservation advantage. (not well studied) n Maccherini et al. Transplantation. 1991; 52: 621 -626 Yamashita et al. Ann thorac Surg. 1996; 62: 791 -797
Ischemia-Reperfusion Injury n It is known that lung hyperinflation is a excellent model of pulmonary edema…. therefore care should be taken to avoid during harvest and storage.
Ischemia-Reperfusion Injury Peri-Surgical interventions: n Lick and colleagues reported a small series where using leukocyte-filtered modified perfusate is pumped through the lung at time of reperfusion. In case report…. no ischemiareperfusion injury. n Lick et al. Ann Thorac Surg. 2000; 69: 910 -919
Ischemia-Reperfusion Injury Post-surgical interventions: n TP-10 inhibitor - One of few randomized trials in lung transplantation, using soluble complement receptor-1 inhibitor led to reduction in duration of mech vent. - Interestingly, greatest effect in px who received bypass. n
Ischemia-Reperfusion Injury n - - NO Early preclinical and uncontrolled reports suggested that admin of NO either prior to or shortly after reperfusion injury could dec severity of disease. Recent controlled clinical trial failed to show benefit when inhaled 10 min after reperfusion. Meade et al. Am J Respir Crit Care Med 2003; 167: 1483 -1489.
Ischemia-Reperfusion Injury n - - NO Another recent trial by Perrin. RCT in 30 bilateral lung transplants. 20 ppm i. NO at time of reperfusion vs control. Could not identify any reduction in extravasular lung water (p=0. 61) or improvement in gas exchange (p=0. 61). Future studies needed. Perrin et al. Chest 2006; 129: 1024 -1030
Ischemia-Reperfusion Injury ICU management: n Adoption of lung protective strategy would seem reasonable. (only one rat study has actually looked at this). n “In refractory hypoxemia use of inhaled NO, HFO and ECMO may improve gas exchange. ” n Granton, J. Update of early resp failure in the transplant recipient. Current Opinion in Critical Care 2006; 12: 1924.
Ischemia-Reperfusion Injury n n n What about our patient? ? In COPD single lung Tx that develop reperfusion injury…. dilemmas may arise. As px becomes hypoxic and more aggressive vent/peep strategies are used…. may overdistend native lung. Cause shunting of blood to dysfunctional allograft. Futhermore, if worsens still, mediastinal shift may result in impaired venous return.
Ischemia-Reperfusion Injury n n Better to minimize tidal volumes and lowest PEEP to gain acceptable oxygenation and accepting mild respiratory acidosis (+/- novalung? ? ) Place px in lateral decubitus with transplant side up, and aggressive chest physiotherapy. If this fails…. should consider independent lung ventilation. Be aware that will be more difficult to clear secretions and the ease with which the tube may be dislodged. Gavazzeni et al. Chest. 1993; 103: 297 -299.
Prediction of Independent Lung Vent. Prediction of need for single lung ventilation? n Study looking at 170 px who had single lung transplant for COPD. n 12% required independent lung ventilation. n Similar in age, sex, ischemic time, and donor characteristics to those who required conventional ventilation. n Pilcher et al. Predictors of independent lung ventilation: an analysis of 170 single-lung transplantations. Pilcher J Thorac Cardiovasc Surg. 2007 Apr; 133(4): 1071 -7
Prediction of Independent Lung Vent. Patients receiving independent lung ventilation had a greater degree of: n Preoperative airflow limitation (FVC 1/FVC) n More hyperinflation n Lower postoperative Pa. O 2/fraction of inspired oxygen ratios n More radiologic mediastinal shift n More transplant lung infiltrate on the postoperative chest radiograph. n
Prediction of Independent Lung Vent. Multivariate logistic regression analysis showed that independent lung ventilation was associated with: n Increasing levels of recipient hyperinflation (percentage total lung capacity compared with predicted value; odds ratio 1. 04; P =. 032) n Reduced early postoperative Pa. O 2/fraction of inspired oxygen ratio (odds ratio 0. 96; P =. 005) n
Prediction of Independent Lung Vent. Length of ventilation and intensive care unit stay and mortality were higher in the independent lung ventilation group. n Among patients who survived to hospital discharge, there were no differences in longterm mortality between the 2 groups. n
Prediction of Independent Lung Vent. Conclusions= Independent lung ventilation predicted by the combination of: n Increased hyperinflation measured on recipients' preoperative lung function tests n Low Pa. O 2/fraction of inspired oxygen ratio, indicating graft dysfunction in the immediate postoperative period. n
Prediction of Independent Lung Vent. n n n - Another study looking at predictors of native lung hyperinflation. Retrospectively analyzed data from 27 patients who underwent 31 single lung transplantations for emphysema. Two groups: 12 patients with development of acute or chronic NLH 15 patients without development of hyperinflation Yonan. Single lung transplantation for emphysema: predictors for native lung hyperinflation. J Heart Lung Transplant. 1998 Feb; 17(2): 192 -201
Prediction of Independent Lung Vent. NLH was defined as: n Radiologic mediastinal shift with n Flattening of the ipsilateral diaphragm n Associated with respiratory dysfunction or hemodynamic instability n
Prediction of Independent Lung Vent. n n n n n No differences between the two groups regarding: age preoperative partial pressure of oxygen partial pressure of carbon dioxide acid-base status donor lung size and physiological structure side of transplantation primary pathologic condition rejection score infection episodes and obliterative bronchiolitis in the transplanted lung after operation.
