LOW BACK PAIN Dr Zachary Stelmack ANATOMY OF

LOW BACK PAIN Dr. Zachary Stelmack

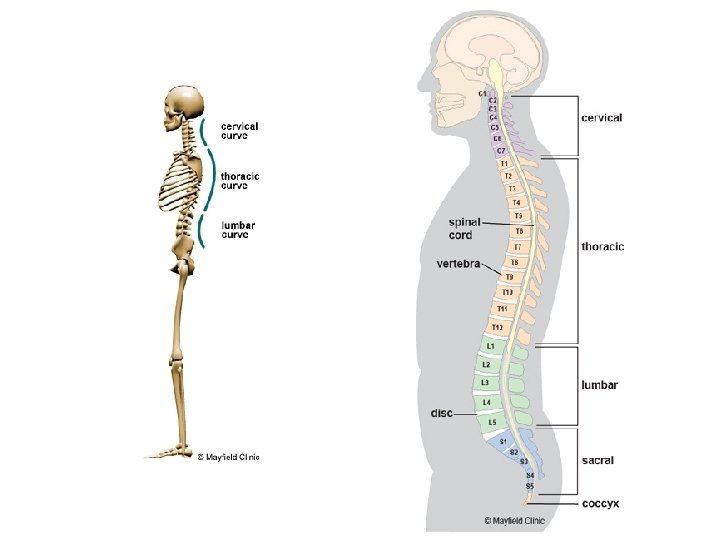
ANATOMY OF THE LUMBAR SPINE/PELVIS 5 lumbar vertebrae (bones of that make up your spine) L 1, L 2, L 3, L 4, L 5 1 Sacrum (not part of the lumbar spine exactly, but goes right along with it) 5 lumbar/Sacral Intervertebral discs L 1(L 1/L 2), L 2(L 2/L 3), L 3(L 3/L 4), L 4(L 4/L 5), L 5(L 5/S 1) Curve of the lumbar spine is set in extension, or convex Sacrum and iliac bones make up the Sacroiliac (SI) Joints

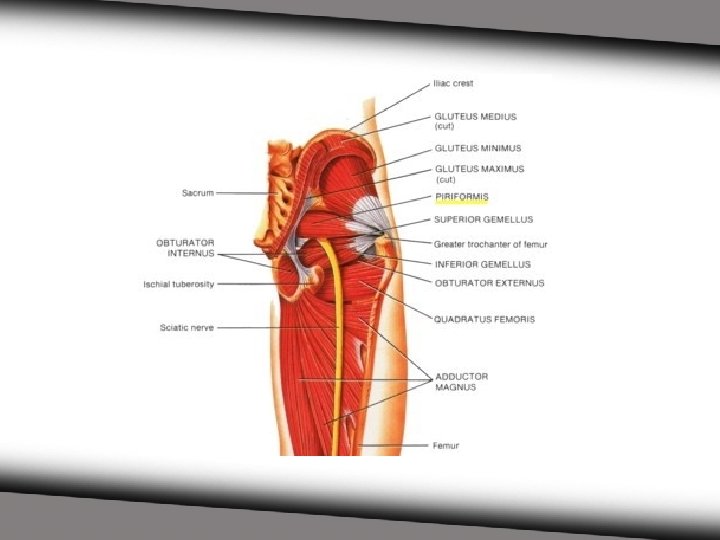
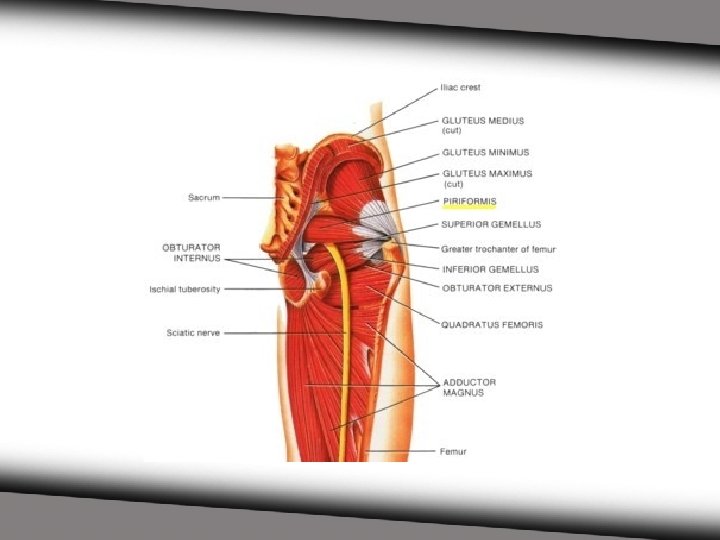
ANATOMY OF THE LUMBAR SPINE Many ligaments - ligaments attach bone to bone - they are there to prevent excessive, damaging motion Muscles common muscles found in the lumbar spine/associated with low back pain: quadratus lumborum trapezius multifidi lumbar paraspinal muscles/erector spine muscles piriformis (a part of pelvis musculature) latissimus dorsi gluteus maximus and medius psoas hamstrings quads




