Lower respiratory tract infections LRTI BRONCHIOLITIS EPIDEMIOLOGY Annual

Lower respiratory tract infections LRTI

BRONCHIOLITIS

EPIDEMIOLOGY Annual incidence is 11. 4% in children younger than 1 year and 6% in those aged 1 -2 years. Incidence peaks in those aged 2 -8 months 95% have serologic evidence of past (RSV). ; presence of antibodies to RSV does not confer immunity. Incidence of bronchiolitis winter months in temperate climates and during the rainy season in tropical climates. Hospitalization -2% of cases under 6 months Mortality rate is 1 -2% of all hospitalized patients and 3 -4% for patients with underlying cardiac or pulmonary disease.

EPIDEMIOLOGY Accounts for 60% of all lower respiratory tract illness in the first year of life!
.")
Bronchiolitis young infants, aged 2 -24 months. viral infection of the small airways (bronchioles). increased mucus secretion, cell death followed by a peribronchiolar lymphocytic infiltrate and submucosal edema debris and edema produce narrowing and obstruction of small airways. decreased ventilation in the lung causes ventilation/perfusion mismatching and hypoxia. in expiratory phase of respiration, further dynamic narrowing of the airways produces disproportionate airflow decrease and resultant air trapping.

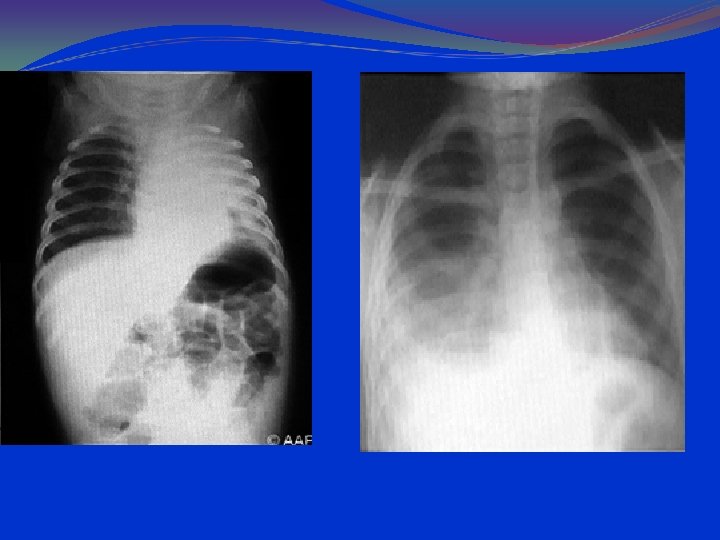
Pathophysiology The virus spreads from the upper respiratory tract to the medium and small bronchi and bronchioles, causing epithelial necrosis and initiating an inflammatory response. The developing edema and exudate result in partial obstruction, which is most pronounced on expiration and leads to alveolar air trapping. Complete obstruction and absorption of the trapped air may lead to multiple areas of atelectasis

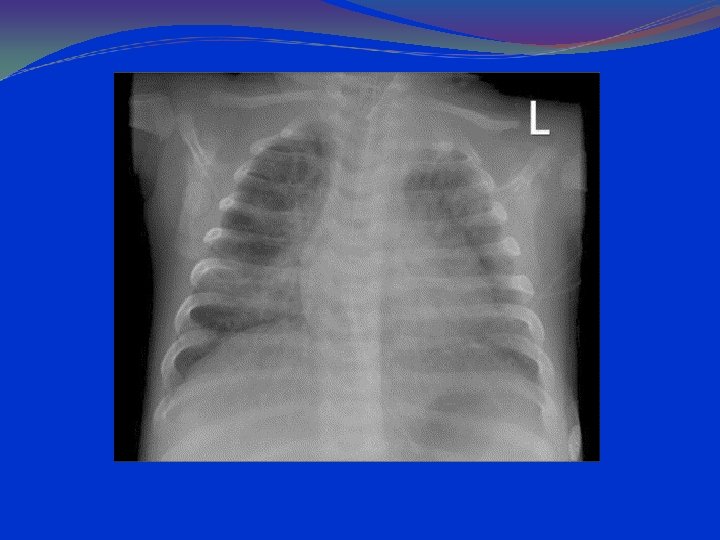
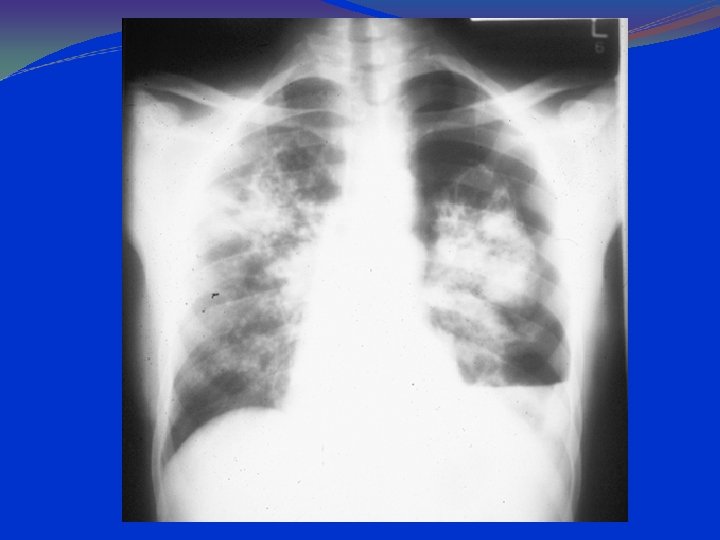
lung hyperinflation with a flattened diaphragm and bilateral atelectasis in the right apical and left basal regions

