LOW VISION Rehabilitation Case reports LOW VISION EXAM

LOW VISION Rehabilitation Case reports

LOW VISION EXAM v History, Chief complaints, ADL, Goals v Education to patient about their eye condition v LV refraction in trial frame v Lighting a. filters b. contrast c. glare v Magnification v a person with low vision is one who has an impairment of visual functioning

MAGNIFICATION Relative Size v The object is manipulated to gain the magnification v The actual size of the object is increased thereby increasing the retinal image v In most cases this is a simple type of magnification, copier enlargement

MAGNIFICATION Angular Magnification v Uses two or more lenses in a system to create magnification v Effective when the object it too far away to move closer or when it is too big to make larger v Ocular lens goes closest to the eye, objective lens is closest to the object. Usually a telescopic system v Other lenses or prisms may be found between the lenses
 v Magnifiers ( hand held,")
MAGNIFICATION Relative –distance v Microscope (reading glasses, bifocal, loupe) v Magnifiers ( hand held, stand, dome, ) v Magnification that uses relative distance, tends to bring the image closer to the eye and that is relative distance

MAGNIFICATION Electronic v Also referred to as projection magnification v It is the enlargement of an object by projecting it onto a screen v Works the same way as relative size mag but with the use of technology v This results in an electronic size increase of the object with out as much loss of field of view

 v Dx: Born with congenital glaucoma,")
LOW VISION EXAM v 48 yo WM (RK) v Dx: Born with congenital glaucoma, s/p corneal transplant/ senile nuclear sclerosis, degenerative retinal drusen v Goals: Works with patients of his own and would like to ‘see’ them better while talking to them in his new office

LOW VISION EXAM v Entering Visual acuities with out glasses OD: 20/100 -2 near: 4 pt (J 1) @ 1 ½ inch OS: 20/200 near: 3 pt ( J 1+)@ 1 inch v Low vision refraction: OD: -4. 00 -1. 00 x 025 20/60 OS: -2. 00 -1. 00 x 180 20/200

RECOMMENDATION v Stella floor lamp for his office for better illumination, his office did not have any windows or natural light v Walters 4 x 12 telescope, for distance spot reading for taking the bus VA 20/25 - h/o using a Bioptic but did not want one v New glasses for in his office- for help with identifying faces

LIGHTING v Stella lamp • 10 point level dimming • Trispectrum technology cool light warm light bright light- similar to “natural light” • Flexible arm- to control glare

LIGHTING v Uno day light lamp v 3 point touch v Natural day lite v Light weight

TELESCOPES v Telescopes are an afocal optical systems consisting of two lenses, separated in space, in air. There are two types of telescopic systems, Keplerian and Galilean. v The optical principles of the two telescopes are visually identical. v An enlarged retinal image falls over a larger area of photoreceptor cells, providing the patient with additional information and better acuity
 objective")
TELESCOPES v Keplerian telescopes have a v Galilean telescopes have a weak (+) objective lens and a strong (+) eyepiece lens. (-) eyepiece lens. v form an inverted image so they v form an erect/upright image. require an erecting lens or prism v Galilean telescopes have several v 4 x or stronger, and give an practical advantages for low vision optically superior image, but are work. Typically they are 2 x, 3 x or 4 x more expensive with a smaller exit in strength, inexpensive, light, and pupil requiring better centering and have a large exit pupil, which makes aiming. centering less difficult.
 v Dx : wet ARMD")
L. V REFRACTION v 90 yo F ( FH) v Dx : wet ARMD c h/o injections v Taking care of her husband with dementia v Goals include; wants stronger reading glasses, difficult for her to read small print labels v Already has strong reading glasses OD: +4. 00 -0. 75 x 087 OS: +4. 50

L. V REFRACTION v Entering Visual acuities with current distance glasses OD: +0. 25 -1. 50 x 110 20/100+ OS: -2. 00 5/125 -3 ADD: +3. 50 Near: 32 pt @ 30 cm OU v LV refraction: OD: -1. 75 -0. 75 x 110 20/50 OS: -1. 00 -1. 50 x 105 5/125 ADD: +3. 00 32 pt @ 30 OU v Stella lamp/ dome: read newsprint comfortably, thrilled with increased DVA and reading VA
 v Dx: h/o strabismus OD,")
L. V REFRACTION v 80 yo W M (RH) v Dx: h/o strabismus OD, dry ARMD OS, wet ARMD OD h/o injections OD and cataract removed OS- which decreased the vision. v Goals: reading choir music in Church, reading newsprint, dials on TV remote

