Lower Limb Prosthesis Basic Biomechanical Principles Manipulation of

Lower Limb Prosthesis

Basic Biomechanical Principles Manipulation of ground-reaction- forc Distribution of forces Moments and Lever arm

Distribution of Forces should be distributed over an area as big as possible. Pressure = force/ area P = F/A

Moments and Leverarms A force gives a rotating effect on a point outside the line of action of the force. Moments = Force x Distance The perpendicular distance of force to a point can also be called the Lever- arm.

Manipulation of ground reaction – forces Proper alignment of mechanical joints will give the required stability and control of the prosthesis.

Socket Design The most important part of a prosthesis in the socket If a socket is properly designed and well fitted, taking into consideration where horizontal and vertical forces act on the socket, the prosthesis will be comfortable. (Materials and components used are of lesser importance)

At every level of amputation the prosthesis is confronted with the following Bio-mechanical questions: 1. How can the body weight be transferred from the stump to the prosthesis? 2. How can the forces be optimally distributed? 3. Which moments and horizontal forces are acting on the stump? 4. How and where can optimal fixation from the prosthesis to the stump be realized?

Prosthesis should be: 1 - lightweight 2 -Durable 3 -acceptable cosmetically 4 - easy to clean 5 -easy to don and doff 6 - adjustable

All LL prosthesis include: 1 - shank 2 - socket 3 - suspension systems 4 - Foot ankle assembly 5 - knee unit (for above knee)

Amputation

Causes of Amputation Peripheral Vascular Disease Trauma Cancer Congenital

Aims Rapid healing of the tissues through which amputation performed. Adequate length of stump. Use of residual part to maximum. Rehabilitation of the patient.

Amputation Stump The terminal segment which remains after the amputation. Types: 1 -End bearing Weight is taken by the stump Solid bony end required Scar is not terminal, anterior/posterior E. g. Syme's & Gritti-stokes 2 -Non end bearing (proximal bearing) Weight of the body is transmitted by way of the artificial limb socket to structures other than stump end. E. g. Above knee - by ischial tuberosities, thigh muscles Below knee - Upper end of tibia and knee

Criteria for an Ideal Stump 1 - Stump: Optimum length Firm and smoothly rounded. Conical in shape, tapering distally. Tip of the sectioned bone should be covered with periosteal flap and muscles to increase its vascularity and weight bearing property. 2 -Muscle Adequate flap, not too thin or bulky. Good venous and lymphatic drainage.

3 - Skin Neatly cut and sutured Adequate tension No folds/puckering/dog ears Freely movable on bone and subcutaneous tissue. No inflammation/discoloration. 4 - Scar Well healed Painless Mobile Not terminal in lower limb amputation. Proximal Joint , full range of movement
 Definitive Amputation - where no further operative procedure, expected. Primary")
Types of amputation A) Definitive Amputation - where no further operative procedure, expected. Primary suturing done. B) Provisional Amputation - primary healing is unlikely to occur. Usually heals by granulation. C) Revision Amputation - refashioning of provisional stump

Level of Amputation - influenced by following : a. Healing of stump - which depends on the collateral circulation, colour, and temperature of skin. Growth of hair, bleeding from skin and muscles during surgery suggests good vascularity. b. Age - elderly - more proximal, in children - distal c. Cosmesis d. Return of function, which is better with below knee than above knee.

1 -Single flap Skin flaps 2 -Double flaps 3 -Equal length - terminal scar 4 -Unequal length — scar anterior / posterior If limb is ischemic then flap with better blood supply should be longer. E. g. -Syme's amputation - posterior flap longer Below knee amputation - flaps of equal length Above knee amputation, flaps of equal length In PVD - posterior flap longer

Note: In order that the bone is adequately covered, the combined length of the 2 flaps /1 flap should be atleast 1. 5 times the diameter of the limb at the level of bone section. The shorter flap should be broader than the longer flap so that the skin edges to be sutured are of equal length. Distal part of the flap should have only skin and deep fascia. Proximal part of the flap should have sufficient muscle to cover the bone end.

Muscle - cut just distal to the level of bone, Myodesis - anchoring muscles to the bone. Myoplasty - opposing muscles are joined together over the bone. The above procedures help to achieve better control over the stump and decrease complications of phantom limb. Nerves - are pulled down, cut cleanly with a blade and allowed to retract. Large nerves like sciatic nerve should be ligated with a fine suture before cutting. Blood vessels - all major blood vessels are doubly ligated and the tourniquet released before closure to check for hemostasis. Periosteum - cut at the level of bone. A sleeve of periosteum may be raised to close over the bony stump. Bone - Transversely cut: Edges are beveled.