RISK FACTORS OF SEVERITY Prematurity Low birth weight Age less than 6 -12 weeks Chronic pulmonary disease Hemodynamically significant cardiac disease Immunodeficiency Neurologic disease Anatomical defects of the airways Older siblings Concurrent birth siblings Passive smoke exposure Household crowding High altitude

ETIOLOGY Typically caused by viruses RSV-most common Parainfluenza Human Metapneumovirus Influenza Rhinovirus Coronavirus Human bocavirus Occasionally associated with Mycoplasma pneumonia infection

Clinics Early symptoms are those of a viral URTI, including rhinorrhea, cough, and sometimes low-grade fever. paroxysmal cough and dyspnea develop within 1 -2 days. Fever Increased work of breathing Wheezing Cyanosis Grunting Noisy breathing Vomiting, especially post-tussive Irritability Poor feeding or anorexia
 Tachycardia Fever, usually")
Clinics Physical Tachypnea, over 50 -60 breaths per minute (most common) Tachycardia Fever, usually in the range of 38. 5 -39°C Mild conjunctivitis, otitis, pharyngitis Diffuse expiratory wheezing Nasal flaring Intercostal retractions Cyanosis Inspiratory crackles Apnea, especially in infants younger than 6 weeks Palpable liver and spleen from hyperinflation of the lungs and consequent depression of the diaphragm

DIFFERENTIAL DG Asthma Gastric reflux with aspiration of gastric contents also may cause the clinical picture of bronchiolitis; multiple episodes in an infant may be clues to this diagnosis. Bronchitis Congestive Heart Failure and Pulmonary Edema Mycoplasma Apnea Pneumonia Cystic fibrosis Vascular ring Lobar emphysema Foreign body Cardiac disease Reflux Aspiration
 with white blood cell (WBC) count within")
LABORATORY AND IMAGISTICS Complete blood count (CBC) with white blood cell (WBC) count within normal limits. 2/3 of the children have WBC counts of 10, 000 to 15, 000/μL. Most have 50 to 75% lymphocytes Serum chemistries may be affected in dehydration. Arterial blood gases (ABG) in severely ill patients, with mechanical ventilation. Chest radiographs should include anterior-posterior (AP) and lateral views. Hyperinflation and patchy infiltrates ; these findings are nonspecific and may be observed in asthma, viral or atypical pneumonia, and aspiration. Focal atelectasis Air trapping Flattened diaphragm Increased anteroposterior diameter

RSV rapid antigen testing done on a nasal swab or washing is diagnostic but not generally necessary; it may be reserved for patients with illness severe enough to require hospitalization. A positive culture or direct fluorescent antibody test result can confirm the diagnosis of RSV infection

COURSE Depends on co-morbidities Usually self-limited Symptoms may last for weeks but generally back to baseline by 28 days In infants > 6 months, average hospitalization stays are 3 -4 days, symptoms improve over 2 -5 days but wheezing often persists for over a week Disruption in feeding and sleeping patterns may persist for 2 -4 weeks

Prognosis is excellent. Most children recover in 3 to 5 days without sequelae, although wheezing and cough may continue for 2 to 4 wk. Mortality is < 1% when medical care is adequate. Bronchiolitis has been identified as a risk factor for asthma, but the association is controversial and the incidence seems to decrease as children age.

Treatment Supportive therapy O 2 supplementation as needed IV hydration as needed Indications for hospitalization include accelerating respiratory distress, ill appearance (eg, cyanosis, lethargy, fatigue), apnea by history, hypoxemia inadequate oral intake. children with underlying disorders such as cardiac disease, immunodeficiency, or bronchopulmonary dysplasia, which put them at high risk of severe or complicated disease, also should be considered candidates for hospitalization