L. V REFRACTION v Entering Visual acuities with current specs OD: -0. 25 -2. 50 x 014 20/60 -2 OS: -1. 00 -0. 75 x 085 20/250 ADD: +2. 75 Near: 16 pt @ 30 cm OU v LV refraction: OD: +0. 50 -1. 00 x 135 20/50 OS: +0. 25 -0. 50 x 085 20/225 ADD: +3. 00 14 pt @ 30 cm OU v New specs for choir, typoscope/ large print checks/Stella lamp for increased illumination/ large TV remote ( with large buttons)
 v dx: + dry ARMD")
L. V. REFRACTION v 86 yo WM (R. S) v dx: + dry ARMD OU, + Fuchs corneal dystrophy OS v c/o just bought new specs and now seeing double with them. v Can not drive with one image above the other.

L. V REFRACTION v Entering VA with new specs: OD: +0. 25 -1. 75 x 125 20/20 OS: +2. 00 -2. 50 x 080 20/30 -1 Add: +3. 00 5 pt @ 35 cm v Von Graffe: OD: 1^ BD OS: 1^ BO v Trial frame: 3^ base up OS v Called to say thank you, he can drive now

DIPLOPIA v Warning about prisms – visual acuity will be slightly blurry with a large amount of prism, however vision may actually appear clearer due to the loss of diplopia v prism doesn’t always work- when it does, so happy v can take up to several months for the eyes to adjust

L. V. REFRACTION v 65 yo W F , worked as an accountant (K. W) v Dx; acute retinal necrosis 2/2 viral infection. v Can be due to VZV, HSV I, or II , or CMV v h/o meningitis- RD OU, and 5 hours of surgery in the hospital v Using +4. 50 OTC OU specs used to help with TV and walking around. Now, not helpful v h/o cataract extraction 10+ years ago

ARN v General pathology v There appear to be two distinct disease phases: v Acute Herpetic Phase: episcleritis or scleritis, anterior (usually granulomatous) uveitis, vitreous opacification, and inflammation of the retina, retinal arteries, and choroidal vasculature. Optic neuropathy can also occur. v Late Cicatricial Phase: Retinal holes and tears occur at the junction of normal and atrophic retina, leading to retinal detachment in 50 -75% of untreated eyes. Subsequent proliferative vitreoretinopathy with fibrosis and traction on the retina also contribute to retinal detachment. Multiple retinal holes with the appearance of a sieve are typical. Most retinal breaks occur in the necrotic retina and the junction between normal and necrotic retina.

ARN v Entering VA with her glasses: OD: 5 “/125 OS: HM v LV refraction: OD: +8. 50 -2. 00 x 180 20/500 OS: HM ADD: +3. 00 63 pt print at 30 cm v CCTV


GLARE CONTROL v RED/Orange: corning lens/ NOIR for R/C dystrophies or achromatopsia v AMBER: macula dystrophies or disturbances v YELLOW: increased contrast in nighttime driving. useful early ARMD * v GREEN: usually chosen by glaucoma patients* v BLUE: usually stroke related vision loss (blue/ yellow on CCTV) v FL-41/PLUM: for glare and migraine control v GRAY: over all good tint
 v Dx with mild oculotanous albinism")
GLARE / FILTER v 18 yo WM (AR) v Dx with mild oculotanous albinism v Difficulty with glare while driving, new driver v Hard to read his sheet music while in choir: black notes on white paper

GLARE v Entering acuities: • OD: 20/30 • OS: 20/20 v Refraction: • OD: -0. 50 20/20 • OS: -0. 25 20/20 v A/R coating and blue blocking Crizal/ prevencia for indoor glare v Polarized amber fit overs for driving v Fl-41 specs for choir cut the glare from overhead lighting to see his sheet music more comfortably
 v Dx: congenital nystagmus, and (2014)")
GLARE/ FILTERS v 61 yo WM ( LA) v Dx: congenital nystagmus, and (2014) cataracts. v Goals: gets lost in grocery stores can not read labels v A LOT of glare issues currently wearing yellow tinted specs v Can not see his phone, wants to learn about features on his i. Phone

FILTERS v Entering VA with out glasses: OD: 20/350 OS: 20/350 Near VA: 80 pt @ 20 cms v Refraction: OD: +4. 00 -1. 75 x 165 20/300 OS: +4. 00 -1. 75 x 175 20/300 ADD: +2. 50 20 pt @ 35 cm v +6. 00 OTC reader- 20 pt @ 35 cm

RECOMMENDATIONS v 6 x ill stand c posture desk for reading v. Referred to our OT for i. Phone training v. Tried every single filter and he loved the v U 26 30% Blue

ECCENTRIC VIEW v 77 yo WM v + dry ARMD for 20 years. Just now having problems with near work. Really enjoys doing art, he has taught, and like to do wood carving. He is still driving during the day v VA according to his record OD: 20/400 OS: 20/25 v VA with EV: OD: 20/ 80 Down OS: 20/25 v So happy * 3. 5 x ill hand held* fine print, menus etc.