Prediction of Independent Lung Vent. Patients with NLH had: n Significantly higher preoperative mean pulmonary artery pressure > 30 mm Hg. n Lower mean FEV 1. n Higher mean residual volume. n
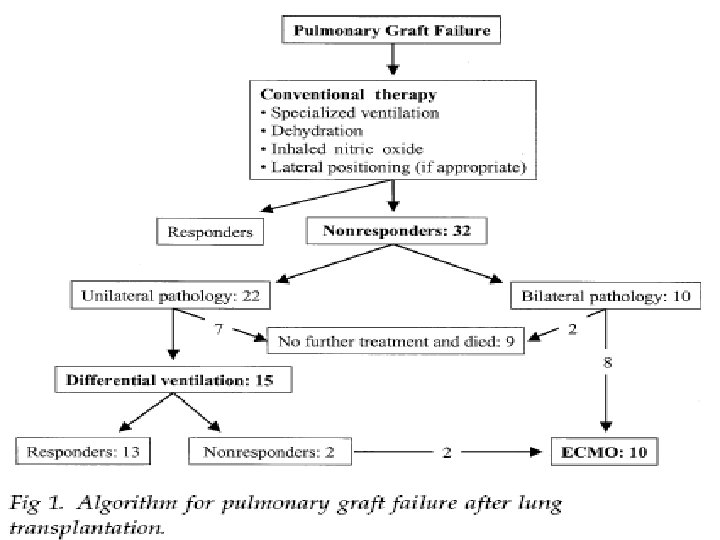
CASE A quick in and out bronch shows no anatomic abn and on TEE the pulmonary veins look good. After a short period of time you realize that he is deteriorating that the hypoxia is quickly becoming refractory. You quickly mobilize ECMO and after a short time on ECMO the patient stabilizes. 15) Your staff asks you if you know of any evidence for the use of early ECMO in these patients? n
ECMO n n Several publications looking at ECMO in this situation. In the setting of pulmonary htn (high risk), early ECMO has been advocated (experience based). Another review of 17 cases ECMO may preserve initial organ function due to reduction in use of injurious ventilation strategies. Dahlberg et al. J Heart Lung Transplant 2004; 23: 979 -984. Pereszlenyi et al. Eur J Cardiothorac Surg 2002; 21: 858 -863.