In hospitalized children, 30 to 40% O 2 by tent or face mask is usually sufficient to maintain O 2 saturation > 90%. Endotracheal intubation is indicated for severe recurrent apnea, hypoxemia unresponsive to O 2 therapy, or CO 2 retention or if the child cannot clear bronchial secretions. Hydration maintained with frequent small feedings of clear liquids. For sicker children, fluids should be given IV initially, and the level of hydration should be monitored by urine output and specific gravity and by serum electrolyte determinations. There is little evidence that systemic corticosteroids are beneficial
 occurs.")
Antibiotics should be withheld unless a secondary bacterial infection (a rare sequela) occurs. Bronchodilators are not uniformly effective some children may respond with short-term improvement. This is particularly true of infants who have wheezed previously. RIBAVIRIN active in vitro against RSV, influenza, and measles, is toxic RSV immune globulin has been tried Prevention of RSV infection by passive immunoprophylaxis with monoclonal antibody to RSV ( palivizumab ) SYNAGIS decreases the frequency of hospitalization but is costly and is indicated primarily in high-risk infants

RESPIRATORY PHYSIOTHERAPY NEBULISATIONS WITH: Epinephrine: 0. 01 m. L (ie, 0. 01 m. L/kg of 1: 1000 solution [1 mg/m. L]) SC q 15 -20 min, not to exceed 0. 3 m. L/dose Racemic epinephrine: <2 years: 0. 25 m. L of 2. 25% solution via nebulizer diluted in 3 m. L NS >2 years: 0. 5 m. L of 2. 25% solution via nebulizer diluted in 3 m. L NS ALBUTEROL, VENTOLINE 90 mcg; 4 -8 inhalations q 20 min up to 4 h, then q 1 -4 h prn; use with a spacer device

NONSTANDARD THERAPIES Heliox Mixture of helium and oxygen that creates less turbulent flow in airways to decrease work of breathing Only small benefit in limited patients Anti-RSV preparations RSV-IGIV or Palivizumab No improvement in outcomes Surfactant May decrease duration of mechanical ventilation or ICU stay

COMPLICATIONS Highest in high-risk children Apnea Most in youngest children or those with previous apnea Respiratory failure Around 15% overall Secondary bacterial infection Uncommon, about 1%, most in children requiring intubation

PNEUMONIA

EPIDEMIOLOGY • The WHO Child Health Epidemiology Reference Group estimated an annual incidence of 150. 7 million new cases, of which 11 -20 million (7 -13%) are severe enough to require hospital admission. 95% of all episodes of clinical pneumonia in young children worldwide occur in developing countries

PATHOPHISIOLOGY Inflammation of the alveolar space and may compromise air exchange. Often complicating other lower respiratory infections such as bronchiolitis or laryngotracheobronchitis, pneumonia may also occur via hematogenous spread or aspiration. Most commonly, this inflammation is the result of invasion by bacteria, viruses, or fungi, but it can occur as a result of chemical injury or may follow direct lung injury

PATHOLOGY Bronchopneumonia is a patchy consolidation involving one or more lobes. The neutrophilic exudate is centered in bronchi and bronchioles, with centrifugal spread to the adjacent alveoli. In interstitial pneumonia, patchy or diffuse inflammation involving the interstitium is characterized by infiltration of lymphocytes and macrophages. The alveoli do not contain a significant exudate Bacterial superinfection of viral pneumonia can also produce a mixed pattern of interstitial and alveolar airspace inflammation.

Four stages of lobar pneumonia In the first stage, within 24 hours of infection, microscopically by vascular congestion and alveolar edema. Many bacteria and few neutrophils are present. 2. The stage of red hepatization (2 -3 d) similar to the consistency of liver: presence of many erythrocytes, neutrophils, desquamated epithelial cells, and fibrin within the alveoli. 3. In the stage of gray hepatization (2 -3 d), the lung is graybrown to yellow because of fibrinopurulent exudate, disintegration of red cells, and hemosiderin. 4. The final stage of resolution : resorption and restoration of the pulmonary architecture. Fibrinous inflammation may extend into the pleural space, causing a rub heard by auscultation, (resolution or to organization and pleural adhesions) 1.

ETIOLOGY Bacteria accounted for 60%, of which 73% were due to Streptococcus pneumoniae; Mycoplasma pneumoniae and Chlamydia pneumoniae were detected in 14% and 9%, respectively. S pneumoniae, S aureus H influenzae are by far the most common bacterial pathogen in 1 -3 years age group Enterococci Newborns: group B Streptococcus, gram-negative rods (E. coli, Klebsiella pneumoniae), Lysteria monocytogenes Chlamydia trachomatis, U urealyticum, Mycoplasma hominis, Treponema pallidum Toxoplasma gondi

Viruses that cause acute pneumonia Øadenovirus Øcoronavirus Øinfluenza A and B viruses Øparainfluenza virus Ørespiratory syncytial virus Øcoxsackievirus A 21 Ørhinovirus

BACTERIA THAT CAUSE PNEUMONIA GRAM POSITIVE COCCI 1. Streptococcus Pneumoniae the most common 2. Streptococcus Pyogenes 3. Streptococcus Agalactiae

