Lower GI bleed Dr Shrish Bhatnagar Dedication SGPGIMS

Lower GI bleed Dr Shrish Bhatnagar

Dedication SGPGIMS JNMC Late Dr S K BHATNAGAR

Classification • Anatomical – upper & lower - by ligament of Trietz • Practical – Upper - UGIE accessible Mid - Accessible by Capsule endoscopy or Enteroscopy Lower - Colonoscopy accessible

LGIB= bleed below lig. of treitz

Etiology
 -Origin most commonly from the")
Clinical presentation • Hematochezia (bright red blood per rectum) -Origin most commonly from the colon. -Less reliable in infants - shorter intestinal transit time -Massive UGI bleeding may present with hematochezia • Melena (black, tarry, and foul-smelling stools) -Source - above the ileocecal valve -Also in bleeding from the proximal large bowel with slow colonic transit time • Occult Gastrointestinal Bleeding -pallor or fatigue -iron deficiency anemia • Symptoms Of Severe Blood Loss -malaise, tachycardia, or even profound shock without any objective sign of bleeding

Classification by the amount of bleed • • • Large vol. bleeds Meckel’s diverticulum Duplication cysts AV malformations IBD Moderate vol. bleeds Intussusception Small vol. bleeds • With colitis IBD CMPA Infectious enterocolitis • Without colitis Polyp SRUS Anal fissure
 Cause N (%) Colitis 27 (42%) Colorectal")
Lower GI bleed in children (India, n=64) Cause N (%) Colitis 27 (42%) Colorectal polyp 26 (41%) Solitary rectal ulcer 3 (5%) Enteric fever 3(5%) PHTN colopathy 2 (3%) Colonic AV malformation 1 (1. 5%) Internal hemarrhoid 1 (1. 5%) Undiagnosed 1 (1. 5%) Yachha SK et al. J Gastroenterol Hepatol 1996; 11(10): 903 -7.

Management • Resuscitation • Approach to diagnosis – Localisation of bleed • Therapy

Resuscitation The hemodynamic stabilization of a bleeding child involves 1. Assessing the degree of hemodynamic compromise 2. Establishing a venous access 3. Treatment of shock – fluids and drugs 4. Arresting further bleed

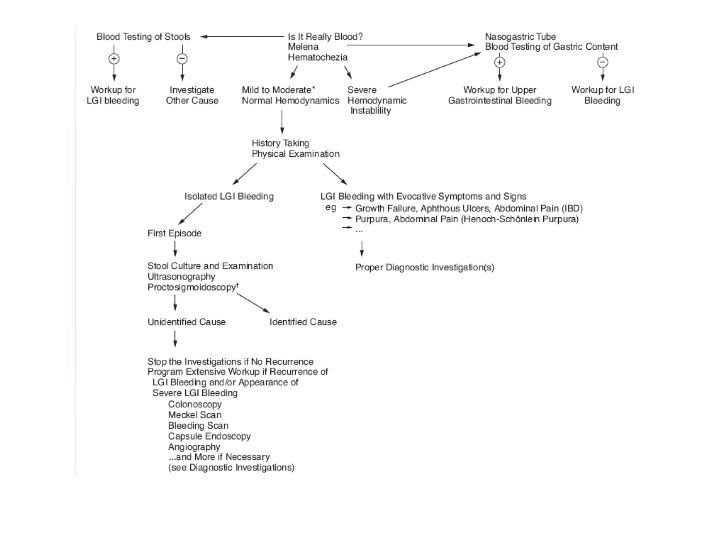
Approach • IS IT BLOOD ? - food or medicine • IS IT BLOOD FROM THE CHILD ? - maternal blood at delivery - fissured nipple during breastfeeding - munchausen syndrome by proxy

Contd. . • IS IT BLOOD FROM THE GI TRACT ? - swallowed blood *post adenoidectomy *post tonsillectomy *epistaxis *trauma to nasopharynx - hematuria - menstrual bleed

Contd. . • IS IT BLOOD FROM LOWER GI TRACT ? - gastric aspirate - hyperactive bowel sound - UGIE - BUN/s. creatinine

Exclusion of an UGI Source of bleeding • Nasogastric lavage containing , - gross blood, - 25% blood-tinged fluid, or - strongly guaiac positive dark fluid • Sensitivity 80% , PPV 93% and NPV 99%. • The presence of bile increases the sensitivity Luk GD et al. JAMA 1979; 241: 576– 8.