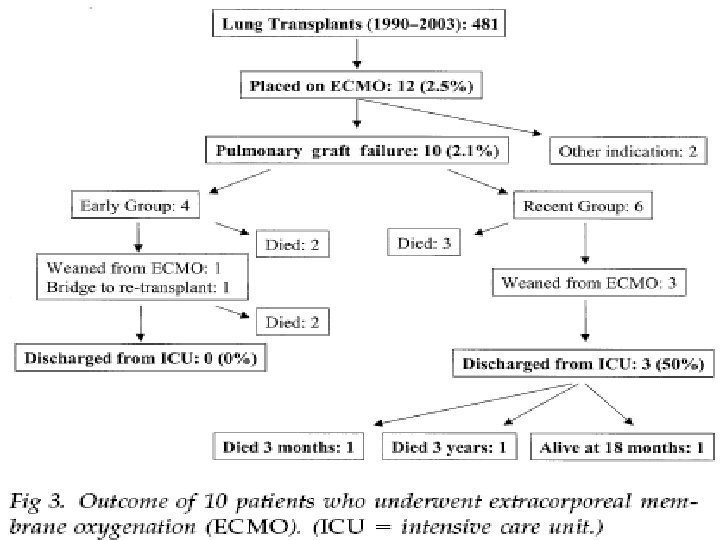
ECMO More recent publication by Oto at Alfred Hosp in Melbourne. n Ten transplant recipients from total of 481 (2. 1%) were treated with ECMO. n Prior to initiation had TEE to exclude lung torsion and pulmonary vasc prob, and a retrospective crossmatch to exclude humoral rejection. n
ECMO Initiate 21 days (740 days) Initiated after 0 -2 days
ECMO
CASE n One of your keen residents asks if there is anyway this could be acute rejection? Are there any definitive tests to prove this is not rejection?
Biopsy!! n n Patients with acute rejection can also have alveolar infiltrates, hypoxemia and systemic inflammatory response syndrome. To rule out hyperacute rejection can do a retrospective crossmatch. For longer term observation pathologic assessment of multiple transbronchial biopsy specimens has proven to be the gold standard. Debate between transbronchial and surgical biopsy. Trulock et al. Chest. 1992; 102: 1049 -1054.
Open Lung Biopsy n n n In 2003 Burns et al looked at 41 patients on mech vent with questionable acute rejection that received transbronchial and open lung biopsy. Surgical biopsy inc dx of rejection by 33% and treatment changes in 15 of the 41. Currently unresolved debate as previous studies contradicted this finding. Burns et al. J Heart Lung Transplant 2003; 22: 267 -275.
Open Lung Biopsy The risk of open lung biopsy must be weighed against the risk of simple empirical therapy for rejection after exclusion of infection. n Given the consequences of intensification of immunosuppression in the intubated, critically ill px, open lung biopsy may be justifiable. n
CASE n Now that the possibility of rejection has been brought up…. . what are the different types of rejection? How are they treated?
Rejection Hyperacute- humoral based with preformed antibodies to the allograft vascular endothelium - Only anecdotally reported in the literature with lung transplant. Cellular immune based rejections n Acute n Chronic/bronchiolitis obliterans syndrome (BOS) n
Rejection n n Standard immunosuppressive management: Triple drug combo=cyclosporin, imuran, prednisone. Methylprednisolone intraop and first 24 hrs. Then steroids suspended for 2 weeks, based on experimental and clinical evidence they impede bronchial anastamotic healing. Then oral pred started. Some evidence tacrolimus/imuran/steroid may be a better combo. (acute and chronic rejection)
Rejection Acute: n Most common complication following lung transplantation. n Most recipients experience at least 1 episode in first year. n It is clear that there is a association between frequency and severity of acute rejection and subsequent dev of BOS. n
Rejection n n n Thus, early detection and alteration of immunosuppression may have a significant impact on subsequent reduction of BOS. S/S: Fever Dyspnea Dec Pa. O 2 Fall in vital capacity Infiltrates.
Rejection After first postop month, CXR freq normal during episode of acute rejection. n Obviously, infection can present similarly. n Need to distinguish with transbronch biopsy and BAL. n Tx: n Methylprednisolone 10 -15 mg/kg for 3 -5 days. n 2 -3 weeks of oral steroid taper. n
Rejection Some work by Loubeyre et al, that may be able to use HDCT to Dx acute rejection and avoid TBB (65% sens for rejection, 85% specific for acute lung complication.
Rejection Maintenance immunosuppression regimen should also be scrutinized. n First adjustment from maintenance cyclosporine is a switch to tacrolimus in event of cyclosporin toxicity or acute rejection episodes despite adequate cyclosporine dosage. n Newer agents such as sirolimus, leflunomide may be used more in future. n
Rejection n n Chronic/bronchiolitis obliterans syndrome(BOS): 70% of graft recipients are dx by 5 th year. Usually presents as a late decline in FEV 1 from a post-op baseline. Pathologic lesion is broncholitis obliterans.