ETIOLOGY OF BACTERIAL PNEUMONIA S- Pneumoniae generally resides in the nasopharynx and is carried asymptomatic in approximately 50% of healthy individuals. A strong association exists with viral illnesses, such as influenza. Viral infections increase Pneumococcal attachment to the receptors on activated respiratory epithelium. Once aerosolized SP go from the nasopharynx to the alveolus, Pneumococci infect type II alveolar cells, multiply in the alveolus and invade alveolar epithelium. Pneumococci spread from alveolus to alveolus through the pores of Kohn, thereby producing inflammation and consolidation along lobar compartments

Patients with pneumococcal pneumonia may produce bloody or rust-colored sputum Streptococcus agalactiae is a commensal organism in the genital tract and it can cause pneumonia in newborns which inhale fluid containing the bacteria during its journey down the birth canal and develops pneumonia soon after birth. Staphylococcus aureus is gram positive organism, affecting children and old people. as well as extreme ages. it can produce thin walled air filled cavities ("pneumatoceles") Staphylococcal pneumonia is diagnosed by finding typical clusters of Gram-positive cocci by microscopy and subsequently a growth of Staphylococcus aureus in a purulent sputum that often appears creamy and bloodstained.
 Commonly following influenza in debilitated patients and in")
Staphylococcal pneumonia and bronchopneumonia ( cont’) Commonly following influenza in debilitated patients and in those with cystic fibrosis. Abcess formation is very common. The abcesses are thin walled, multiple and commonly bilateral giving rise to patchy bronchopneumonia.
 when they grow and reproduce")
Some strains of staphylococcal bacteria produce toxins (poisons) when they grow and reproduce on food. Contaminated food with staphylococcal bacteria and these toxins can cause staphylococcal food poisoning. The toxins can also cause scalded skin syndrome and, very occasionally, toxic shock syndrome

Bacteria gram positive rods 1. Bacillus anthracis 2. Nocardia sp 3. Actinomyces sp. Bacteria Gram Negative cocci 1. Neisseria meningitidis 2. Moraxella catarrhalis Bacteria gram negative rods 1. Klebsiella pneumoniae

Bacillus anthracis is Anthrax or Wool-Sorters disease Associated with wool sorting, with animal handlers, and veterinarians, produces eschar Nocardia sp Beaded filamentous rod shaped bacteria, Pleura and chest wall involvment Actinomyces sp. Beaded filamentous rod shaped bacteria, causing rib destruction, cutaneous sinuses, cavitation, spreads to pleura and chest wall.
 cause epidemics in schools, adolescents. Klebsiella pneumoniae produces Current Jelly")
Neisseria meningitidis (meningococci) cause epidemics in schools, adolescents. Klebsiella pneumoniae produces Current Jelly sputum, more commonly seen in patients with cronic cardiopulmonary ilness, immunocompromised. Also called (friedlanders bacillus) Severe form of pneumonia with high mortality Upper lobes being most affected with massive lobar consolidation Sputum is jelly like and blood stained producing (current jelly sputum).

2. Pseudomonas aeruginosa produces green sputum, abscess formation, Common cause of pneumonia in cystic fibrosis and those with severely compromised respiratory defenses. 3. Acinetobacter sp. often found on respiratory therapy equipment and on human skin very difficult to treat due to multiple drug resistance. 4. Burkholderia pseudomallei exposure with contaminated soil 5. Francisella tularensis , Tularemia Infection is via tick bite or contact with contaminated rabbits. 6. Hemophilus influenzae more commonly seen in patients with COPD, alcoholics, and the elderly. 7. Bordetella pertussis Whooping cough

ANAEROBIC BACTERIA • Bacteroides • Fusobacterium • Porphyromonas • Prevotella • Actinomyces • Bifidobacterium • Clostridium • Peptostreptococcus • Propionibacterium

Gram-Negative Bacteria E-coli, Salmonella, Pseudomonas, Moraxella, Helicobacter, Stenotrophomonas, Legionella, Along with the above mentioned bacteria, there are several other type of Gram-Negative bacteria such as Hemophilus influenzae (also known as Bacillus influenzae), Neisseria Meningitidis, Moraxella Catarrhalis, Neisseria Gonorrhoeae, Acinetobacter Baumanii (which comes under Nosocomical Gram-Negative bacteria group).

Fungal Pneumonia Endemic fungi Histoplasmosis Blastomycosis Cryptococcosis Sporotrichosis - primarily a lymphocutaneous disease, but can involve the lungs as well Aspergillus Candida Coccidiodomycosis Histoplasmosis All Chickens, bats, river valleys Coccidioidomycos All California, Southwest USA

Coccidioides immitis: Pneumonia may develop after travel to the southwestern United States and after exposure to a wind or rain storm in an endemic area. Blastomyces dermatitidis: Patients may have traveled to the midwestern United States or the Canadian Shield.

