Lower GI Conditions Dr Nishan Silva MBBS Lower
")
Lower GI Conditions Dr. Nishan Silva (MBBS)

Lower GI Bleeding

Lower GI Bleeding • A common presentation • Arises from: Small Intestine, Colon, Rectum, Anus • 3 categories Ø Occult bleeding – FBC Low Hb or +FOB Ø Moderate bleeding – PR Blood (fresh, mixed with stools or dark) Ø Acute Massive Bleeding (rare) • Large Vol. (Fresh PR) • Start and stop spontaneously • Haemodynamically unstable Shock • A Surgical Emergency! ABC’s OHCM 7 th Ed p 589

A typical scenario A 68 -year old Glaswegian man presents to A+E with a 3 day history of rectal bleeding and lower abdominal pain. On enquiry, he admits to change in bowel habit with recent episodes of constipation and weight loss over the past 3 -4 months. He has no past medical or surgical history, is a former smoker of 30 cigs/day for 26 years and does not drink alcohol.
")
Causes of Lower GI bleeding • • • Colorectal Cancer IBD (UC, Crohn’s Disease) Diverticulosis Colonic Polyp(s) Rectal Varices Haemorrhoids Anal Fissure Rectal Prolapse Infective diarrhoea Angiodysplasia Ischaemic Colitis
 Ø Colour Ø Type")
A Good History Ø Age Ø PR Blood (and Mucus) Ø Colour Ø Type of Blood Ø Quantity Ø Ø Previous episodes of PR bleeding Abdominal Pain or Tenderness Associated Anal pain +/- Defecation Altered Bowel habit Ø Stool Frequency & Consistency Ø Diarrhoea/Constipation/Both Ø Tenesmus Ø Anorexia and Weight Loss Ø Dizziness, Collapse

A Good History Ø PMHx: Gastric Ulcer, IBD, Cancer Metastases Ø Drug Hx: Aspirin, Warfarin, Steroids, Iron for IDA Ø Family Hx: Crohn’s, UC, Bowel Ca, Polyps, FAP Ø Social Hx: Alcohol intake, Smoker, Anal Intercourse Ø Systemic Enquiry: Ø Ø Mouth ulcers Eye problems Skin changes Joint pains

• Inspection – – – – Examination Breathlessness, Jaundice, Cachexia Shock? Finger clubbing Signs of Anaemia (Conjunctival pallor, Koilonychia) Mouth Ulcers, Angular Stomatitis in IDA Scars, Stomas Abdominal distension • Palpation – Abdominal Tenderness or Pain (LIF Div, RIF Crohn/Caecal Ca) – Mass felt with examining hand – Hepatomegaly Liver Mets • PR exam – – Haemorrhoids, Prolapse, Fissures or Fistulas Palpable mass per rectum (up to 7 cm) Stool colour/consistency Blood on examining finger

Investigations § § § § § FBC Ferritin & iron studies U+Es LFTs CRP Glucose Coagulation Screen Group & Save If extensive bleeding Proctoscopy/Sigmoidoscopy Colonoscopy +/- Biopsy or Barium Enema § Others: § Upper GI Endoscopy (Melaena) § Angiography (Mesenteric bleeding) § Tc 99 Red cell scan (GI Bleeding & Meckel’s))

Lower GI Bleeding • A few examples: – Colorectal Cancer – Inflammatory Bowel Disease (Ulcerative Colitis & Crohn’s disease) – Others: Diverticulosis, Haemorrhoids, Anal Fissures, Fistula in Ano. . – Sample EMQ’s