 flexion extension lateral flexion very")
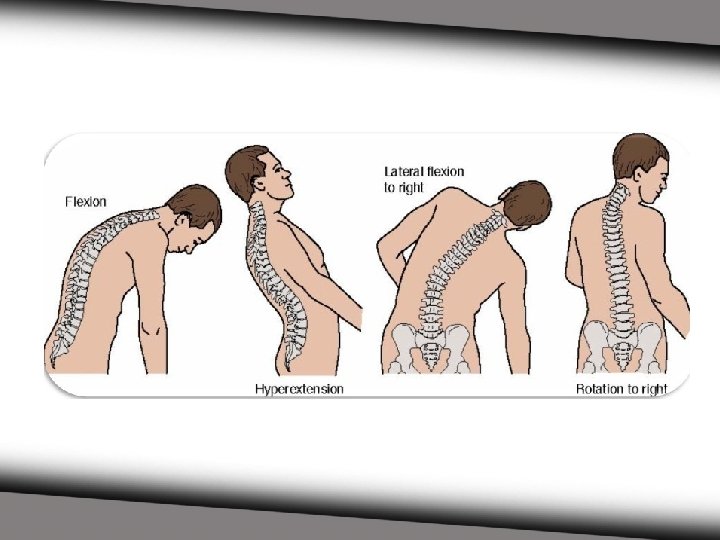
ANATOMY OF THE LUMBAR SPINE Range of Motion (ROM) flexion extension lateral flexion very slight rotation the pelvis performs flexion and extension