RUBY v 28 yo AAM v Dx: optic atophy 2^ to MS, vision loss began 2 years ago v Goals: he wants to live independently, read his own mail, bills, cook for him self.

HAND HELD TECH v Visual acuity : OD: 20/225 OS: 3/125+ Near: 40 pt @ 25 cm v Refraction NI at all, auto refractor indicated a low myopic v Demonstrated hand held, stands, v Did best with electronics- RUBY HD hand held electronic magnifier v refer to Erin/ OT for help with Low vision aides v Orientation and mobility training.


HOMONYMOUS HEMIANOPSIA v 48 yo M v h/o stroke on left side. Loss of right side vision. Things disappear and he runs into people, bumps his head doesn’t like to go places at night. In other words he does not have neglect. “neglect” is an official diagnosis. v LV refraction: OD: +0. 50 -0. 25 x 120 20/20 OS: +0. 50 -0. 25 x 060 20/20

FRESNEL PRISM v Started with 30^ yolked base right fresnel prism on the inside of his glasses lined up with the outer limbus. v Next referred to our Erin/ OT for training v Very happy with outcome v NO DRIVING

CHORIORETINITIS SCLOPETARIA v Definition: chorioretinitis sclopetaria- proliferation of fibrous tissue in the choroid and retina as the result of contusion of the sclera by a high velocity missile to the orbit. v The term sclopetaria may originate from the old English word “sclow” which means to claw or tear, or from the Latin word “sclopetum” which was a Roman gun. When a high-velocity projectile such as a BB passes adjacent to the globe, there are direct and indirect shock wave forces which can lead to simultaneous retraction of the choroid and retina leaving an area of bare sclera at the site of the break. Immediately after the injury, there is usually extensive intraocular hemorrhage, with subretinal, intraretinal, and vitreous hemorrhage, with large overlying retinal breaks. The hemorrhage resorbs and organizes, leaving extensive fibrous proliferation that seems to fuse the retina and the choroid. The lesion has irregular borders, sometimes with a claw-like configuration. Due to significant post-traumatic fibrovascular proliferation and scar formation, there is very low risk of retinal detachment after injury (1).

K. M. v 28 yo M v Dx: 6 GSW to the head and 11 to the body v Fractured orbital bones and subsequent reconstruction of face v c/o diplopia, blur at distance and inability to read his mail or any forms v Seems like his eyes don’t feel like they are side to side and don’t work well together. He sees a second image over the first one

K. M. v Entering VA s rx: OD: 20/150 OS : 20/500 Near: 16 pt @ 30 cm v Refraction: OD: -0. 75 x 165 20/40 2^ BD OS: -0. 50 -2. 50 x 005 20/60 3^ BI ADD: +1. 75 he could read standard print with good lighting.



J. S. v 60 yo WM v Dx: has surgery in 2008 for a pituitary adenoma. Feb 2016 debulk the pit tumor v Symptoms: in 2008 the tumor was pressing on his right optic nerve causing vision loss. Recently he was having memory problems

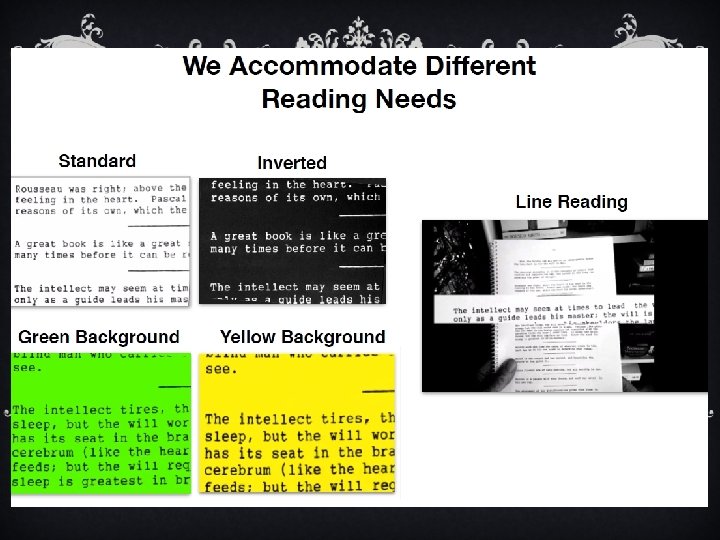
J. S. v c/o biggest problem is glare/lighting. His new cubical at work has fluorescent lights and he can not control his own lighting. The new cubicle is only waist high allowing light from other desks. He needs print to be 12 pt size, reverse contrast, and he needs walls so he does not get extra glare. v Has a CCTV v Magic on his computer. – adaptive computer software v Letter to his employer