Colorectal Cancer • 3 rd commonest malignancy in UK • M: F = 3: 1 peak age 45 -70 yo • Risk Factor’s: – – – FH of Colorectal Ca, FAP, HNPCC, Prev Hx of Colon, Breast, Ovarian or Uterine Ca Prev Hx of Adenomatous Polyps Chronic UC or Colonic Crohn’s disease Western diet, Obesity, Smoking *Taken from: Oxford Handbook of Clinical Medicine 7 th Edition p 613 • Presentation depends on site: – Left-sided: Altered bowel habit (constipation & diarrhoea), PR bleeding bright red coating the stool, Tenesmus, Painful defecation? Small diameter of Left Colon Tendency towards obstruction – Right-sided: Present later. Weight loss, Right abdo pain/mass, Tendency to bleed, Blood mixed in with stools, high incidence of IDA • Emergency (40%): Obstruction, Perforation w/Peritonitis, Acute Haemorrhage

Colorectal Cancer • Investigations: – – – – FBC Microcytic hypochromic anaemia, LFTs deranged with hepatic spread + Faecal occult blood Sigmoidoscopy/Colonoscopy + biopsy Lesion (w/ 3 -5% synchronous) Barium Enema may show ‘Apple core’ appearance CT/MRI for rectal cancers, local pelvic spread and metastasis Liver US Hepatic Mets Raised Carcino-embryonic antigen (CEA) used for monitoring Taken from: www. Web. MD. com • • Taken from: http: //radiopaedia. org/images/894115 Pathology: Adenocarcinoma (95%) Character: ulcerating, stenosing, infiltrating Spread Local, mesenteric, paracolic, paraaortic nodes, Liver, Lung, Bone & Brain
 & TNM Staging (1958) Duke’s Modified")
Colorectal Cancer • Staging: Duke’s Modified Criteria (1929) & TNM Staging (1958) Duke’s Modified Criteria 5 yr survival % A Limited to mucosa 90 B 1 Involves muscularis propria 70 B 2 Penetrates through muscle, extending to serosa and bowel wall 60 C 1 Invades muscularis propria with lymph node involvement 30 C 2 Penetrates through wall into serosa with lymph node involvement 30 D Distant Metastatic Spread <10 TNM Staging T 1 – Confined to the mucosa and submucosa T 2 – Invasion of muscularis propria but no extension into serosa T 3 – Extends into serosal - no breach or local spread T 4 – Direct invasion through serosa and local structures N 0/1/2 – no nodes, 1 -3 nodes, >4 nodes M 0/1 – Metastases not present/present T 1 N 0 M 0 & T 2 N 0 M 0 = Dukes A T 3 N 0 M 0 & T 4 N 0 M 0 = Dukes B Any T with N 1 or N 2 = Dukes C & Any T&N with M 1 = Dukes D • Treatment: Surgical Resection with curative intent +/- Chemo – – – Right Hemicolectomy Caecal, Ascending, Proximal Transverse Ca Left Hemicolectomy Distal Transverse, Descending Sigmoidectomy Sigmoid Ca Anterior Resection Low sigmoid/High Rectal Ca Abdominoperineal (A-P) Resection Low Rectal Tumours <8 cm from Anal canal permanent colostomy – **Hartmann’s Carcinoma w/ Acute Obstruction (excision, colostomy, rectal stump) • Other options: Chemotherapy (5 -FU) for Duke’s B&C, RT, Palliation
")
A. Abdomino. Perineal Resection (APR)
")
A. Abdomino. Perineal Resection (APR)
")
A. Abdomino. Perineal Resection (APR)