Postoperative care 3 weeks: remove sutures, start shrinker sock 6 weeks: casting for socket/prosthesis fabrication 8 weeks: start therapy once patient is able to done prosthesis and stand for 15 minutes. 4 -8 weeks of therapy. Consider gabapentin, pregabalin for limb pain / neuroma

Complications 69% phantom limb pain 42% residual limb pain 50% painful neuroma (consider gabapentin, pregabalin)

Rigid Dressing

Soft Dressing

Physical Therapy Examination General medical condition Cognition Emotional state Prior level of function Home situation Skin assessment

Physical Therapy Examination Residual Limb condition Range of motion Strength Neurological exam Phantom limb sensation Phantom pain Functional Status

Treatment interventions 1 -Residual limb care Edema control Residual limb wrapping Possible use of a temporary prosthesis Proper hygiene and skin care Massage

Positioning Contracture prevention and management Therapeutic exercise

Levels of Lower Extremity Amputation

Partial Foot Amputation Toes Amputation of one or more of the lesser toes has relatively little effect on overall foot function; However, loss of the great toe does limit the final toe off.

What do we use? Toe fillers Insoles These devices made of foams with varying degrees of compliance to fill the shoe and redistribute pressure away from the sensitive end of the residuum

Lost Big Toe!! Therefore lost propulsive function add an energy-storing footplate or energystoring rod known as a Morton’s toe extender. Made of carbon fiber usually

Ray Amputations We need to distribute the forces of physical activity over the remaining surface area as evenly as possible first or fifth ray removal lost mediolateral stability. The usual approach is a custom-molded insole, and filler

Transmetatarsal Amputation Done to preserve limb viability Require foot filler
 amputation of the foot between the metatarsus and tarsus midfoot disarticulation removes")
Lisfranc’s (tarsometatarsal) amputation of the foot between the metatarsus and tarsus midfoot disarticulation removes more of the foot’s weight-bearing capability and control of ambulation forces.

Chopart’s Amputation of the foot by a midtarsal disarticulation. Calcaneus and talus remain less surface area over which to distribute weight-bearing forces. Ankle stabilization is generally required. Prothesis should extend to the calf Plastic calf shelf strapped around the leg

Note!!!! Decreased barefoot walking ability due to the loss of the weight bearing metatarsal heads. Elimination of forefoot pronation and supination capability. Increased potential for development of equinus contracture. Loss of inherent roll-over ability of the foot.

Symes Amputation -ankle disarticulation, removal of malleoli, & anchoring heel pad to the wt bearing surface Pros: • End weight-bearing • Short-term household ambulation possible without prosthesis • Self-suspension • Excellent proprioception • Better gait velocity, cadence and Less therapy and training required 1

Cons: • More-complex amputation surgery • Slightly higher wound failure rate • Prosthetic limb is cosmetically larger than contralateral limb
 Canadian: plastic laminated,")
Symes Prosthesis Original: leather socket, steel side bars (not used now) Canadian: plastic laminated, with SACH and removable post wall Removable window design: as before with window cut on medial side to increase strength Flexible post build up: non fenestrated plastic laminated
 Amputation")
Trans. Tibial (below knee) Amputation

Surgical Procedure At the junction of the upper and middle third of tibia Longer residual limb Long LA Gait Hard fit

Prosthetic Prescription

Foot Ankle Assembly Resemble shape of anatomic foot Provide basic function required in walking Shock absorption during heel strike Ankle PF in early stance Stable base in midstance MTP hyperextension in late stance