Exclusion of an UGI Source of bleeding • Ratio of blood urea nitrogen to creatinine -A high ratio of blood urea nitrogen to creatinine would be in favor of upper gastrointestinal bleeding. The urea nitrogen increases following gastrointestinal bleeding because of an increased absorption of blood protein from the small intestine or a decreased renal excretion of urea nitrogen due to hypovolemic state. Pediatr Gastroenterol Hepatol Nutr. 2015 Mar; 18(1): 30– 38. . • Ratio ≥ 30, has sensitivity 68. 8% & specificity 98% for UGIB. Urashima M et al. J Pediatr Gastroenterol Nutr 1992; 15: 89– 92 • Esophagogastroduodenoscopy - gold standard

Identifying cause and Localization History • Age at onset • Characteristics of blood in stool • Associated symptoms - constipation/diarrhea - Presence of abdominal or anorectal pain - Presence of colitis features • H/o travel/recent use of antibiotic / contaminated food • Family history • Dietary h/o Cow milk or soy protein • Rule out a hematological cause

Characteristics of bleed • Hematochezia limited to the outside of the stools or spots of red blood coating the stools or found in the diaper • Hematochezia mixed through the stool - colonic source for the bleeding located • Hematochezia mixed with mucus and loose stools suggests colitis Rectal bleed Bleed Above Rectum

Characteristics of bleed • Maroon-colored stools distal small bowel • Currant jelly stools ischemic bowel lesions (intussusception or midgut volvulus) • Malena – UGI bleed usually but from anywhere upto right colon

Correlation of amount, color, pain and stool characteristics Walker Ped. Gastrointestinal Disease 4 th ed, 2004

Pointers in history • • • H/o petechiae, ecchymosis, epistaxis - Hematological disorder Recent antibiotic administration - Pseudo membranous colitis An infant on cow’s milk with colitis - Cows milk protein allergy Passage of painless, large volume, maroon blood requiring blood transfusions -Meckels or intestinal duplication Mass prolapsing per rectum with bleeding - Polyp /prolapse rectum /intussusceptum Recurrent abdominal pain, diarrhea, loss of weight, pedal edema, fever - IBD

Abdominal and rectal examination • Hepatosplenomegaly, ascites, dilated veins Portal hypertension • Abdominal mass - Intussusception, IBD, intestinal duplication • Anal fissure - Constipation, Crohn disease • Skin tag, fistula, abscess -Crohn disease, immunodeficiency syndromes • Hemorrhoids, rectal varicosities - Portal hypertension, constipation (adolescent) • Rectal mass at digital rectal examination Polyp, intussusceptum

Physical Skin markers • Purpura - Henoch-Schönlein purpura, hemorrhagic disease, hemolytic uremic syndrome • Jaundice, palmar erythema, spider angioma Liver cirrhosis • Café au lait spots - Turcot syndrome • Pigmentation of the lips, buccal mucosa, face Peutz-Jeghers syndrome • Iritis & Arthritis – IBD • Short stature, webbed neck, widespread nipples – Turner syndrome

Diagnostic investigations • • Laboratory invx Radiography USG abd Proctosigmoidoscopy & Colonoscopy Enteroscopy /capsule endoscopy Radionuclide scanning Angiography Intraoperative endoscopy

Laboratory investigations • Complete blood count, clotting studies -Eosinophilia in allergy/parasitic infections -Chronic iron defeciency anemia due to chronic blood loss • Stool microscopy for pus cells and trophozoites of E. histolytica • Stool culture in infectious colitis • C. difficle toxin in pseudomembranous colitis • LFT in liver disease & PHTN

Radiography • History & physical exam s/o obstructive or ischemic process – plain erect film abdomen • To look for – - air fluid level - dilated loops of bowel - pneumoperitoneum • Ba enema – no role

Ultrasound • In acute emergency setting when acute obstruction /ischemia is suspected. • Abdominal mass • Intussusception , volvulus, duplication cyst etc.

Proctosigmoidoscopy/colonosc opy • Diagnostic & therapeutic advantage • Most LGI bleed self-limiting and colonoscopy done as a elective procedure
 Cause % Juvenile polyp 69. 4% Ulcerative colitis")
Colonoscopic finding in LGI bleed (n=72) Cause % Juvenile polyp 69. 4% Ulcerative colitis 5. 5% Acute colitis 4. 2% Tuberculosis 2. 7% Allergic 1. 3% Amoebic 1. 3% Thapa BR et al. Indian Pediatr 1991; 28: 383 -9.
 Juvenile polyps (n= 219) Juvenile polyposis (n=")
Colonic polyps in Indian children (n= 236) Juvenile polyps (n= 219) Juvenile polyposis (n= 17) p Value Age (yrs) 5. 97 ± 2. 62 7. 68 ± 2. 95 <0. 05 Gender (M: F) 3. 5 : 1 3. 2 : 1 NS Duration of symptoms (months) 12. 24 ± 13. 15 33. 0 ± 27. 0 <0. 001 Rectal bleeding 99% 94% NS Polyp localised to rectosigmoid 90% 0% <0. 001 Adenomatous changes 5% 59% <0. 001 Polypectomy (session/child ) 1. 04 ± 0. 20 4. 76 ± 3. 72 <0. 001 Poddar U et al. Am J Gastroenterol 1998 Apr; 93(4): 619 -22.

Polyps • Juvenile polyps - most common colonic polyps in children • A significant number of cases of polyps are multiple and proximally located, which emphasizes the need for total colonoscopy in all • Juvenile polyps should be removed even if asymptomatic because of their neoplastic potential. • Surveillance colonoscopy is required in juvenile polyposis only. Poddar U et al. Am J Gastroenterol 1998 Apr; 93(4): 619 -22.

