Lumbar Spinal Stenosis KTPH Orthopaedics Spine Teaching Anshuja

Lumbar Spinal Stenosis KTPH Orthopaedics Spine Teaching Anshuja Charvi Wadhwa

What is it? 1. Narrowing of spinal canal/neural foramina 2. Compression spinal cord and nerves Why? • Spinal Degeneration • Ageing; common • Inflammatory (Paget’s; AS) • Spinal Disc Herniation • Tumour • Infection • Congenital (Achondroplasia)

Causes of spinal stenosis Osseous structures Osteophytes Soft tissue structures Spondylolisthesis Herniated disc Hypertrophy/buckling of ligamentum flavum Synovial facet cysts

Classification • Etiologic classification • Anatomic classification • Central stenosis • Lateral Recess stenosis • Foraminal stenosis Acquired Congenital Degenerative Achondroplasia Post surgical Short pedicles, medial facets Post Traumatic /# Inflammatory (AS, Paget’s)

Hypertrophied ligamentum flavum Thecal sac compression Bulging discs Central canal stenosis Nerve root compression Superior articular facet overgrowth Intraforaminal disc extrusion Normal Nerve root compression Foraminal stenosis Lateral recess stenosis

Central stenosis Thecal Sac Compression • Structures • Anterior: - Posterior longitudinal ligament, disc • Posterior: - Ligamentum flavum • Laterally: - Medial borders of superior facet • Absolute stenosis: • cross-sectional area <100 mm 2 or • <10 mm of AP diameter on CT cross section • Male spinal canal smaller than female at the L 3 -L 5 level • More common in older population

Lateral recess stenosis Subarticular stenosis/ Entry zone stenosis • Structures • Anteriorly: - Posterolateral vertebral body • Posteriorly: - Superior articular facet • Medially: - Thecal sac • Laterally: - Pedicle • Causes: • Facet joint arthropathy/ superior articular process enlargement • Disc disease • Ligamentum flavum hypertrophy • Vertebral body osteophytes

Foraminal stenosis—nerve root compression • Structures • Anteriorly: - adj vertebral bodies and discs • Superior and inferior: - pedicles • Posteriorly: - facet joint • Laterally: - ligamentum flavum extensions • Causes • Intraforaminal disc protrusion • Superior facet impingement
 dermatomal • Pain, burning radiation")
History • • Back Pain Leg Symptoms (>back pain) dermatomal • Pain, burning radiation from buttock to leg • Weakness +/- foot drop • Tingling • Radiation +ve • Fatigue • Heaviness • Cramps Bladder Symptoms • Recurrent UTIs (due to autonomic sphincter dysfunction) Neurogenic claudication – posture related • Starts proximal extends distal • Worsens on standing or walking • Improves with sitting/ leaning forward • Lying on side more comfortable than lying flat (greater lumbar extension) • Normal vascular examination

Vascular VS Neurogenic Claudication

Examination • <50% have abnormal neurological findings • Limited extension • Kemp sign • Back extension worsening foraminal stenosis unilateral radicular pain • SLR • Valsalva test • holding breath and bearing down > increasing intratechal pressure • Pain worsened if herniated disc

Investigations • • Xrays MRI CT Myelogram EMG/Nerve conduction studies • Sensitivity examiner dependant • Radiculopathy VS peripheral neuropathy

Ix - Xray • Standing AP/Lateral • Degenerative findings • Scoliosis • Spondylolisthesis • Flattening of lordotic curve • Flexion/Extension • Segmental instability

Ix - MRI • Obliteration of perineural fat and compression of lateral foramen • Facet and ligamentum flavum hypertrophy • 3 of 14 asymptomatic patients had MRI findings of anatomic spinals stenosis 1 1. Boden SD, Davis TS, Patronas NJ, Wiesel SW. Abnormal magnetic resonance scans of the lumbar spine in asymptomatic subjects. A prospective investigation. J Bone Joint Surg Am. 1990; 72: 403– 87(7): 694 -703