Protozoal Pneumonia Parasites causing pneumonia are 1. Toxoplasma gondii 2. Strongyloides stercoralis 3. Ascariasis. 4. Cryptosporidia 5. Hookworms A variety of parasites can affect the lungs. These parasites enter the body through the skin or by being swallowed, they travel to the lungs, usually through the blood. The eosinophils, responds hihgy to parasite infection. Eosinophils in the lungs can lead to eosinophilic pneumonia.
 Rocky mountain spotted fever, scrub typhus, rickettsialpox")
Rickettsial Pneumonia Typhus fevers (epidemic and endemic) Rocky mountain spotted fever, scrub typhus, rickettsialpox Louse-borne flea-borne through rats and mouse fleas

Rickettsial Pneumonia Q fever ranging from multiple segmental opacities to pleural effusion, lobar consolidation, or linear atelectasis. Hepatosplenomegaly is a common finding; it usually is accompanied with elevation of liver enzymes Rickettsia pneumonia cannot be distinguished clinically, radiologically, or histologically from atypical pneumonia.

ATYPICAL BACTERIA These are the bacteria's that will be called as atypical bacteria and causing also atypical pneumonias like other viral agents etc. and constitute following organisms Legionella Mycoplasma pneumoniae Chlamydia trachomatis an afebrile pneumonia, usually seen in 2 wk to 6 months of age Chlamydia psittaci Chlamydia pneumoniae , Chlamydia trachomatis This is a sexually transmitted disease that may also cause pneumonia and bronchitis. It usually is a subacute infection of early infancy producing a sudden cough and eosinophilia without fever that lasts from 1 -3 weeks, but it may occur in adults too.

Etiology of Pneumonia in Hospitalized Children – Streptococcus pneumoniae 73% – Mycoplasma pneumoniae 23% – Chlamydia pneumoniae 13% – Mycobacterium tuberculosis 2%

Features of viral Pneumonia Strikes primarily in the fall and winter and tends to be more serious in people with cardiovascular or lung disease. Usually starts with a dry (nonproductive) cough fever , headache, sore throat, dry cough, malaise, running nose, common cold, aches and pains precedes several days before viral pneumonia ; In viral pneumonia onset is less abrupt Leucocyte count is usually normal or low • On x ray may show features of interstitial or of atypical pneumonia • Course is mild and self limiting and resolves by 7 -10 days time l Diagnosis confirmed by isolation of virus and serological tests

Features of Bacterial Pneumonia Onset is often sudden High grade fever Rigors and chills Sputum is rusty coloured or blood stained

CLINICS Neonates The infant may present with tachypnea; grunting, flaring, and retractions; lethargy; poor feeding; or irritability. Fever may not be present in newborns; however, hypothermia and temperature instability may be observed. Cyanosis may be present in severe cases. Nonspecific complaints, such as irritability or poor feeding, may be the presenting symptoms. Cough may be absent in the newborn period. Early-onset group B streptococci infection usually presents via ascending perinatal infection as sepsis or pneumonia within the first 24 hours of life. Chlamydia trachomatis pneumonia should be considered in infants aged 2 -4 weeks and is often associated with conjunctivitis.

Infants After the first month of life, cough is the most common presenting symptom. Infants may have a history of antecedent upper respiratory symptoms. Depending upon the degree of illness, tachypnea, grunting, and retractions may be noted. Vomiting, poor feeding, and irritability are also common. Infants with bacterial pneumonia often are febrile, but those with viral pneumonia or pneumonia caused by atypical organisms may have a low-grade fever or may be afebrile. The child's caretakers may complain that the child is wheezing or has noisy breathing.

Toddlers and preschool children A history of antecedent upper respiratory illness is common. Cough is the most common presenting symptom. Vomiting, particularly post-tussive emesis, may be present. Chest pain may be observed with inflammation of or near the pleura. Abdominal pain or tenderness is often seen in children with lower lobe pneumonia and replaces chest pain! The presence and degree of fever is dependent upon the organism involved.

Older children and adolescents Atypical organisms, such as Mycoplasma, are more common in this age group. In addition to the symptoms observed in younger children, adolescents may have other constitutional symptoms, such as headache, pleuritic chest pain, and vague abdominal pain. Vomiting, diarrhea, pharyngitis, and otalgia/otitis are other common symptoms.