Solitary Rectal Ulcer Syndrome • SRUS benign rectal disorder often related to abnormal defecation or straining • Constipation, rectal bleeding, passage of mucus, H/O manual evacuation • Endoscopy • Histological is necessary fibrous obliteration of the lamina propria • Difficult to Treat condition

Meckel's diverticulum • A true intestinal diverticulum that results from the failure of the vitelline duct to obliterate, 50% cases have ectopic gastric mucosa which bleeds • Most common cause for painless major lower gastrointestinal bleeding in children aged less than 2 years • Treatment : Surgical Resection

Meckel’s scan • 99 m. Tc-pertechnetate - Uptake is by mucus secreting cells • Time - Activity in the ectopic gastric mucosa at the same time as activity in the normal gastric mucosa, although a small Meckel’s diverticulum may seem to appear later • Location - May appear anywhere within the abdomen but most frequently seen in the right lower quadrant • Ranitidine suppresses the gastric mucosal secretion and minimises the enhancement of D 2 which occupies a similar area as the Meckel’s diverticulum and thereby improves the sensitivity of the scan

Meckel’s scan

Meckel’s scan • Meckel’s Scan - Specificity of 95% but sensitivity only 85% • Even though Superior mesentric artery angiography and 99 m. Tc-labeled red blood cell scan are alternatives, in the event of a negative Meckel’s scan and a highsuspicion of Meckel’s bleed, laparotomy is done. Sfakianakis GN et al. AJR 1982; 138: 7– 12. Kong MS et al. J Formos Med Assoc. 1993; 92: 717– 720.

Duplication cysts • Most common in the ileum. Gastric duplications least common. • Except for duodenal duplications, they occur on the mesenteric side. • An intra-abdominal mass may be appreciated in a child either by abdominal palpation or on rectal examination • Small bowel duplications often(30%) contain gastric mucosa and may be diagnosed by 99 m. Tc radioisotopic imaging Wyllie R, Hyams JS, Pediatric Gastrointestinal Disease. Pathophysiology, Diagnosis, Management, 2 nd ed. Philadelphia: WB Saunders 1999: 505.

Duplication cyst

Tc 99 m-labelled. RBC Scan • May detect bleeding at a rate as low as 0. 1 to 0. 5 m. L/minute • Advantages (1) sensitive to low rates of bleeding (2) safe (3) noninvasive (4) no risk of contrast reactions (5) low in cost • Disadvantages (1) Lack of therapeutic capability (2) Doubt about its accuracy. • The sensitivity of the test can be decreased by bowel motility stimulated by intraluminal blood. Howarth DM et al. Nucl Med Commun 2002; 23: 591 -4.

Angiography • Less sensitive than radionuclide scanning with the ability to detect bleeding of more than 0. 5 ml/min • Bleeding detection rates - 20% to 70%. • Sensitivity depends - severity of bleeding at the time of angiography - intermittent bleeding, procedural delays - venous or small vessel bleeding. • Diagnostic and therapeutic role - pharmacologic vasoconstriction - selective microembolization
 • 18 pts with lower intestinal bleeding (LIB)")
Vascular malformations of the colon (VMC) • 18 pts with lower intestinal bleeding (LIB) and VMC • Age of clinical onset-1 week to 16 years • Duration of LIB before diagnosis -1 month to 9 years. • Scintigraphy, colonoscopy, and barium enema results were normal or suggested a vascular problem • Mesenteric arteriography detected VMC in all 18 cases • Left hemicolon and rectum were affected in 83% of the cases De la Torre L et al. J Pediatr Surg. 2002 Dec; 37(12): 1754 -7.

Capsule Endoscopy • Noninvasive mode of examining the small intestine • “Diagnostic yield” is greater for capsule endoscopy than for enteroscopy and ranges from 40% to 90% • Colonic sources of bleeding are difficult to evaluate via capsule endoscopy because of retained stool, limited battery life, and poor field of vision due to the colon’s large diameter Pennazio et al. Gastroenterology 2004; 126: 643– 53. Rastogi A et al. Gastrointest Endosc 2004; 60: 959– 64.

Diagnostic yield of capsule endoscopy • 44 consecutive CEs in 43 pt, were evaluated retrospectively. • Indication for CE *obscure GIB - 40 pts *iron def. anemia - 1 pt *rt lower quadrant abd. pain - 2 pts • Overall diagnostic yield was 42% (18/43 pts) Rastogi A et al. Gastrointest Endosc 2004; 60: 959 -64.

Contd. . • Result – Diagnostic finding No. of pt Angiodysplasia 13 Intestinal ulcers 2 Crohn disease 2 Mass lesion 1 Rastogi A et al. Gastrointest Endosc 2004; 60: 959 -64

Summary • Lower GI Bleed common causes are different from adults • Polyp, SRUS, Colitis(Infective/Inflammatory/ Allergic) are main causes of LGI Bleed in children • Detailed history and meticulous examination gives lead in many cases of LGI Bleed • Endoscopy and Colonoscopy are the mainstay for initial diagnostic testing.

Thanks….
- Slides: 46