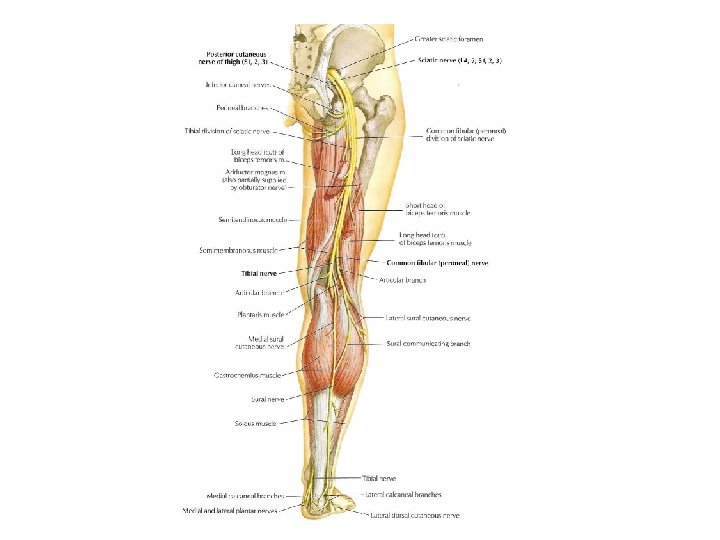
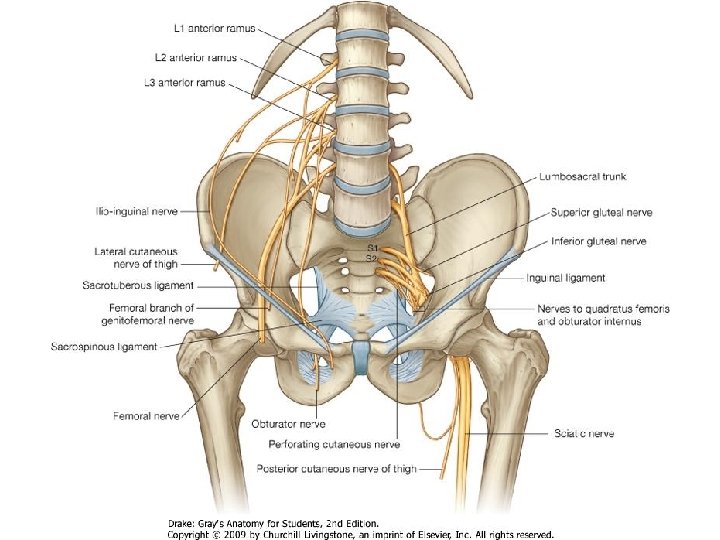
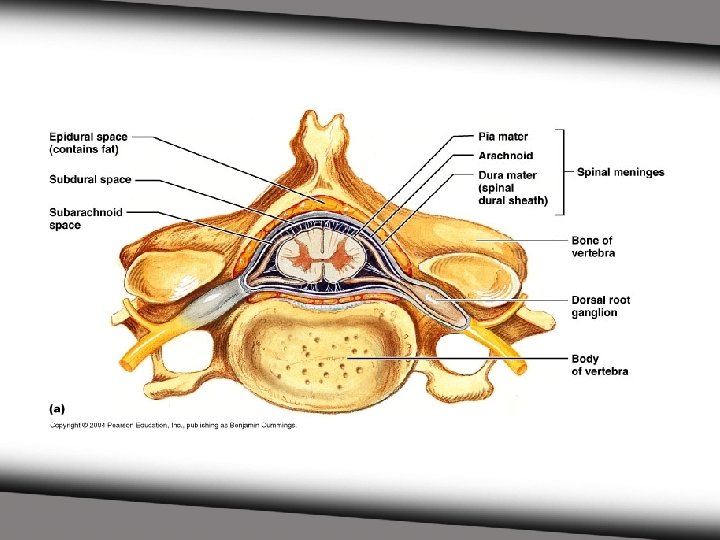
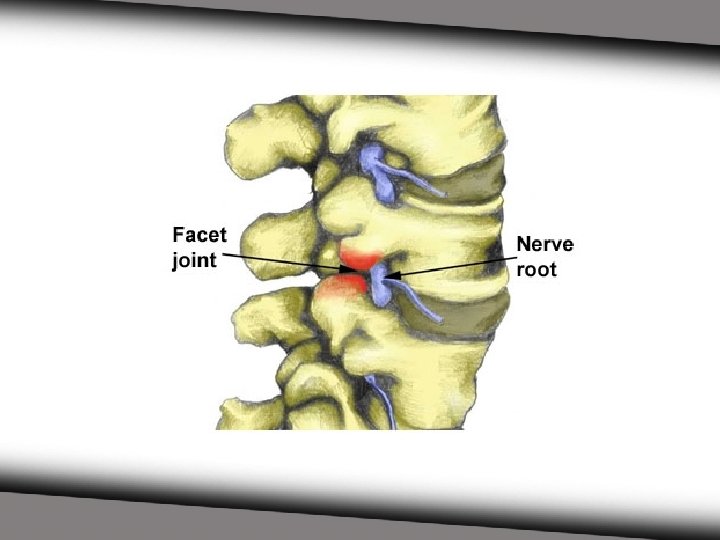
ANATOMY OF THE LUMBAR SPINE The spinal cord is protected as it sits in the canal made up of the vertebrae - this is called the vertebral canal Nerves exit the spinal cord through openings between the vertebrae Most common nerves: femoral nerve supplies front of thigh sciatic nerve supplies back of thigh/leg