Ix – CT Myelogram • Central and lateral compression • Osteophytes • Bony facet hypertrophy • Axial CT – trefoil canal • Limitation: - superimposition of multiple spinal structures that contribute to the overall pattern of stenosis Facet Joint Hypertrophy Tight restriction of neuroforaminal recess

Treatment

Non surgical treatment • Physiotherapy • Goal: increase muscular stabilization + correct spine posture • Core strengthening -> abdominal muscles, increase lumbar flexion and reduce lumbar lordosis • Strengthen spine flexion muscles • Stretch spine extension muscles

Non surgical treatment • Weight loss • Bicycling; aquatic exercises • Bracing • Reduce lordosis Improve exercise tolerance • Weakens abdominal and core muscles

Non surgical Intervention • Analgesia

Non surgical intervention • Gabapentin and Pregabalin • • Injury site accumulation of voltage sensitive Ca and Na channel Binds to these channels Inhibits neurotransmitter release Reduces abnormal axonal excitability Reduces pain scores 1 Increase walking distance 1 Reduces in sensory deficits 1 No evidence efficacy of gabapentin vs pregabalin 1. Tran DQ. Lumbar spinal stenosis: A brief review of non surgical management. Can J Anaesth. 2010 Jul; 57(7): 694 -703
 • Provide sympathetic block and vasodilation")
Non surgical Intervention • Epidural injections (LA, steroids) • Provide sympathetic block and vasodilation • Increases blood flow to neural tissue • Steroids reduce inflammatory edema, reduce transmission of nociceptive C fibres and reduce sensitization • 2 RCTs 1, 2 • Short lived Improvement of pain and function (<1 mnth) • No support of steroids to local anaesthetic agents 1. 2. Fukusaki M, Kobayashi I, Hara T, Sumikawa K. Symptoms of spinal stenosis do not improve after epidural steroid injection. Clin J Pain 1998; 14: 148 -51. Koc Z, Ozcakir S, Sivrioglu K, Gurbet A, Kurcukoglu S. Effectiveness of physical therapy and epidural steroid injections in lumbar spinal stenosis. Spine (Phila Pa 1976) 2009; 34: 985 -9

Surgical Intervention • Decompression • Fusion • Interspinous Process Decompression
 • Preserve neurological status • Low")
Goals of Surgery • Improve radicular pain (80%) • Preserve neurological status • Low back pain may not show much improvement after decompression 1, 2, 3 1. 2. 3. Lee JY, Whang PG, Lee JY, Phillips FM, Patel AA. Lumbar spinal stenosis. Instr Course Lect. 2013; 62: 383– 396. Mayer HM. Discogenic low back pain and degenerative lumbar spinal stenosis - how appropriate is surgical treatment? Schmerz. 2001; 15: 484– 491 Farzad OK. Lumbar spinal stenosis: Who should be fused? An updated review. Asian Spine J 2014 Aug; 8(4): 521 -530
 Infection (10%) Blood Clots GA Risks • •")
Surgical risks • • Bleeding (27%) Infection (10%) Blood Clots GA Risks • • • Dural sac tear Failure of bone fusion to heal Failure of screws/rods Nerve injury (2%) Need for further surgery Failure to relieve/ return of symptoms

Decompression

Indications for Surgical Decompression • Neurological function decline • Cons mgx failure for 3 -6 months 1 • Cauda equina / Conus medullaris 1. Lee JY, Whang PG, Lee JY, Phillips FM, Patel AA. Lumbar spinal stenosis. Instr Course Lect. 2013; 62: 383– 396.
 •")
Surgical intervention - Decompression • Open • Complete laminectomy (pedicle to pedicle decompression) • Minimally invasive techniques (MIT) • Hemilaminectomy / Laminotomy

Surgical intervention - Decompression Open Laminectomy • Prone • Jackson table • Radiolucent • 360 rotation • Abdomen hangs free • Wilson frame • Maintains spinal flexion • Continuous chest support 1. Claudio S. Positioning on surgical table. Eur Spine J, 2004 Oct; 13(Suppl 1): S 50 -S 55