Non- articulated prosthetic Feet
 No ankle")
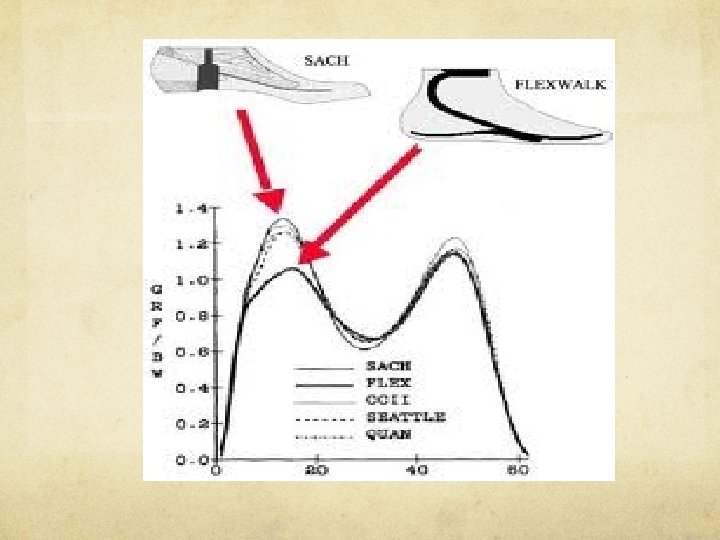
I- Nonenergy- storing prosthetic feet A- SACH Foot (solid ankle cushion heel) No ankle joint Cushioned heelcompresses during heel strike(stimulates PF) Rigid ant keel to roll over during late stance Light weight durable
 Rigid no ankle joint More flexible keel")
B- Stationary attachment flexible endoskeleton foot (SAFE) Rigid no ankle joint More flexible keel to aid in inversion and eversionirregular surfaces Cushioned heel Heavier

II-Dynamic or energy storing feet Keels deform during midstance storing energy Energy released during push off (recoil of keel) Improves function Improves quality of life Eg. Seattle, Sten , Flex foot, Carbon copy II

Articulated Prosthetic Foot

A- Single Axis: Single mechanical axis for PF and DF Limited by Ant and post bumpers Quicker foot flat –stable knee Heavier less durable Used in Transfemoral

B- Multi-axis: Eg Gressinger Allows PF, DF, inversion, eversion and transverse rotation Walking on uneven ground Better shock absorption Heavier, less durable, expensive

So!!!! Foot unit Advantages Disadvantages Posiible uses SACH Inexpensive Light Durable Reliable Energy consuming Rigid Best used on a flat surface General use Children( durable) If ambulation needs are limited Single Axis (1 plane) Adds stability to prosthetic knees Greater weight (70% heaver than SACH) Greater cost To enhance knee stability in AKA quickly goes to flat foot Multiaxis Foot DF, PF, In, Ev, Rot Multidirectional motion Relatively bulky Heavy, Expensive Greater movement uneven surfaces -unstable Relieves stress Ambulation on uneven surfaces SAFE Flexible keel Multidirectional motion Accommodates uneven surfaces Smooth rollover Heavy Greater cost Not cosmetic Greater maintenance Ambulation on uneven surfaces Dynamic Elastic keel Conforms to uneven ground As above

Shanks 1 - Exoskeleton: Harder outer plastic shell Durable Doesn’t allow alignment 2 - Endoskeleton (modular): Pylon covered by soft foam Lighter cosmetic Easily adjusted

Transtibial socket
 Common for TTA Custom molded plastic Bar in ant wall")
Total Contact (PTB socket) Common for TTA Custom molded plastic Bar in ant wall to apply pressure on pat tendon Trimline extends ant to mid patella, mediolaterally to femoral condyles, and post below level of PTB bar Distributes weight through bulges on pressure tolerant areas and away from pressure sensitive areas

Biomechanic of PTB socket As we agree P= F/A To minimize discomfort we must : force applied by thigh corset , crutches etc area by doing total contact socket

Pressure tolerant, pressure sensitive areas We need to increase pressure on tolerant areas We need to decrease pressure on sensitive areas HOW? ?

Advantages of total contact socket Prevents edema and aids venous return Greater area to distribute load Better sensory feedback to the wearer.

Bent knee or kneeling and Bypass Prosthesis Receives pressure from thigh , ischium and gluteus Bypass the tibia Due to severe knee contracture External knee hinges present Bad cosmetically

Transtibial suspensions

Supracondylar cuff suspension 1 - Without fork strap and waist belt Fabric or leather strap grips prox ant patella and around thigh For early prosthetic fitting #in arthritic hands , mediolateral instability, short limb

2 - Supracondylar cuff with fork and waist belt suspension Elastic to allow for knee flexion Active amputees, and vigorous movement

Brim suspensions Supracondylar: PTB with supracondylar wedge mediolateral above femoral condyles Built in or separate wedge looks good Easy to don and doff More expensive

2 Supracondylar/suprapatel lar As before with high anterior socket margin “quadriceps bar” More effective For short residual limb Helps genu recurvatum

Sleeve suspension Neoprene, latex or other elastic With other suspension Suction type effect Not in short residual limb or mediolateral instability

Suction suspension Silicone suction suspension: Flexible molded silicone liner rolled on limb Secured to socket with trasverse pin Suction effect Secure Good skin integrity Good hand dexterity