J. S. v VA cc 2018: OD: 20/60 OS: 20/40 v ( worse from 2017: OD: 20/30 OS: 20/25) v Letter written to his employer v Filters and he likes FL 41 - fluorescent light glare

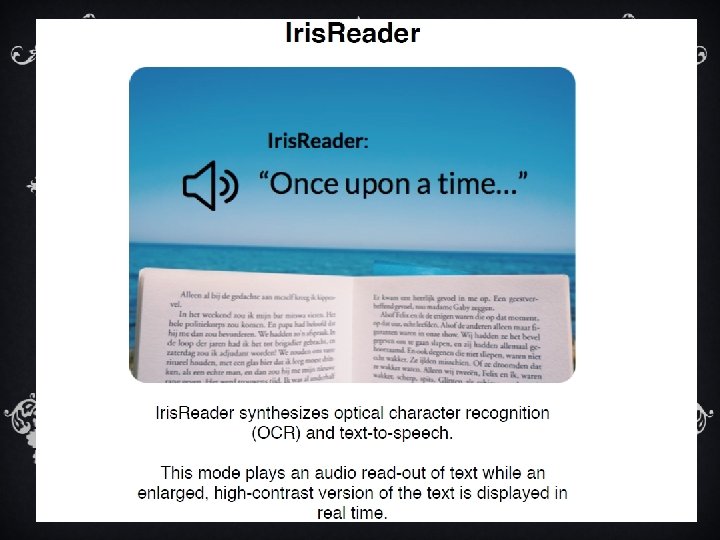
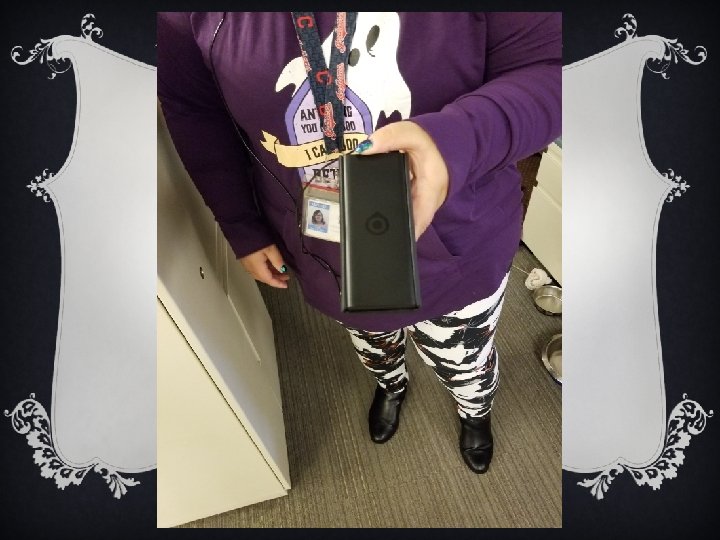
ELECTRONICS v Hand held CCTV- RUBY v Desk top CCTV v Omni reader- scanner v Orcam v Iris vision- uses the Samsung galaxy smart phone v Accessibility Apps on i Phone- Erin will discuss

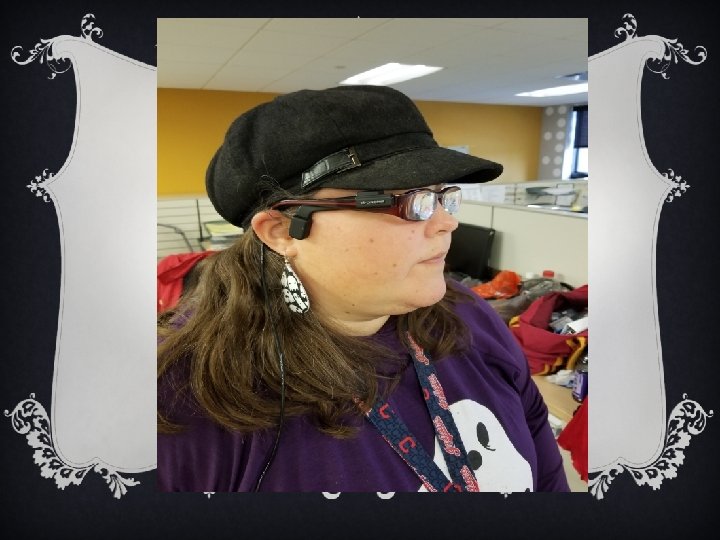
IRIS VISION v 69 yo M v h/o optic atrophy 2/2 swelling in the brain from a car accident in 1985. v Entering VA : OD: NLP OS: 3/100 Nv: 63 pt @ 30 cm v Wants something portable so he can read when not at home. v Has a CCTV that works well for him at home v Wants to recognize faces.