Surgical intervention - Decompression Open Laminectomy • Posterior approach • L 4/L 5 interspace at iliac crest • Midline incision between paraspinal muscles • Dissect Fat and Lumbosacral fascia • Detach erector spinae subperiosteally • Dissect down to spinous process and lamina to facet joint 1. Claudio S. Positioning on surgical table. Eur Spine J, 2004 Oct; 13(Suppl 1): S 50 -S 55

Surgical intervention - Decompression Open Laminectomy

Surgical intervention - Decompression Benefits of MIT 1, 2 • Avoid muscle crush injury • Minimize ST injury • Self retaining retractors • No disruption of tendon attachments sites • Utilize known anatomic neurovascular and muscle compartment spaces • Shorter hospital stay, less blood loss, lower mean CK muscle isoenzyme levels, faster recovery rate 3 1. 2. 3. Claudio S. Positioning on surgical table. Eur Spine J, 2004 Oct; 13(Suppl 1): S 50 -S 55 Choll W Kim. The current state of minimally invasive spine surgery. J Bone Joint Surg Am, 2011 Mar 16; 93(6): 582 -596 Yagi M Okada E Ninomiya K Kihara M. Postoperative outcome after modified unilateral approach microendoscopic midline decompression for degenerative spinal stenosis. J Neurosug Spine 2009; 10: 293 -9

Surgical intervention - Decompression MIT 1 • • 1. Incision 2 -3 cm lateral to midline Length of tubular retractor Cobb elevator down to spinal lamina Sub periosteal elevation of muscle away from lamina Serial dilatation of soft tissue Placement of tubular retractor Securing tube with table mounted retractor holder Popov V, Anderson DG. Minimal Invasive Decompression for Lumbar Spinal Stenosis. Advances in Orthopedics. 2012; 2012: 645321. doi: 10. 1155/2012/645321.

Surgical intervention - Decompression MIT 1 • • • 1. Ligamentum flavum separated from lamina Laminotomy with rongeur remove ligamentum flavum Pedicle examined for spinal pathology Superior articular process resected Disc space examined, herniated disc removed Decompression confirmed and haemostasis achieved Popov V, Anderson DG. Minimal Invasive Decompression for Lumbar Spinal Stenosis. Advances in Orthopedics. 2012; 2012: 645321. doi: 10. 1155/2012/645321.

Surgical intervention - Decompression MIT

Surgical intervention - Decompression MIT

Fusion Surgery

Indications for Fusion Surgery 3, 4 • Segmental instability • Degenerative spondylolisthesis • Degenerative scoliosis • Caused by complete laminectomy and/or removal of >50% of facets • Wide disc space >2 mm • > 5 mm displacement or >10 -15 deg rotation on lateral standing flexion-extension lumbosacral radiographs • Slippage > 25% 1. 2. 3. 4. Farzad OK. Lumbar spinal stenosis: Who should be fused? An updated review. Asian Spine J 2014 Aug; 8(4): 521 -530 Epstein NE. Decompression in the surgical management of degenerative spondylolisthesis: advantages of a conservative approach in 290 patients. J Spinal Disord. 1998; 11: 116– 122. Chen YM, Jin AM, Zhang H, Zhu LX, Min SX, Zhang L. Indication of fusion for degenerative lumbar spinal stenosis treated by "windows technique" laminoforaminotomy. Zhonghua Wai Ke Za Zhi. 2010; 48: 31– 34. Carreon LY, Glassman SD, Howard J. Fusion and nonsurgical treatment for symptomatic lumbar degenerative disease: a systematic review

Surgical Intervention – Types of Fusion • Posterolateral fusion • Bone graft between transverse processes • Anterior/Interbody fusion • Bone graft between vertebral body usually occupied by disc • Fusion between endplates

Surgical Intervention – Types of Fusion • Types of Interbody fusion • Transforaminal lumbar interbody fusion (TLIF) • Posterior lumbar interbody fusion (PLIF) • Anterior lumbar interbody fusion (ALIF) • Transpsoas interbody fusion • Xtreme lateral interbody fusion (XLIF) • Direct lateral interbody fusion (DLIF) • Oblique lumbar lateral interbody fusion (OLLIF)