Anterior Resection

Inflammatory Bowel Disease

Ulcerative Colitis • A relapsing and remitting inflammatory disease originating in the colonic mucosa and submucosa. • UC is limited to the colon. Begins in the rectum and can extend proximally, but rarely beyond ileocaecal junction. • M = F but 2 peaks: – i) 14 -40 years old – ii) 15% of new pts >60 years old at diagnosis • Unknown Aetiology • Associated RFs: – HLA-DR 130 association in severe UC – 60% UC pt’s + p. ANCA autoantibodies – 3 -4 times increased risk in Non-smokers and Ex-smokers – NSAIDs and stress implicated in UC flares
 (commonest): Urgency and high frequency of defecation")
Ulcerative Colitis • Presentation – Proctitis (50%) (commonest): Urgency and high frequency of defecation (4 -15/day), diarrhoea mixed with blood and mucus, rectal irritability, tenesmus. – Left-sided Colitis (30%): Rectal irritation, extensive blood & mucus in stool Bloody diarrhoea. – Pancolitis (20%): Diarrhoea, crampy, distended abdomen with systemic features: pyrexia, anorexia, weight loss, malaise and tachycardia. May involve appendix. Severe Pancolitis Backwash ileitis into terminal ileum • Extraintestinal features: A PIE SAC • Complications of UC: Perforation, Haemorrhage, Toxic Megacolon (hypotonic, grossly distended bowel > 5 cm) Colorectal Ca & death if complication sinadequately treated
 • Pyoderma")
Extraintestinal Manifestations in IBD A PIE SAC • Aphthous Ulcers (CD only) • Pyoderma Gangrenosum • I (Eye): Iritis, Uveitis, Episcleritis, Conjunctivitis (CD>UC) • Erythema Nodosum • (Primary) Sclerosing Cholangitis (p. ANCA UC>CD) / Sacroilitis • Arthritis (HLA-B 27: Ank. Spo) • Clubbing of Fingers (CD>UC) Taken from: http: //surgery. med. umich. edu/pediatric/clinical/physician_content/n-z/ulcerative_colitis. shtml

• Ulcerative Colitis Investigations: – – – FBC Low Hb due to blood loss, Raised WCC & Platelet count U+E’s hypokalaemia due to mucus loss Raised CRP & ESR Low Albumin espec. during inflammation Stool Microscopy, Culture & Sensitivity – Barium enema indicates disease extent. Chronic UC: loss of haustrations, Taken from: web 2. airmail. net/uthman/specimens/images/uc. htm rigidity & shortening of colon ‘Lead-pipe’ appearance. Excludes toxic l megacolon in severe UC. – Colonoscopy + Biopsy Inflamed, easily bleeding mucosa in rectum/distal colon. Inflammation limited to the mucosa with crypt distortion & abscess. Chronic UC Pseudopolyp formation. Taken from: www. ulcerativecolitistreatment. net Taken from: www. Radiopedia. org – http: //web 2. airma

Ulcerative Colitis • Treatment aims: Ø Induce disease remission & maintain remission and disease symptoms • Medical Therapy – Correct anaemia, hypokalaemia, hypoalbuminaemia, – Corticosteroids: Oral Prednisolone induces remission. IV Hydrocortisone used in severe flares of colitis - Long-term avoided. – Sulfasalazine or Mesalazine (5 -ASA metabolites) have anti-inflammatory effect to induce remission. Also Rectal suppositories for distal colitis – Azathioprine, 6 -mercaptopurine – immunosupression to prevent disease relapse or in cases of intolerance to steroids – Anti-TNF Infliximab good in moderate-severe UC • Surgery indicated when: – Acute colitis fails to respond to medical Tx. – Chronic Colitis persists despite treatment, unacceptable Tx SE’s, developmental delay, poor quality of life. – Toxic megacolon (within 24 hrs) – Partial or Total Colectomy with Ileostomy usually cures

Crohn’s Disease • Chronic transmural inflammatory GI Disease which is non-caseating & granulomatous in nature. Associated with recurrence in severe disease and extraintestinal manifestations. • Can affect any portion of GI tract Termimal Ileum (50%) & Proximal Colon common. Inflammation is discontinuous and separated by normal gut mucosa (‘skip lesions’). • M = F affects any age but majority of cases between 11 -35 years old • Unknown aetiology. Commonest in White Anglo-Saxon & Ashkenzai Jews • Associated Risk Factors: – CARD 15/NOD-2 mutations – Family Hx of Crohn’s or UC – Altered cell mediated immunity abnormal Th 1 activity (IL-2, IFN-γ) – x 3 -4 risk in Smokers – High sugar, low-fibre diet