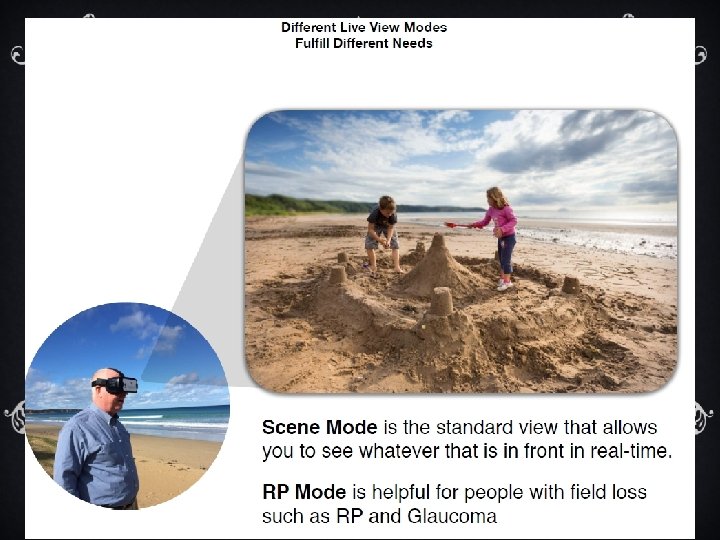
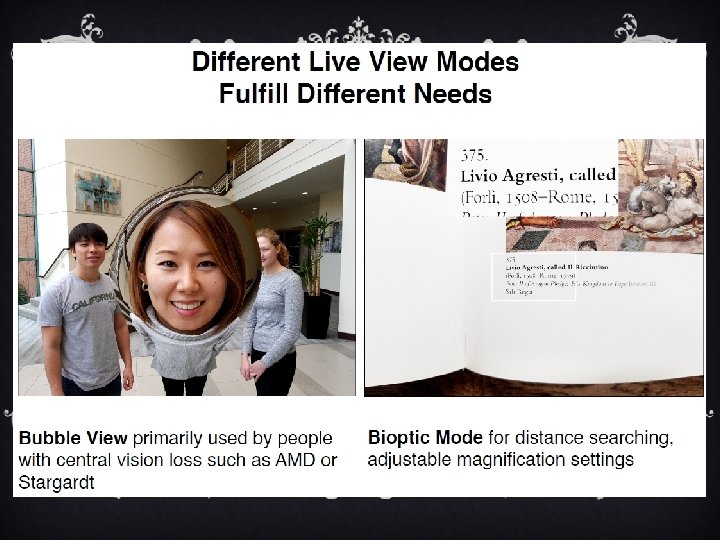
IRIS VISION v Uses Samsung Galaxy S 7 smart phone v Uses Virtual realty glasses v It uses the camera on the phone itself as a CCTV camera v Digital binoculars on your face v Two modes; live view mode reading mode


ORCAM v 35 yo WF v Dx: aniridia OU, advanced juvenile glaucoma OU, aphakia OU failed PK OS v Corrected Visual acuities; OD: 20/250 -1 OS: HM@1” v Goals: needed something to help her in stores v Currently uses : Merlin at home, Onyx at work, magnifier on her smart phone, 7 x/ and 10 x ill hh for spot reading labels v Works as a licensed TVI and LV rehab therapist

ORCAM v We do not sell the Or. Cam v You need to contact the company if patients are interested v Clip on to your glasses and it will read labels and faces for you.

v It is best used to read to you, the groceries labels, text, long or short term. It can identify currency, some facial recognition has to be taught. Product recognition. v Does it work for distances? It works best intermediate for reading, however, the print has to be standard font. Not fancy. Not hand written text v It’s light weight, convenient- newest model is wireless and magnetizes to glasses frame v OCR – optical character recognition

THANK YOU v We hope you enjoyed our presentation v We look forward to working with you and your patients and helping them reach their goals. v I would like to present to you, Erin St. Denis our OT
- Slides: 64