Joint and Thigh corset suspension Leather thigh corset connected to to prosthesis through metal joints and side bars 40 -60% of bodyweight to thigh For lax knee ligs Gives mediolateral support Bad gait Less knee control

Gait abnormalities Gait cycle phase Gait abnormality Cause Modification Initial contact to loading response -Abrupt heel contact, rapid knee flexion -Prolonged heel contact, knee remains fully extended -Jerky knee motion -Excessive heel lever -Inadequate heel lever or worn-out heel Realign prosthetic foot, change heel stiffness Increase heel stiffness Improp er socket flexion Learned gait pattern. Quadricep s weakness Loose socket, poor alignment Inadequate suspension Realign prosthesis Gait training, gait strengthening

Contd’ Gait cycle phase Abnormality Cause Modification Midstance Medial or lateral socket thrust Lateral trunk shift over prosthesis Pelvis drops or elevates Foot too far outset or inset Loose socket Prosthe sis too short/too long Realign prosthesis Replace socket Adjust socks Adjust length of prosthesis Midstance to terminal stance Early knee flexion or "drop off" Inadequate toe lever Realign prosthesis, replace foot Terminal Stance Heel-off too early Heel-off excessively delayed Excessive toe lever Too much socket flexion Realign prosthesis

Contd’ Gait cycle phase Abnormality Cause Modification Swing phase Foot drags Prosthesis too long Inadequate suspension Shorten limb Modify suspension Successive double support Uneven step length Hip flexion contracture, gait insecurity Uncomfortable socket Physical therapy Adjust socket fit
")
Knee Disarticulation(Through Knee Amputation)

Surgical Procedure Removal of tibia and fibula Advantages all weight onto the end of the stump. The supracondylar area is still intact The socket is Self suspending. The major muscle groups are intact The long stump means long lever arm Disadvantages: Before problem of cosmesis Now, just longer lever arm
 4 bar polycentric knee")
Prosthetic prescription Modified quadrilateral socket Some ischial WB (not necessary) 4 bar polycentric knee used now
amputation")
Transfemoral (aboveknee)amputation

Surgical Procedure Equal Anterior and posterior flaps Doesnot tolerate TWB Myodesis or Myoplasty assist hamstring action

Prosthetic prescription Knee Units: A- Axis: -Single axis – allows flex and ext only. - SIMPLE CHEAP -Polycentric: 4 bar linkage system- more stable , but HEAVY, COSTY

STABILITY OPTIONS Manual lock automatic lock that can be unlocked voluntarily. This is the most stable knee available. Prosthesis shortened 1 cm to allow gait clearance Most stable Weight-Activated Locking Systems “ safety Knee” -First prescription -Spring loaded wedge into groove upon transfer of BW

MOTION CONTROL OPTIONS Constant Friction knee unit -degree of swing control to maintain a consistent gait -provided by mechanical friction at the axis of rotation and is adjusted to match the normal cadence -simple, lightweight and dependable. Disadvantage -single walking speed Variable friction knee unit -Increased resistance as the knee bends from full extension - provides “cadence response, ” allowing variable walking speeds

Contd… Pneumatic control Hydraulic control -compresses air as the knee is flexed, stores the energy, then returns the energy as the knee moves into extension. -For active amputees, -Pneumatic systems are generally considered to provide superior swing control to friction knees but to be less effective than hydraulic systems. -use a liquid medium (usually silicone oil) to respond to a wide range of walking speeds. -provide the closest thing to normal knee function. -provide a smoother gait, -heavier, require more maintenance, costy

Extension Aids Internal extension aid -elastic webbing, tension spring within knee unit External extension aid -Fork strap, kick strap -infront of knee and connected to waist belt - Cheap easy
 - 4 sides and corners - Posterior socket wall")
Sockets Quadrilateral (ischeal gluteal bearing) - 4 sides and corners - Posterior socket wall directly at ischeal tuberosity and buttock for WB - Ant wall higher than post to apply post direct forces
 Ischial tuberosity inside socket WB through ischium and")
Contd… Ischial containment socket: (Narrow ML) Ischial tuberosity inside socket WB through ischium and ischial ramus More stable-”bony lock” Keep femur in add In short residual limb Two types: NSNA, CATCAM

Suspension mechanism Total Suction suspension-while standing -needs pull sock or elastic bandage Partial susction Suspension: Using silicone suspension

Belt suspension

Hip disarticulation and Hemipelvectomy Canadian type prosthesis
- Slides: 86