 provides cushioning in between the vertebrae")
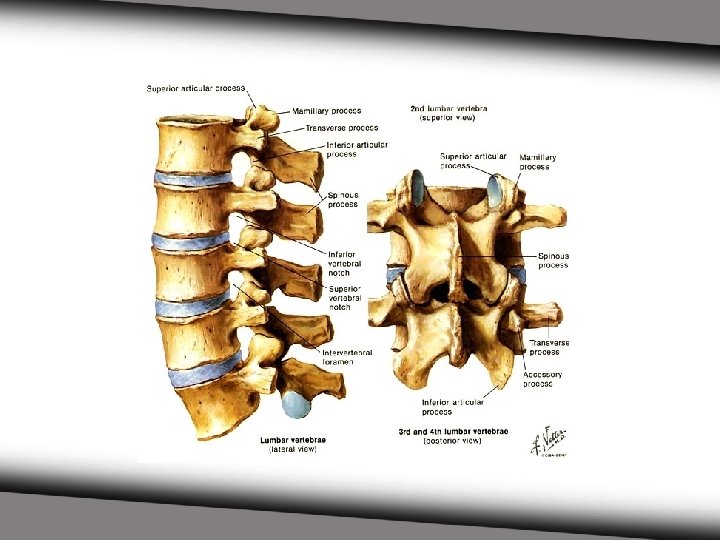
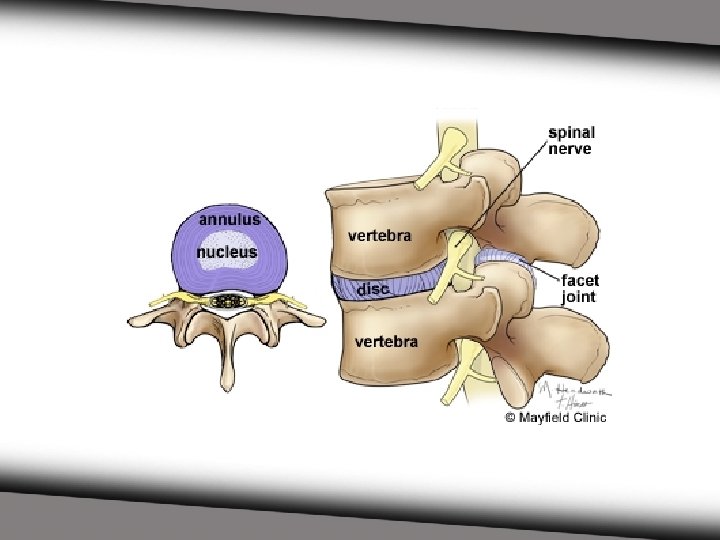
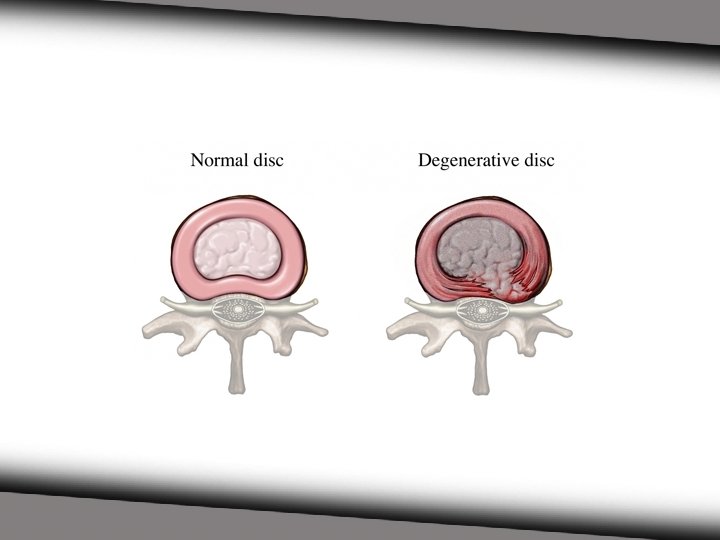
ANATOMY OF THE LUMBAR SPINE Intervertebral Discs (IVD) provides cushioning in between the vertebrae protects against compression 2 parts an outer annulus fibrosis (more fibrous) an inner nucleus pulposus (gelatinous-like)
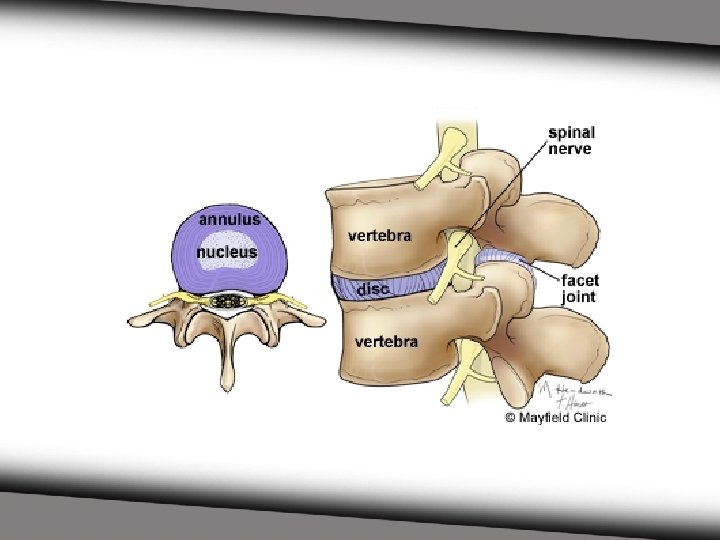