PHISICAL EXAM respiratory distress, hypoxemia, and hypercarbia grunting, flaring, severe tachypnea, and retractions assessment of oxygen saturation by pulse oximetry Visual inspection - respiratory effort and count the respirations – tachypnea Auscultation -crackles or rales Percussion -identify an area of consolidation. rashes and pharyngitis

IMAGERY The typical radiological finding is a homogenous, non -segmental, circumscribed consolidation of lung tissue. The opacities are situated anywhere in the lungs, although they are located most often in the basal segments, and are unifocal or multifocal. An air bronchogram is often seen and is considered to be characteristic of pneumococcal pneumonia. The affected segments of the lung are not reduced in volume. Pleural involvement (pleural effusion) is not usual
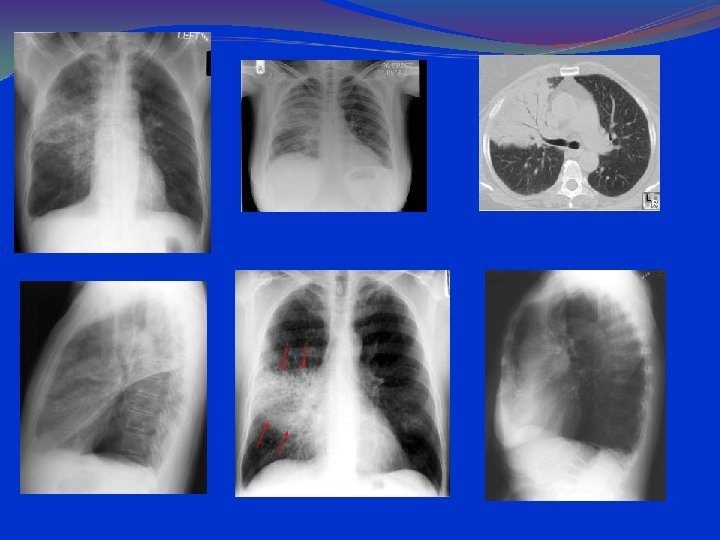

CLINICAL FORMS Broncho-Pneumonia Common cause is staphylococcal infection. Bronchopneumonia is characterized by patchy exudative consolidation of lung parenchyma due to terminal bronchiolitis with consolidation of peribronchial alveoli. Bilateral (less often unilateral), patchy consolidation with intervening normal lung tissue. Lesion is more extensive at the base of the lung and often fuses together resembling lobar pneumonia (confluent bronchopneumonia).

Transverse thin-section CT scan at the level of the carina in a patient with measles infection shows multiple centrilobular nodules (arrowhead) and bilateral areas of lobular consolidation (arrows). Franquet T Radiology 2011; 260: 18 -39 © 2011 by Radiological Society of North America



Staphylococcal Pneumonia in Children • Pneumonia caused by S. aureus associated with high rate of complications (e. g. , pleural effusion or empyema in 55 -80%; pneumothorax, pyopneumothorax, and pneumatoceles frequently observed) • Very high mortality rates reported in primary staphylococcal pneumonia

CLINICS TOXIC SYMPTOMS: Toxic shock syndrome is caused by toxins secreted by Staph aureus. Toxic shock syndrome is characterized by the sudden onset of high fever, vomiting, diarrhea, and muscle aches, followed by low blood pressure which can lead to shock and death. There may be a rash with peeling of skin.

FUNCTIONAL: Dyspnea Chest discomfort Pleuritic pain Chest splinting Cough productive of purulent or blood-tinged sputum Tachypnea Tachycardia In advanced cases you may see: Cyanosis Confusion Pain referral to the abdominal region due to diaphragmatic inflammation

PHYSICAL SIGNS respiratory distress, hypoxemia, and hypercarbia grunting, flaring, severe tachypnea, and retractions assessment of oxygen saturation by pulse oximetry Visual inspection - respiratory effort and count the respirations – tachypnea Auscultation -crackles or rales Percussion -identify an area of consolidation. rashes and pharyngitis

IMAGERY INTERSTITIAL CONDENSATIONS CONFLUATION PROGRESSION TO ABCESS, EMPIEMA Restitutio ad integrum or pneumatocelae

Gram negative infections are caused by Klebsiella pneumoniae, Escherichia coli, Pseudomonas aeruginosa, Haemophilus influenzae, and Proteus. The radiological picture is identical, and it is not possible to differentiate between bacteria. Gram negative lung infections are seen in chronically ill patients , chronic lung diseases, diabetes, or different types of cancer. Aspiration to the respiratory tract is the commonest single cause of Gram negative pneumonia. Opacities caused by Gram negative bacteria are usually localized in the basal lung segments. It is not possible to differentiate these opacities from those caused by staphylococcus aureus. Complications such as empyema and lung abscess are frequently seen

Atypical or Interstitial or viral Pneumonia Causes Mycoplasma Legionella Chlamydia Pneumocystis carinni. Coxiella Fungi Histoplasma capsulatum (histoplasmosis) Coccidioides immitis (coccidioidomycosis

Atypical or Interstitial or viral Pneumonia In atypical pneumonia the x ray finding usually do not show lobar type of picture but meaning that the affection is restricted to small areas that is interstitial spaces between alveoli, rather than involving a whole lobe. As the disease progresses, however, the look can tend to be lobar pneumonia. There is also absence of leukocytosis. Extrapulmonary symptoms, give some clue to the causing organism.

Atypical or Interstitial or viral Pneumonia In atypical pneumonia : x ray chest infiltration, commonly begins in the perihilar region (where the bronchus begins) and spreads in a wedge- or fan-shaped fashion toward the periphery of the lung field. Reticular shadows as small linear striations running in all directions on which may be small white nodular appearance.

