LOW BACK PAIN SHARLEEN A SUICO MD FAAPMR

LOW BACK PAIN SHARLEEN A. SUICO, MD, FAAPMR University of Toledo Medical Center July 6 th, 2017

Objectives Review of spine anatomy Discuss common pathologies for low back pain Explore treatment options for low back pain pathology

Spine Anatomy Review

SPINE ANATOMY Bones Joints Ligaments Muscles Nerves

Bones - Vertebrae � 7 Cervical � 12 Thoracic � 5 Lumbar � 5 Sacral � 4 Coccygeal

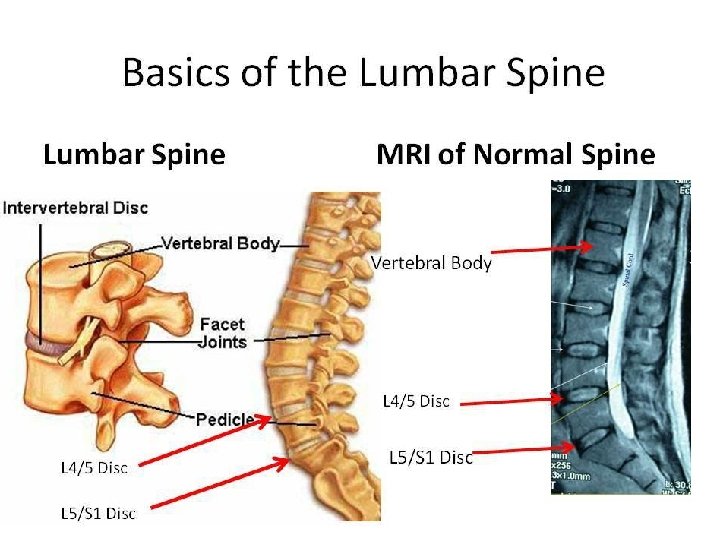
Bones – Vertebral Body

Bones – Lumbar Vertebrae

Bones – Sacrum

Bones – Sacrum
 Zygapophyseal (Facet) Vertebral")
Joints of the Vertebral Column Uncovertebral (C 3 -C 7 only) Zygapophyseal (Facet) Vertebral body endplate-discendplate

Vertebral Endplate-Disc

Ligaments

Ligaments

Intrinsic Back Muscles

Intrinsic Back Muscles

Nerves - Spinal nerves exit above vertebra until C 8 nerve root (below C 7/above T 1) - Below C 7, nerve roots exit underneath corresponding vertebra

Nerves

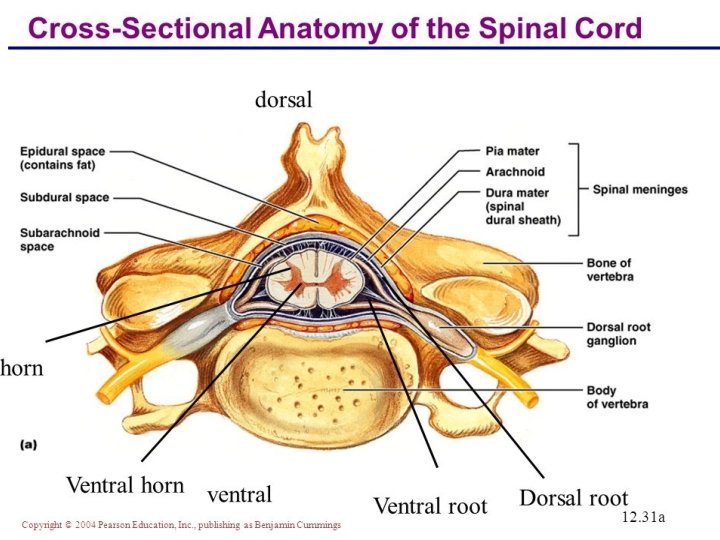
Spinal Cord Anatomy Spinal cord opiate receptors are in the dorsal horn Rexed Lamina I � Mu and delta receptors Rexed Laminae II to V � Kappa receptors

Nerves – Facet Innervation Facet joints – dual innervation Cervical: from “that level” and “level below” = C 5 -C 6 facet innervated by medial branches from C 5 and C 6 Thoracic and Lumbar: from “that level” and “level above” = L 4 -L 5 facet innervated by medial branches from L 3

Nerves – Intervertebral Disc Innervation Nucleus pulposus lacks innervation Anterolateral annulus fibrosis: ventral rami and gray rami communicans Posterior annulus fiborosis: sinuvertebral nerve (branch of ventral