ANATOMY OF THE LUMBAR SPINE Joints of the Spine Facet Joints found in the back part of the vertebrae this is where movement occurs

WHAT CAN GO WRONG? Degeneration of the bones/joints/discs Growths Impingement -disc -nerve -ligament -spinal cord

WHAT CAN GO WRONG? Sprains/Strains -ligaments -tendons -muscles Breaks/Fractures Infection/Inflammation

WHAT CAN GO WRONG? *REMEMBER* - The nerves travel in between the vertebrae and it is the discs that keep the space open so they are not impinged Muscles and ligaments ensure proper range of motion and function - and most importantly: STABILITY and PROTECTION
 Tumors Bone degeneration Disc tears Disc bulge")
WHAT CAN GO WRONG? Bone spurs (growths) Tumors Bone degeneration Disc tears Disc bulge Facet joint degeneration Muscle/ligament sprains Inflammation

WHAT CAN GO WRONG? Most causes of pain all come down to inflammation, muscle tightness, and nerve impingement

MOST COMMON CONDITIONS ASSOCIATED WITH LBP Muscle Hypertonicity/Spasm, sprains/strains Lumbar Disc Degeneration/Disc Bulges Sciatica Arthritis Spinal Stenosis

Muscle Hypertonicity/Spasm, Sprains/Strains Overuse Improper movements Improper sleep injury

Muscle Hypertonicity/Spasm, Sprains/Strains Muscles tighten Decreases normal range of motion Causes mostly local pain or diffuse pain Most common muscles involved: lumbar paraspinals/erector spinae, quadratus lumborum, and piriformis, hamstrings, quads PAIN: usually dull/achy, stays local or slightly diffuse - Stiffness, tightness

Muscle Hypertonicity/Spasm, Sprains/Strains Prognosis: good, if taken care of Treatments consist of muscle therapy, stretches, therapeutic exercises, adjustments If left untreated: can heal inappropriately muscle tightness causes decreased range of motion and eventually degeneration of the joint more likely to frequently have re-injury muscle imbalance and eventually involvement of other muscles

Muscle Hypertonicity/Spasm, Sprains/Strains NOTE: almost every issue of the spine involves muscle hypertonicity

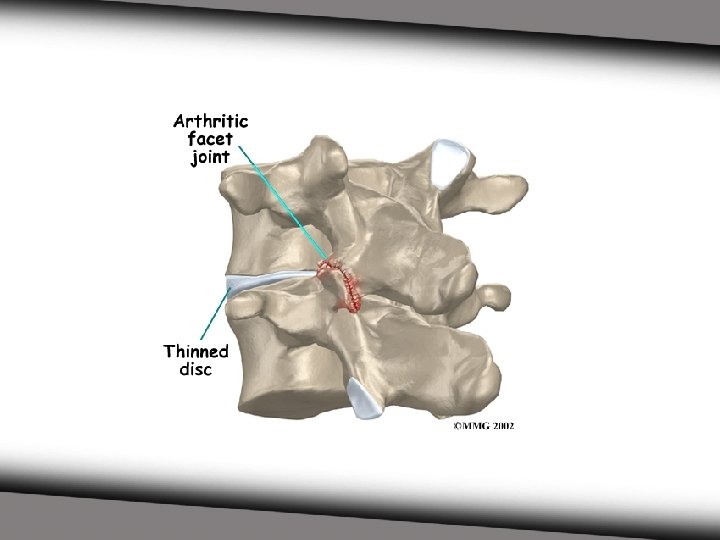
Lumbar Disc Degeneration/Disc Bulge Degeneration is more common after the age of 30 Disc Bulge/Herniation are more common under the age of 30 Outer disc can tear Disc can bulge Disc can degenerate

Lumbar Disc Degeneration/Disc Bulge All of these things cause impingement Compress tissue Compress nerves PAIN: usually diffuse, sharp at times, dull achy pain can be positional based pain can be radiating



Lumbar Disc Degeneration/Disc Bulge Improper movements Lifting heavy objects often Injury/falls Age Obesity TOO MUCH FLEXION

Lumbar Disc Degeneration/Disc Bulge Prognosis: good if caught early on, if left alone can develop into chronic condition Treatment: muscle therapy exercises/positional exercises distraction/traction If left untreated: chronic, travel, arthritis