Rejection Risk Factors: n Episodes of acute rejection n Primary Graft dysfunction n CMV pneumonia n Noncompliance with meds n
Rejection Causes not totally clear. n Evidence suggests both alloimmune and nonalloimmune mech are important (for example GERD). n There is evidence that fundoplication will lower BOS scores and even eliminate it in certain individuals n Cantu et al. Ann THorac Surg 2004; 78: 1142 -51
Rejection n Diagnosis- two approaches (definitive proof and diagnosis of exclusion)
Rejection Treatment: (no well established protocol) n Conversion from cyclosporin to tacrolimus may stabilize progression. n ? addition of mycophenolate may be benificial. n ? sirolimus n ? azithromycin daily is currently being investigated and may show promise. n Retransplantation? n
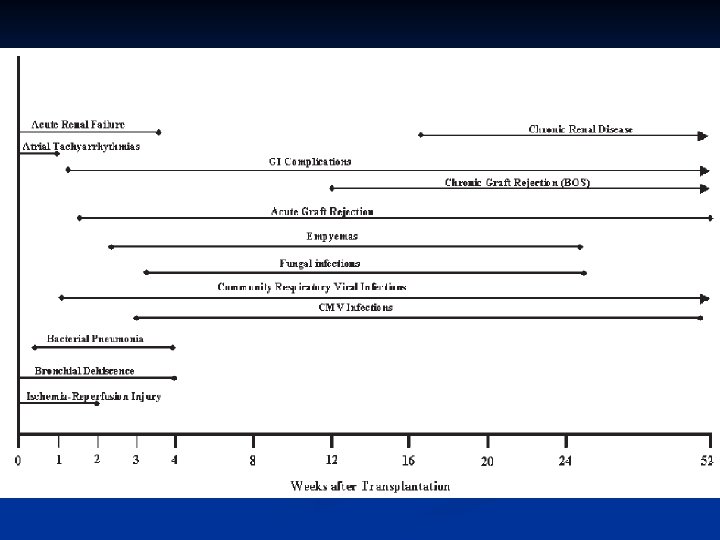
CASE n 17)Could this be infectious? Where in the complications timeline to infectious etiologies usually fit? Are there any exceptions?
Infection post transplant Unlikely in this scenario. n But infection is one of the leading causes of morbidity and mortality. n Immediate post-op bacterial are the greatest threat. n But candidia or aspergillus or viral (herpies or CMV) can also arise. n Lung transplant: procedure and postoperateive management. 2008 Uptodate. com.
Bacterial n n Most common pathogen are those that colonized the donor or recipient. Gram neg such as Pseudomonas, Klebsiella and H. flu are most common. Gram positives (staph) are also a frequent cause (head injury). Most centers use a 7 -10 day prophylaxis (eg vanco, cefepime) or depending on previous colonization. We use generally use ceftaz and clox till lines and drains are out.
Viral n n n CMV is most commonly seen infection post-op complication (13 -75% of transplants). Most risk obviously in CMV neg recipient receiving CMV pos donor. Optimal prophylaxis remains controversial. Most centers will supply 12 weeks of IV gancyclovir (5 mg/kg qd) for +D/-R and CMV immunoglobulin. If just +R get only gancyclovir for 12 weeks. If –D/-R nothing.
Viral Patients in the community are also susceptible to other viral infections (eg. RSV, adenovirus, influenza, parainfluenza). n Several of these have specific treatments so be aware of them (eg. Aerosolized ribavirin) n
Fungal infections Major problem in the long term. n Aspergillus and Candida account for majority. n Both can represent colonization but also can be life-threatening infections. n Aspergillus colonization and infection occur within first 6 months. n Mortality for pneumonia/disseminated disease approaches 60%. n Critical Care Aspects of Lung Transplantation. Journal of Intensive Care Med 19(2); 2004
Fungal infections Several antifungal prophylactic strategies used. n Systemic or inhaled or both. n However, use of systemic antifungal therapies limited by lack of in vitro activity against some infections, drug interactions, significant treatment limiting toxicities. n Several reports of using inhaled Ampho B lipid complex…. may see used in future. n
Fungal infections What do we do? n Candida prophylaxis= nystatin swish and swallow. n PCP= septra or aerosolized pentamidine. n Aspergillus=aerosolized ampho B. n Toxoplasma neg px= pyrimethamine for 6 months. n
Fungal infections n n Although bronchial dehiscence is a rare complication due to improved surgical tech and lack of steroids for period of time after OR. B/c of inherent ischemia occurring at the anastomosis fungal infections my develop at this site. This can lead to life threatening airway complicatoins. Careful attention should be paid to this area on all bronchoscopies.