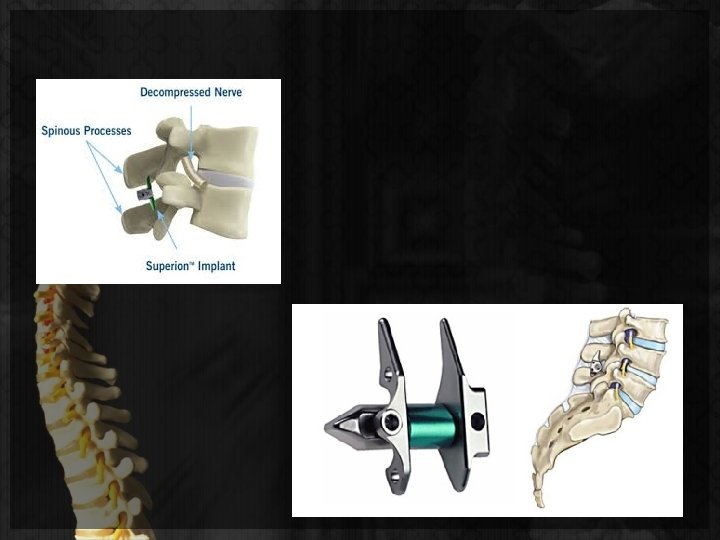
Interspinous Process Devices

Interspinous process devices 1, 2, 3, 4 • Interspinous process devices/spacers, inserted between the spinous processes in the back of the spine. • spread vertebrae apart and preserve space for nerves. • Prevents hyperextension of spine • Minimally invasive surgical option • Indicated if pain relief sitting/bending and pain aggravated upon standing • Xstop and Coflex 1. 2. 3. 4. Davis RJ, Errico TJ, Bae H, et al. Decompression and Coflex interlaminar stabilization compared with decompression and instrumented spinal fusion for spinal stenosis and low-grade degenerative spondylolisthesis: two-year results from the prospective, randomized, multicenter, Food and Drug Administration Investigational Device Exemption trial. Spine (Phila Pa 1976). 2013 Aug 15. 38(18): 1529 -39. [ Davis R, Auerbach JD, Bae H, et al. Can low-grade spondylolisthesis be effectively treated by either coflex interlaminar stabilization or laminectomy and posterior spinal fusion? Two-year clinical and radiographic results from the randomized, prospective, multicenter US investigational device exemption trial: clinical article. J Neurosurg Spine. 2013 Aug. 19(2): 174 -84. Kim HY, Choi BW. Change of radiological parameters after interspinous implantation (X-stop®) in degenerative spinal stenosis. Eur J Orthop Surg Traumatol. 2013 Apr. 23(3): 281 -5. Stromqvist BH, Berg S, Gerdhem P, et al. X-stop versus decompressive surgery for lumbar neurogenic intermittent claudication: randomized controlled trial with 2 -year follow-up. Spine (Phila Pa 1976). 2013 Aug 1. 38(17): 1436 -42.
 • 4 -year follow-up •")
Surgical outcomes • Spine Patient Outcomes Research Trial (SPORT) • 4 -year follow-up • Operative VS Conservative mgx • Both groups had improvements from baseline • Greater improvements in primary outcome measures for operative group • SF-36 Bodily Pain and Physical Function and Oswestry Disability Index 1. And a 8 year follow up. Refer to SPORT presentation

Surgical Outcomes • Försth et al Study 1 • 247 Pts with LSS, with or without spondylolisthesis • Decompressive surgery VS decompressive + fusion surgery • No difference in effectiveness • @2 yr f/up: - no significant difference in mean Oswestry Disability Index score • @5 yr f/up: - no significant difference in Clinical outcomes 1. Forsth P, Olafsson G, Carlsson T, et al. A Randomized Control Trial of Fusion Surgery for Lumbar Spinal Stenosis. N Engl J Med. 2016 Apr 14. 374 (15): 1413 -23.

Thank you
- Slides: 45