Spine Pathology

Spine Pathology Disc disorders Bone disorders � Spinal stenosis � Spondylolysis � Spondylolisthesis Joint disorders � Facet � Sacroiliac joint dysfunction/sacroiliitis

Disc Disorders Age 30 -40 years Highest prevalence at L 4 -5 or L 5 -S 1 ¾ will resolve with conservative care in 6 mos to 1 year Nucleus pulposus migrates through the annulus fibers � May initiate release of phospholipase A 2 activates inflammatory mediators (leukotrienes, prostaglandins, platelet activating factors, bradykinins & cytokines)

Disc Disorders Classification Bulging disc No annulus defect; Disc convexity beyond vertebral margins Prolapsed disc Nuclear material protrudes into annulus defect Extruded disc Nuclear material extends to PLL Sequestered disc Nuclear fragment free in canal

Disc Herniations Etiology: � Spontaneous � Lifting activities � Coughing/sneezing � Bending/twisting activities Clinical features � Symptoms depend on herniation location � Acute discomfort radiating down limbs � Weakness, numbness, paresthesias � Lateral lumbar list or shift

Disc Herniation A = Central Herniation B = Posterior Lateral Herniation affecting L 5 Nerve root C = Far-lateral Herniation affecting L 4 Nerve root

Disc Herniations Exacerbations with lumbar motion � Forward flexion – central and posterior-lateral HNP � Extension – lateral HNP � Sitting � Coughing � Sneezing � Valsalva maneuvers � Neural tension tests Lasegue’s Test – supine SLR Seated straight leg raise

Neural Tension Tests Supine SLR Seated Straight Leg Raise

Internal Disc Disruption Degradation of internal architecture of disc w/o gross herniation Associated with annular fissure & nuclear tissue disorganization Can lead to chemical and mechanical stimulation of nociceptive fibers Axial discomfort from endplate fractures d/t excessive loads Grading 0 No annular disruption 1 Inner 1/3 annular disruption 2 Inner 2/3 annular disruption 3 Outer 1/3 annular disruption +/ - circumferential spreading

Degenerative Disc Disease

DDD vs Disc Herniation

Bone Disorders – Spinal Stenosis Degenerative changes disc space narrowing, vertebral body osteophytosis and joint arthropathy Limb pain syndrome usually ~50 yrs of age L 3 and L 4 most common levels Central vs Lateral Stenosis � Lateral Stenosis subdivided into 3 areas of entrapment A. B. C. Lateral recess Mid Zone Intervertebral Foramen

Central Spinal Stenosis

Lateral Stenosis Far lateral stenosis Lateral recess stenosis
 Vascular Discomfort Numbness, aches, pain Cramping, tightness Location")
Spinal Stenosis CLAUDICATION Types Neurogenic (Pseudoclaudication) Vascular Discomfort Numbness, aches, pain Cramping, tightness Location Buttock, thigh, calf Calf Exacerbation Standing, walking, lying flat Walking, cycling Bicycle test Painless Painful Downhill walking Painful Painless Uphill walking Painless Painful Remission Flexed position, bending, sitting Standing, resting, lying flat Associated Factors Back pain, decreases spine motion, atrophy, weakness, normal pulses Rare back pain, normal spine motion, rare atrophy or weakness, abnormal pulses, loss of hair, shiny skin

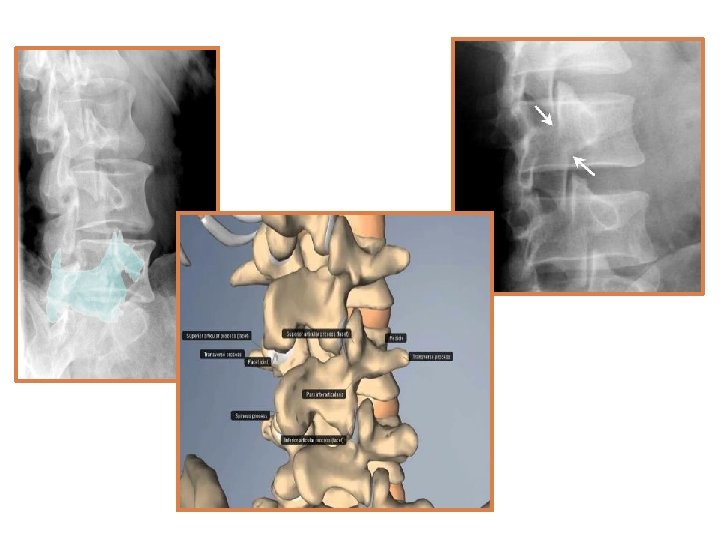
Bone Disorders - Spondylolysis Vertebral defect most commonly seen in children and adolescents L 5 vertebral level Pars interarticularis � Junction of pedicle, transverse process, lamina and the 2 articular process � Scotty Dog Hyperextension forces Neurologic exam should be normal