Crohn’s Disease • Presentation Variable & dependent on site Ø Diarrhoea, Abdominal Pain + Tenderness (terminal ileitis), RIF mass (inflamed bowel or abscess), Perianal abscesses/ fistulae/skin tags. Ø Weight loss, malaise, fever occur in active disease. Ø Failure To Thrive in children • NB: Rectal bleeding less common in CD than UC • Extraintestinal signs: Aphthous ulcers, Uveitis, Iritis , pyoderma gangrenosum, erythema nodosum, polyarthritis, ankylosing spondylitis, sacroilitis • Complications in CD: – Full-thickness mucosal inflammation Stricture Small bowel obstruction – Abscess formation between loops of intestine – Perforation – Fistula formation: Enteroenteric, Enterocutaneous and Vesicocolic

• Investigations: – – Crohn’s Disease FBC Low Hb (Vit B 12 def. , blood loss), High WCC Raised CRP & ESR Low Albumin due to malabsorption Stool Microscopy, Culture & Sensitivity – *Taken Barium shows ‘Kantors String sign’ Taken of the terminal ileum. Also Rose-thorn from: James Enema Going -SSC in Pathology IBD Lecture Taken from: www. Learningradiology. com Flickr. com/photos/robhengxr/159283669 ulcers – Colonoscopy/Sigmoidoscopy+ Biopsy Red, oedematous thickened mucosa with deep ulcerations and erosions, separated by normal mucosa producing a cobblestone appearance. Histology shows transmural inflammation, fissuring ulcers and non-caesating granulomas

Crohn’s Disease • Management: Medical vs Surgical • Medical Mx aims to reduce inflammation & control complications. Also treat abnormal blood results eg. Anaemia – Corticosteroids (Hydrocort, Predn)– control inflammation exacerbations in moderate-severe disease – Azathioprine or Cyclosporin – immunosupression – Methotrexate – Anti-TNF Infliximab – prevent fistula formation – Metrondiazole used to treat Colonic fistulas – Nutritional therapy - elemental diet to limit antigens & reduce inflamm • Surgical Mx aims to treat complications such as strictures, bowel obstruction, sepsis, perforation or fistula formation with minimal compromise to bowel. SURGERY MAY CAUSE NEW LESIONS Ø 50 -80% patients will require surgery throughout their lives

Summary of other causes of Lower GI Bleeding Adapted from: Oxford Handbook of The Foundation Programme 2 nd Edition
 HISTORY Outpouching in • bowel wall weakest point")
DESCRIPTION • DIVERTICULAR DISEASE • (DIVERTICULOSIS) HISTORY Outpouching in • bowel wall weakest point • vasa recta meet muscular propria • Marfan, Ehlers. Danlos, • Polycystic Kidney • • • ANGIODYSPLASIA • HAEMORRHOIDS • INVESTIGATIONS & TREATMENT EXAMINATION Low fibre diet & constipation • Tenderness (LIF) +/- Peritonism Abdominal Pain (LIF) Sigmoid Colon • PR Blood or Mucus Massive painless dark red PR Bleeding • Bleeding selflimiting Irregular Bowel Habit (diarrhoea constipation) • Low Hb • Diverticulae on Colonscopy • Tx: High fibre diet • Abx in acute disease -amox/metro/cipro) • Surgical resection if persistent bleeding (recurrent diverticulitis, abscess/fistula/obstruction • Low Hb give Fe. SO 4 • FOB+ • Lesion on Colonoscopy • Consider Angiography • Tx: Arterial Embolisation, Endoscopic coagulation Haemorrhoids on Proctoscopy (co Fever/Pyrexia AVM in colonic • submucosa • Usually • proximal transverse colon Old Age Dilated& displaced vascular ‘anal cushions’ • Multiple pregancies, obese, anal sex • Straining at Stool Multiple vaginal deliveries • Painless • Fresh Blood on Toilet Paper or stools • Perianal Itch Often Asymptomatic Recurrent & brisk Fresh Blood PR • • • PR Blood or Melaena Ex may be Normal • Often not Palpable on PR unless prolapsed • Perianal tags May have rectal Prolapse Tx: High fibre diet, Anusol, Sclerosant, Band ligation or Haemorrhoidectomy