Transverse thin-section CT scan at the level of the carina in a patient with measles infection shows multiple centrilobular nodules (arrowhead) and bilateral areas of lobular consolidation (arrows). Franquet T Radiology 2011; 260: 18 -39 © 2011 by Radiological Society of North America


Atypical or Interstitial or viral Pneumonia The most common pathogen of this group is Mycoplasma pneumoniae. It ranks second only to S. pneumoniae. onset is usually more insidious. Mycoplasma pneumoniae can be communicated through close personal contact via respiratory droplets or contact with poultry or birds chicken etc. EXTRAPULMONARY MANIFESTATIONS: gastrointestinal musculoskeletal dermatologic cardiac neurologic symptoms hematological

Complications of Pneumonia 1. Pulmonary fibrosis. 2. Bronchiectasis 3. Lung abscess 4. Empyema 5. Bacteremia with abscess in other organs 6. ARDS 7. Bacteremia 8. Collapse of lung 9. Hemoptysis

Complications of Pneumonia Parapneumonic effusions Septic arthritis Endocarditis Pericarditis Respiratory failure Mental symptoms

Differential Diagnoses Acute Respiratory Distress Syndrome Asthma Bronchiolitis Empyema and Abscess Bronchitis Foreign Body Aspiration Pertussis

Investigations of Pneumonia Total and differential count PBF Blood , urine, sputum culture/sensitivity Gram staining/stain for AFB Fiberoptic bronchoscopy with bronchial washing/ brushing /biopsy

Inflamatory tests: ESR, Fg, CRP, alpha 2 globulin Pulse oximetry Urine latex agglutination test: antigen detection assays for S pneumoniae Blood and sputum cultures Fluid recovered from the pleural space should be sent for Gram stain and culture, along with p. H, glucose, protein, and lactate dehydrogenase (LDH).

IMAGERY

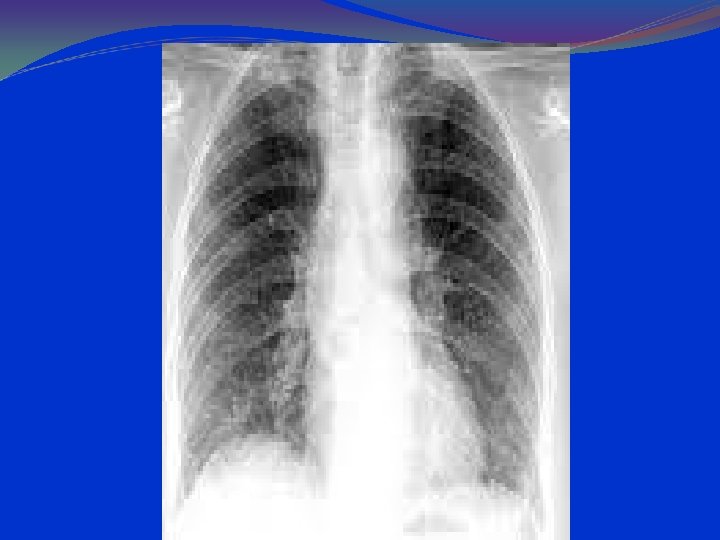
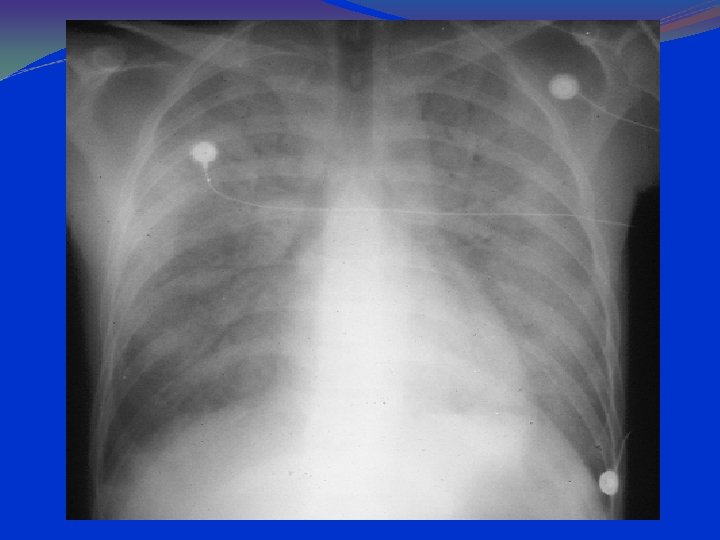
Anteroposterior radiograph of a child with a bacterial pneumonia


parahilar peribronchial infiltrates hilar adenopathy

History of Empiric Therapy Bacterial Pneumonia in Children: • Early 1900’s Serum therapy • 1950’s Penicillin, the miracle drug • 1960’s Ampicillin improves Haemophilus coverage; semisynthetic penicillins (oxacillin, nafcillin) provide Staph coverage • 1980’s 2 nd and 3 rd generation cephalosporins provide excellent coverage for the “usual suspects” • 2010 Are beta-lactams still reliable?