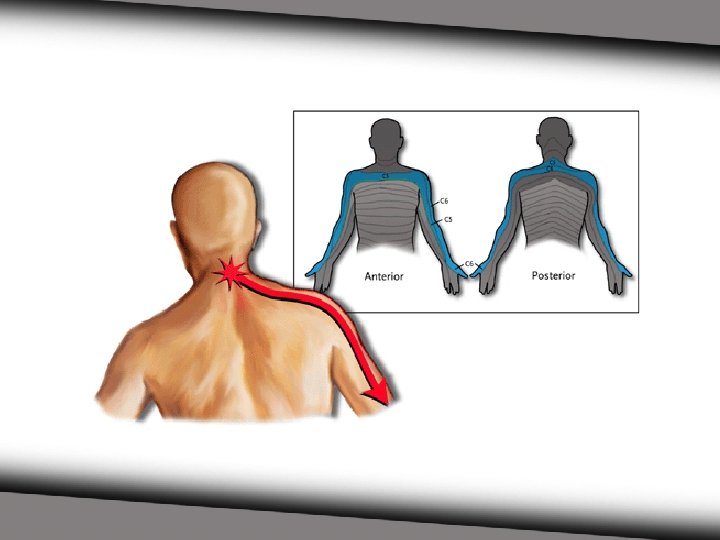
RADIATING PAIN When pain “radiates”, or MOVES some distance away from the initial site of what is causing the pain. It travels down a nerve(s) being effected/impinged/encroached upon. For example: sciatica This is called peripheralization When a patient has radiating pain, one way we judge improvement is by how much pain is centralizing (coming back to original sight of pain) PAIN: sharp, diffuse, burning, numbness, tingling, pins and needles Touching area of radiation won’t change the pain intensity.


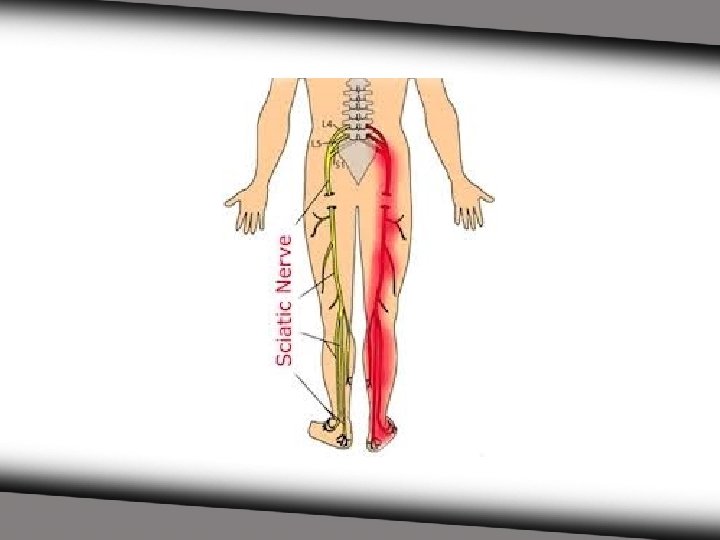
SCIATICA Radiation of pain down one or both legs due to irritation to the sciatic nerve. Can radiate anywhere from buttocks to big toe. Radiation will be continuous typically. The further the radiating pain travels indicates the significance of the condition. The sciatic nerve is the largest nerve in the body. - it travels from the lumbar spinal cord region to the foot - mostly in the back of the leg

SCIATICA Causes: impingement/irritation of the sciatic nerve - bulging disc - degeneration of spine - nerve growth on sciatic nerve - inflammation at the spine or spinal cord, or nerve - very commonly A TIGHT PIRIFORMIS MUSCLE

SCIATICA Prognosis: great if treated right away - the longer it has been chronic, the harder it is to dissipate Treatment: - tissue/muscle therapy to involved muscles - distraction of the lumbar spine/traction - positional exercises - stretches - therapeutic exercise

ARHRITIS Inflammation and degeneration of bone and cartilage of any/many joints Degeneration causes: - pain - bone spurs - narrowing of spaces where nerves are - weakness of bone - stiffness of muscles/tendons/ligaments trying to stabilize effected joint

ARTHRITIS Rheumatoid Arthritis - systemic inflammatory disease/autoimmune - occurs on both sides in same areas - typically spreads Osteoarthritis - can occur in only one joint, one area, one sided - typically occurs in places of high stress/usage - common at areas of old injuries Pain is very similar for both - dull achy, sharp, stiffness - radiating pain common