DESCRIPTION • • RECTAL PROLAPSE • ANAL FISSURE Descent of mucosa or entire rectum through anus HISTORY • “Something coming down” • ++mucus PR Weak rectal support lax • of pelvic floor and anal sphincters due to chronic straining • Elderly, postmenopausal pts, multiple vaginal deliveries • • INVESTIGATIONS • Prolapse may be demonstrated on straining in clinic • Prolapse may be ulcerated & bleeding Repeated defecation (mucosal) or Incontinence (full) Sigmoidoscopy mucosal inflamm Defecating proctogram if uncl diagnosis • Med. Mx: Stool softeners for constipation • Surg. Mx: Rectoplex fix rectum to sacrum • Children constipation, CF, whooping cough • Anal tear posteriorly • May be associated with Crohn’s or Cancer Posterior/Anterior tear at anal margin • • Severe knife-like pain • on defecation Sigmoidoscopy if Colorectal Ca • Deep throbbing pain • Tx: High fibre diet Previous Pregnancy • Hx Constipation, Straining ++ Associated: Perianal tags, ulcers, fistulae • 5% lignocaine therapy • Botox injection • • Sphincerotomy Surgery Fistulotomy or • Staged sphincter repair • • ANAL FISTULAS Usually small vol. bright red bleed EXAMINATION PR Tenderness PR blood on examining finger Abnormal epithelial connection seen between anus and skin All ages • Pain • Infection commonest • • IBD (CD>UC) Bloody or Purulent anal discharge • Anal itching • Systemic symptoms if infected abscess Trauma: episiotomy, prostatectomy, anal sex • Fresh Blood on Toilet • paper • • • Erythema

 veins located in the wall of the")
Hemorrhoids • Hemorrhoids are dilated, twisted (varicose) veins located in the wall of the rectum and anus.

• Hemorrhoids occur when the veins in the rectum or anus become enlarged; they may eventually bleed. • Hemorrhoids may also become inflamed or may develop a blood clot (thrombus).
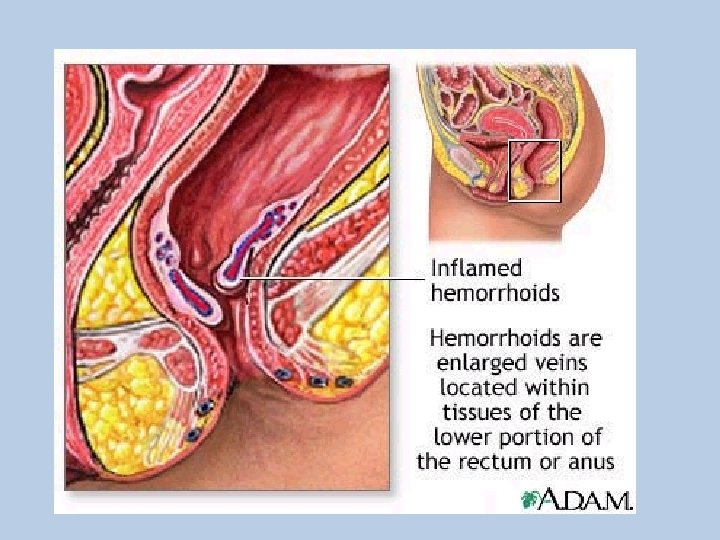

Etiology • • • Most common cause - constipation Prolonged straining Pregnancy Heredity Increased intra-abdominal pressure Aging (due to thinning of supportive tissue)