Worldwide Trends in Pneumococcal Resistance

ATB Amoxicillin 80 mg/kg/d PO divided 2 -3 Penicillin 100 ooo units/kg/d iv divided qid or orally Cefuroxime (Zinacef) IV: 150 -200 mg/kg/d IV divided q 8 h Ceftriaxone (Rocephin) 50 -75 mg/kg/d IV/IM qd; not to exceed 1 g Cefotaxime (Claforan) 100 -200 mg/kg/d IV/IM divided q 6 -8 h Erythromycin 30 -50 mg/kg/d (base and ethylsuccinate) PO divided q 6 -8 h

carbapenems, fluoroquinolones, aminoglycosides, vancomycin

Methicillin-resistant Staphylococcus aureus, known as MRSA, is a type of Staphylococcus aureus that is resistant to the antibiotic methicillin and other drugs in the same class, including penicillin, amoxicillin, and oxacillin Therapeutic choice: vancomycin, targocid ( teicoplanin), linezolid ( zyvoxid)
 • Cefotaxime/Ceftriaxone reasonable empiric therapy for pneumococcus,")
Empiric Therapy of Children with Pneumonia (I) • Cefotaxime/Ceftriaxone reasonable empiric therapy for pneumococcus, Haemophilus, Moraxella, MSSA • Add macrolide for coverage of Mycoplasma and Chlamydia in older patients (? ≥ 2 -3 yrs) • Add clindamycin or vancomycin in patients with severe or complicated pneumonia (clindamycin in most cases if low rates of R; vancomycin if life-threatening)

Need to establish specific etiologic diagnosis when possible (e. g. , thoracentesis, culture, molecular diagnostics) • Consider aggressive management of empyema (e. g. , video-assisted thoracoscopic surgery: VATS)
 is a common opportunistic disease that occurs almost exclusively in")
Pneumocystis carinii pneumonitis (PCP) is a common opportunistic disease that occurs almost exclusively in persons who have profound immunodeficiency. PCP was and still is the most common lifethreatening opportunistic infection occurring in patients with HIV disease.

PCP: Clinical Features Cough Usually nonproductive, occasionally whitish sputum. Dyspnea Fever May be accompanied by night sweats, but not rigors. Rales May be present, but are often absent.

Tachypnea and fever Diffuse bilateral alveolar disease can be observed by radiography. Diagnosis requires the identification of P carinii in pulmonary tissue or lower airway fluids. Lung biopsy, inducement of sputum, bronchoalveolar lavage, or needle aspiration of the lung. The Gomori, Giemsa, fluorescence-labelled antibody, or toluidine blue O stains may be used to identify the organism.


PCP: CXR Findings 90 -95% have pulmonary infiltrates. Combined interstitial & alveolar infiltrates. Predominantly at bases and centrally. Pneumothorax can be present. Lace like appearance.

PA Chest Radiograph Demonstrates bilateral, perihilar, R > L, ground glass opacities

PA Chest Radiograph Progressive disease showing extensive ground glass opacification with consolidation

PA Chest Radiograph Progressive disease showing extensive ground glass opacification with consolidation
: Diagnostic Flexible Bronchoscopy with Bronchoalveolar lavage to find")
Histologic Diagnosis Sputum (induced if necessary): Diagnostic Flexible Bronchoscopy with Bronchoalveolar lavage to find pnuemocytis carinii in sputum and secretions. .
 stain from BAL specimen showing “crushed ping-pong ball”")
Diagnosis continued Gomori methenamine silver (GMS) stain from BAL specimen showing “crushed ping-pong ball” appearance of cyst wall

Calcofluor white stains the fungal cyst wall for rapid diagnosis
 and cysts (arrows)")
Diagnosis continued Immunofluorescence showing trophozoites (arrowheads) and cysts (arrows)

• Four drugs currently available for therapy of P carinii pneumonitis are: Pentamidine isethionate Trimethoprim-Sulfamethoxazole atovaquone trimetrevate Trimethoprim-sulfamethoxazole is preferred because of its low toxicity and greater efficacy.

BACTRIM-DS Bactrim DS tablet contains. 160 mg of trimethoprim and 800 mg of Sulfamethoxazole. 21 days course Prednisolone 40 mg bid x 5 days, then 40 mg/day x 5 days, then 20 mg/day to completion of treatment

Alternative Treatments: TMP 15 mg/kg/day PO + dapsone 100 mg/day x 21 days Pentamidine 4 mg/kg/day IV x 21 days -Atovaquone 750 mg PO bid with meal x 21 days PCP is the most frequently identified serious in HIV disease
- Slides: 108