ARTHRITIS Prognosis: moderate relief, chronic/intermittent reoccurrence - pain brought down to manageable intensity and frequency HOWEVER, PREVENTION IS KEY! Treatment: - tissue/muscle therapy to involved muscles - distraction of the lumbar spine/traction - stretches - therapeutic exercise - ultrasound therapy -laser therapy - anti-inflammatory diet, supplements (anti-inflammatory and support) MOTION is LOTION

SPINAL STENOSIS Encroachment or Narrowing of the vertebral canal onto the spinal cord. Patient usually feels better/relief with flexion. Extension increases symptoms significantly.
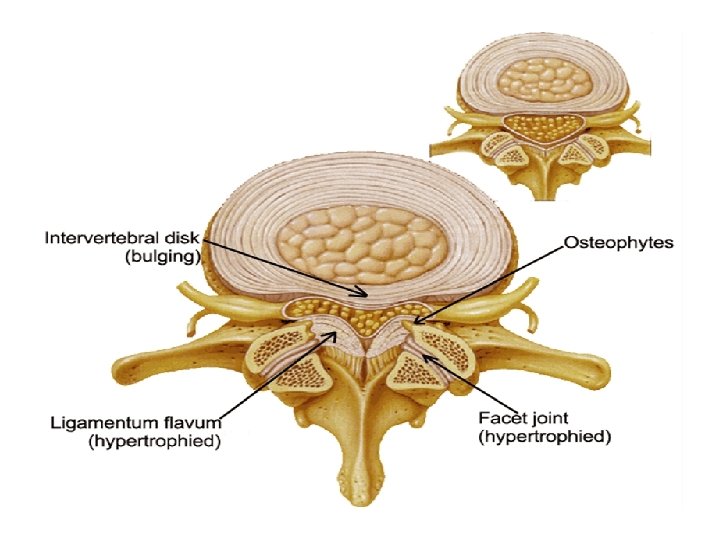

SPINAL STENOSIS Causes: bone spurs arthritis bulging disc facet hypertrophy/inflammation/arthritis spine degeneration

SPINAL STENOSIS Prognosis: minimal to moderate, chronic typically - early intervention is key Treatment: - muscle therapy - flexion and distraction of spine - therapeutic exercise - bike riding/cycling - correction of encroachment - anti-inflammatory diet/supplements

WHAT CAN YOU DO NOW? Insert some things from healthy daily living exercise - Put one leg up when standing for long periods of time -The “captain morgan” stance

WHAT CAN YOU DO NOW? PILLOW AND POSITION Pillow depends on position Side Sleeper pillow: thickness needs to be that of the length between the ear and the tip of your shoulder also, pillow between the legs (6 inches or so) try to avoid hand under face or pillow Back Sleeper pillow: very flat, or can use neck pillow or rolled towel behind neck Stomach Sleeper try to avoid very flat pillow

WHAT CAN YOU DO NOW? WATER increase water intake dehydration can lead to poor joints
")
WHAT CAN YOU DO NOW? 30 minutes of activity daily (NOT JUST WORK ACTIVITY) Walking, biking, swimming, dancing, jogging, sports, etc. AVOID: sit-ups, crunches, equalized weight machines ALWAYS stretch/warm up and cool down

WHAT CAN YOU DO NOW? SITTING no slouching feet flat on the floor (do not keep legs crossed) do not site for periods more than 20 -30 minutes - take breaks make sure work station is straight forward and eye level towel or lumbar roll behind lumbar spine shoulders back and down don’t “push off” to get out of chair, plant feet and drive through heels! POSTURE BREAKS!

WHAT CAN YOU DO NOW? Waking Up DO NOT just jump out of bed in the morning do some light stretches first Upon getting out of bed, AVOID flexion (sitting, squatting, bending forward) for the first 30 mins-1 hour

WHAT CAN YOU DO NOW? THROUGHOUT THE DAY Avoid staying in the same position for long periods of time Lift with your legs Stretch often No aprons/heavy necklaces/lanyards Do not favor a side example: purses, bags, etc. NO luggage ladies!

WHAT CAN YOU DO NOW? THROUGHOUT THE DAY DO NOT self adjust! Do not strain over heavy objects, ASK FOR HELP! When something hurts, get it checked out. Yes, things heal with time but not usually properly!

QUESTIONS?
- Slides: 65