Internal / External Hemorrhoid

Classification of Internal Hemorrhoids • Grade I – Seen on anoscopy, may bulge a short way into anal canal; does not extend below dentate line • Grade II – Prolapses out of anal canal with straining or defecation; reduces spontaneously • Grade III – Prolapses out of anal canal with straining or defecation; reduces manually • Grade IV – Irreducible; may strangulate

Prolapsed Hemorrhoid

Diagnosis • The diagnosis of internal or external hemorrhoids is made by – inspection – digital exam – direct vision through the anoscope & proctosocpe

Treatment • Treatment includes medical as well as surgical modalities • With medical therapy, bleeding and pain usually improve over a 6 week period

Medical Therapy • Stool bulking agent – Psyllium – Methylcellulose • Sitz baths – probably most effective topical treatment for relief of symptoms

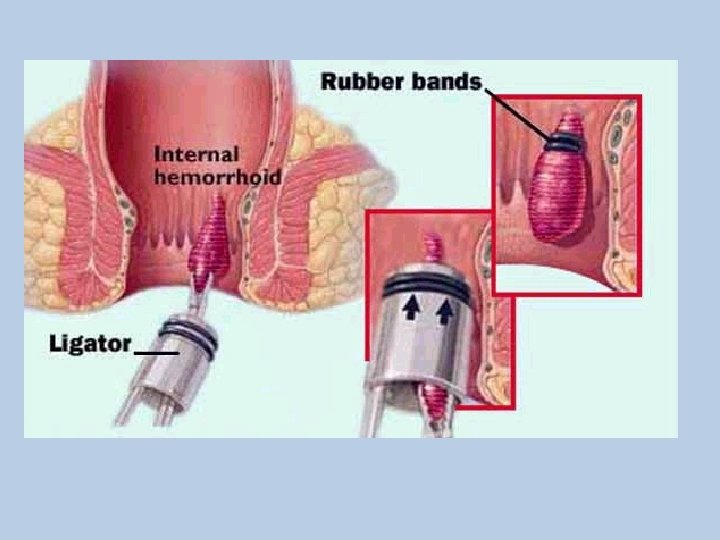
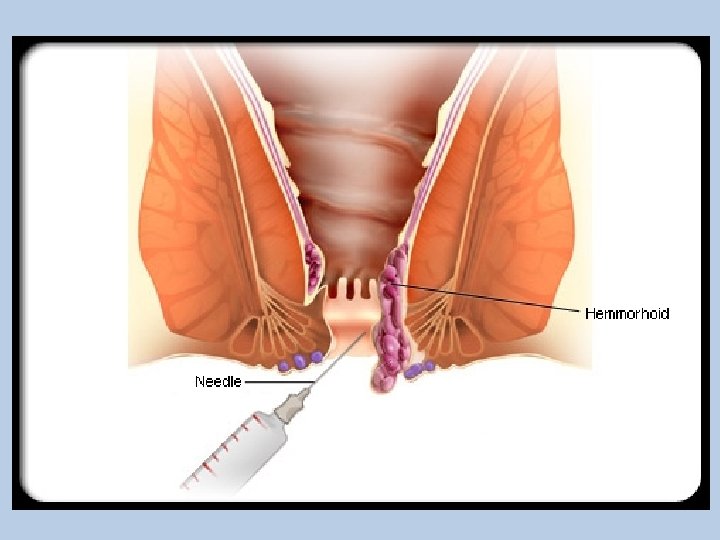
Surgical Therapy • Rubber Band Ligation – One of most widely used techniques – Approximately 5 -7 days after procedure the banded tissue sloughs-off • Infrared Photocoagulation – Laser not often used • Sclerotherapy – Phenol 5% – Sodium tetradecyl sulfate

Anal Fissure

Anal Fissure and Sphincterotomy

Anal Fistula – Fistula in ano

Fistula Types - Fistulectomy

Peri. Anal Abscess

Pilonidal Disease • Pilonidal disease is an infection caused by a hair that injures the skin at the top of the cleft between the buttocks. • A pilonidal abscess is a collection of pus at the infection site; a pilonidal sinus is a chronic draining wound at the site.