Bone Disorders Sponydylolisthesis Spondylolisthesis Slippage of vertebral body compared to the one below Most commonly seen at lumbar vertebral level Males 2 -4 x greater

Clas s Type Age Criteria I Dysplastic Child Congenital abnormality of LS Z-joint II Isthmic (most common) 5 -50 Pars fracture (A), which is most common at L 5 -S 1 or elongation (B) III Degenerativ e Elderl y Facet arthrosis causing subluxation. Common L 4 -5 IV Traumatic Youn g Acute fracture other than pars V Pathological Any Generalized disease: Cancer, infection, metabolic VI Postsurgical Adult Excessive resection of neural arches or facets causing an unstable structure

Spondylolisthesis Grade 1 Spondyloptosis
 Sustain")
Joint Disorders – Facet Syndrome True synovial joints (capsule, meniscus and synovial membrane) Sustain progressively increasing compressive loads down the spine, reaching ~12– 25% in L spine As disc height decreases, greater the load Pain exacerbated with rotation and extension Referred pain can be non-dermatomal No neurologic abnormalities

Facet Arthropathy

Joint Disorders - Sacroiliitis L-shaped articulation between sacrum and ilium � Synovial joint anteriorly � Syndesmosis posteriorly Acute or gradual back, buttock, leg or groin pain w/ TTP over joint Increased discomfort w/ positional changes Discomfort w/in assoc. mm – quadratus lumborum, erector spinae, & piriformis muscles
 � Gaenslen test �")
Sacroiliitis Provocative Tests Provocative Diagnostic Tests � FABERE (Patrick’s test) � Gaenslen test � Iliac compression test � Tenderness to palpation Non-provocative Diagnostic Tests � Yeoman’s test � Gillet’s test � Seated flexion test

FABERE’S TEST GAENSLEN’S TEST ILIAC COMPRESSION TEST

YEOMAN’S TEST SEATED FLEXION TEST GILLET’S TEST

Sacroiliiac Joint Dysfunction

Treatment options

Treatment Goals – The 4 A’s Analgesia Adverse effects Aberrant behaviors ADLs

Physical Activity and Therapy Being physically active is important Patients need to learn correct ways to be active without overdoing it Physical Occupational Massage Aquatics Walking Circuit Training Chiropractor Accupuncture

Pain Psychology Cognitive Behavioral Therapy Heart rate regulation Deep breathing Progressive relaxation Guided imagery Biofeedback

Treatment Rehabilitation and HEP � Mc. Kenzie versus flexion biased Modalities � Heat � Ice � Electrical stimulation (E-stim or TENS) � Traction � Bracing Disuse atrophy

Interventional Procedures Diagnostic and therapeutic Image-guided injections to identify and treat areas of the spine that are pain generators Decrease pain transmission to the dorsal horn of the spinal cord – decreased pain signal propagation and translation to the brain Can decrease the amount of pain meds needed by delivering them to the source of the pain Help to delay or prevent surgery Help treat pain that may develop years after surgery Lasts on average 3 -4 months

Interlaminar ESI – AP view Lateral View AP View

L 5 Transforaminal ESI

Facet Joint Injection Oblique View AP View
")
Medial Branch Blocks (MBB)

Radiofrequency Ablation

Sacroiliac Joint Injection Ultrasound Guidance Fluoroscopic Guidance

Pain pump vs SCS Pain Pump Primarily focuses on nociceptive pain As well as neuropathic pain Place catheter into intrathecal space; connected to pump/reservoir system in subcutaneous tissue in abdomen Medications delivered directly to brain and spinal receptor to mediate pain Spinal Cord Stimulator Primary focus is neuropathic pain As well as nociceptive pain Place electrode leads into epidural space over the dorsal columns Believed to modulate recognition of pain primarily through the gate control theory

Pain Pump Medications Opioids � Morphine or hydromorphone � Sufentanil � Fentanyl � Methadone Local anesthetics � Bupivicaine � Ropivicaine Alpha-2 -adrenergic agonists � Clonidine

Thank you!!!
- Slides: 64