Fungal infections n n In one study by Nunley it was found that 46. 7% with anastamosis infections had airway complications where in only 8. 7% of patients without. These included bronchial stenosis, bronchomalacia, fatal hemorrhage and dehiscence. Nunley et al. Chest 2002; 122: 1185 -1191.
Fungal infections If on bronchoscopic inspection have pseudomembranes should perform biopsy. n Optimal treatment still unknown. n Suggested expert opinion is that should use combination of systemic and inhaled antifungal agents. (eg. Ampho B) n May need bronchoscopic debridement of the tissue. n
Fungal infections Treatment of systemic infections. n Albicans still fluconazol. n Non-albicans caspofungin. n Ampho B is classic drug of choice for aspergillus and fusarium. More utilization of Vori and caspo in last several years. n Careful with Vori as has extensive interactions with immunosuppressants. n Nunley et al. Chest 2002; 122: 1185 -1191.
CASE n The oxygen delivered via ECMO was adjusted according to the arterial blood gas results, and was successfully reduced to 40% within 4 days. After the first 48 hours, the ECMO flow rate was maintained at 2. 5 L/min, with 3200 RPM. Prior to discontinuation of ECMO, the patient was relying on his lung for oxygenation with no oxygen given through the oxygenator.
CASE n n Both the cannulae were successfully removed with application of pressure on the site and without any problems. The patient did very well there after and was discharged to the ward within 8 days. While on the ward several surveillance bronchoscopies were performed. There were some pseudomembrains seen near the anastomosis and they were sampled. They were positive for candida sp. and treatment initiated with IV caspofungin. The site looked stable during repeated bronchoscopy.
CASE n On day 15 you are called to the ward for respiratory decline. He is in respiratory distress and a CXR is performed.
CASE What is high on your differential for the cause of the abnormality? n The patient requires reintubation, independent lung ventilation and is taken to the OR for repair of his bronchial dehiscence. n Is there any evidence for the outcomes of Lung transplant patients who require readmission to the ICU? n
n n n n All lung transplants at Duke University Medical Center discharged from hosp between March 99 and Feb 01. 51/214 px (23. 8%) required ICU admissions. Of those 27/51 (57. 5%) required MV. Dx: Resp failure (70%) Sepsis (6. 8%) Pneumothorax, atrial fib, high-risk bronchoscopy, PE, antibiotic desensitization and cardiac arrest (2. 7% each)
19/51 (37%) died during their ICU admission. n 16/27 (59%) receiving MV died. n Px who died had lower FEV 1 to posttransplant best FEV 1 ratio prior to ICU admission. (51% vs 75% p=0. 001) n Also, had higher APACHE III scores on ICU admission compared to survivors. n
n n n Survival rates by Kaplan-Meier: 1 year= 43. 1% 2 year= 40. 9%
Conclusions: n ICU admission and mechanical ventilation, is associated with a poor prognosis in lung transplant but…. n Is appropriate for selected patients with good allograft function. n
Conclusions n n More immediate ICU complications with IPAH and IPF. Beware the patient that required by-pass or that did poorly on single lung ventilation. If become shocky…. act quickly and look for the diagnosis. (? Bleeding, STAT TEE, contact surgeon) Reperfusion injury is a diagnosis of exclusion and may require independent lung ventilation or ECMO.
Conclusions n n n Predictors of need for independent lung ventilation include preoperative airflow limitation (FVC 1/FVC) and hyperinflation. Mobilize ECMO early. If questioning diagnosis of acute rejection vs infection use open lung biopsy. Acute rejection is a marker for future BOS…. we may be able to make a difference. Patients with post-op good allograft function should be candidates for readmission to ICU.