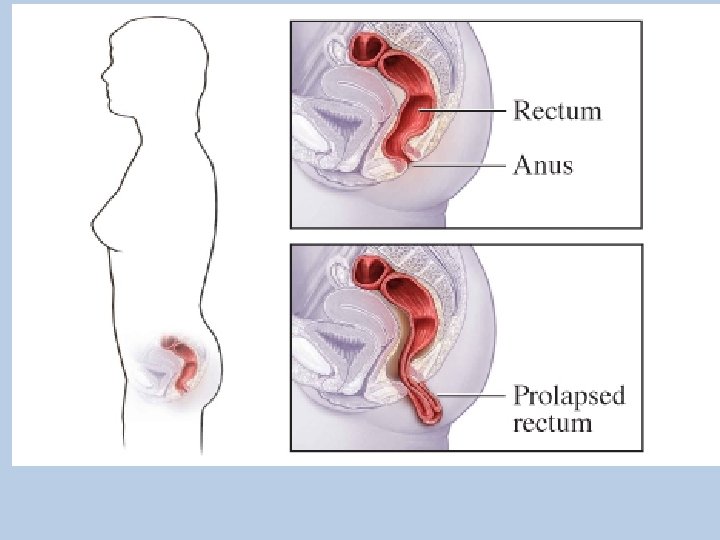
Rectal Prolapse • Rectal prolapse causes the rectum to turn inside out, so that the rectal lining is visible as a dark red, moist fingerlike projection from the anus. • Less commonly, the rectum protrudes into the vagina


Foreign Objects

Surgeries and Other Procedures

Bowel anastamosis

Colostomy

Illeostomy

Illeostomy

Illeostomy

Abdomino-perineal resection

Whipples procedure

Special considerations should be made in • Bowel anastamosis – 3 -4 days of fasting • Colostomy – Reduce fibre, Reduce gas • Illeostomy – Increase fibre • Bowel handling – Nil by mouth till bowel sounds

Sigmoidoscopy / colonoscopy • Low fibre for 3 days • Clear liquids for one day • Energy liquids • Laxatives
 A 30 yo male with bloody diarrhoea 20 times/day,")
MEQ’s Rectal Bleeding • 1) A 30 yo male with bloody diarrhoea 20 times/day, weight loss and colonoscopy showing inflammation from the rectum to caecum • • • (a) (b) (d) (e) (f) (g) (h) (i) (j) Colon Ca Crohn’s Disease Fissure in ano Fistula in ano Gastroenteritis Haemorrhoids Rectal proplase Diverticulosis Ulcerative colitis
 A 30 yo male with bloody diarrhoea 20 times/day,")
MEQ’s Rectal Bleeding • 1) A 30 yo male with bloody diarrhoea 20 times/day, weight loss and colonoscopy showing inflammation from the rectum to caecum • • • (a) (b) (d) (e) (f) (g) (h) (i) (j) Colon Ca Crohn’s Disease Fissure in ano Fistula in ano Gastroenteritis Haemorrhoids Rectal proplase Diverticulosis Ulcerative colitis
 A 25 yo woman, 6 weeks post-partum with PR")
MEQ’s Rectal Bleeding • 2) A 25 yo woman, 6 weeks post-partum with PR bleeding, puritis and perianal pain • • • (a) (b) (d) (e) (f) (g) (h) (i) (j) Colon Ca Crohn’s Disease Fissure in ano Fistula in ano Gastroenteritis Haemorrhoids Rectal proplase Diverticulosis Ulcerative colitis
 A 25 yo woman, 6 weeks post-partum with PR")
MEQ’s Rectal Bleeding • 2) A 25 yo woman, 6 weeks post-partum with PR bleeding, puritis and perianal pain • • • (a) (b) (d) (e) (f) (g) (h) (i) (j) Colon Ca Crohn’s Disease Fissure in ano Fistula in ano Gastroenteritis Haemorrhoids Rectal proplase Diverticulosis Ulcerative colitis
 A 21 yo lady with rectal bleeding and severe")
MEQ’s Rectal Bleeding • 3) A 21 yo lady with rectal bleeding and severe pain on defecation • • • (a) (b) (d) (e) (f) (g) (h) (i) (j) Colon Ca Crohn’s Disease Fissure in ano Fistula in ano Gastroenteritis Haemorrhoids Rectal proplase Diverticulosis Ulcerative colitis
 A 21 yo lady with rectal bleeding and severe")
MEQ’s Rectal Bleeding • 3) A 21 yo lady with rectal bleeding and severe pain on defecation • • • (a) (b) (d) (e) (f) (g) (h) (i) (j) Colon Ca Crohn’s Disease Fissure in ano Fistula in ano Gastroenteritis Haemorrhoids Rectal proplase Diverticulosis Ulcerative colitis
 A 90 yo woman with PR bleeding and something")
MEQ’s Rectal Bleeding • 4) A 90 yo woman with PR bleeding and something coming down every time she defecates • • • (a) (b) (d) (e) (f) (g) (h) (i) (j) Colon Ca Crohn’s Disease Fissure in ano Fistula in ano Gastroenteritis Haemorrhoids Rectal proplase Diverticulosis Ulcerative colitis
 A 90 yo woman with PR bleeding and something")
MEQ’s Rectal Bleeding • 4) A 90 yo woman with PR bleeding and something coming down every time she defecates • • • (a) (b) (d) (e) (f) (g) (h) (i) (j) Colon Ca Crohn’s Disease Fissure in ano Fistula in ano Gastroenteritis Haemorrhoids Rectal proplase Diverticulosis Ulcerative colitis
 A 26 yo man presents with chronic bloody diarrhoea")
MEQ’s Rectal Bleeding • 5) A 26 yo man presents with chronic bloody diarrhoea and RIF pain. He has lost weight recently and feels generally unwell and pyrexial. He is also complaining of joint pains and barium enema shows altered mucosal pattern with deep-fissured ulcers. • • • (a) (b) (d) (e) (f) (g) (h) (i) (j) Colon Ca Crohn’s Disease Fissure in ano Fistula in ano Gastroenteritis Haemorrhoids Rectal proplase Diverticulosis Ulcerative colitis
 A 26 yo man presents with chronic bloody diarrhoea")
MEQ’s Rectal Bleeding • 5) A 26 yo man presents with chronic bloody diarrhoea and RIF pain. He has lost weight recently and feels generally unwell and pyrexial. He is also complaining of joint pains and barium enema shows altered mucosal pattern with deep-fissured ulcers. • • • (a) (b) (d) (e) (f) (g) (h) (i) (j) Colon Ca Crohn’s Disease Fissure in ano Fistula in ano Gastroenteritis Haemorrhoids Rectal proplase Diverticulosis Ulcerative colitis
 A 32 yo woman presents with rectal bleeding, which")
MEQ’s Rectal Bleeding • 6) A 32 yo woman presents with rectal bleeding, which occurs post-defecation. The bleeding is bright red and painless. Endoscopy is normal. • • • (a) (b) (d) (e) (f) (g) (h) (i) (j) Colon Ca Crohn’s Disease Fissure in ano Fistula in ano Gastroenteritis Haemorrhoids Rectal proplase Diverticulosis Ulcerative colitis
 A 32 yo woman presents with rectal bleeding, which")
MEQ’s Rectal Bleeding • 6) A 32 yo woman presents with rectal bleeding, which occurs post-defecation. The bleeding is bright red and painless. Endoscopy is normal. • • • (a) (b) (d) (e) (f) (g) (h) (i) (j) Colon Ca Crohn’s Disease Fissure in ano Fistula in ano Gastroenteritis Haemorrhoids Rectal proplase Diverticulosis Ulcerative colitis

- Slides: 79