LONG ACTING REVERSIBLE CONTRACEPTIVES The Basics Objectives Explain

LONG ACTING REVERSIBLE CONTRACEPTIVES The Basics

Objectives • Explain the basic information for history taking and counseling patients on LARCs (IUDs and Implants), including contraindications. • Utilize online resources for patient education and clinician references regarding medical eligibility. • Demonstrate the techniques for insertion and removal of LARC.

Contraceptive users in the US • 61 million US women in childbearing years • ~43 million of them (70%) are at risk of unintended pregnancy • 62% of women of reproductive age currently using some form of contraception • Couples who don’t use contraception have ~85% chance of experiencing pregnancy over the course of a year
 of pregnancies in the US are unintended Unintended – Mistimed 27%")
Nearly half (45%) of pregnancies in the US are unintended Unintended – Mistimed 27% Intended 55% Unintended. Unwanted 18%

Unintended pregnancy by consistency of contraception use Consistent use 5% Nonuse 54% Inconsistent use 41%

One year failure rates Effectiveness Contraceptive Typical-use pregnancy rate Perfect-use pregnancy rate Ineffective Chance 85% Less effective Condoms 14% 3% More effective Pill/patch/Ring 8% 1 -3% Highly effective IUDs 0. 8 – 2% Injectable 0. 1 – 0. 3% Implant 0. 1 – 0. 3% Sterilization (male and female) 0. 1 – 0. 3%

Pill F Sterilization M Condoms IUD M Sterilization Withdrawal Injectable Vaginal Ring Fertility Awareness Implant Patch EC Other None Contraceptive Methods in the U. S. 25. 00% 20. 00% % of women 15. 00% at risk of unintended pregnancy* 10. 00% 5. 00% 0. 00%
 CDC recommendations for specific contraceptive methods with")
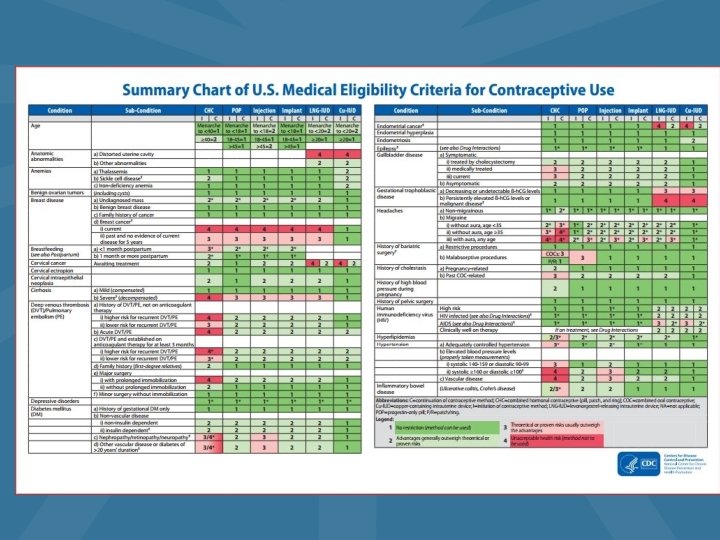
The MEC US Medical Eligibility Criteria (MEC) CDC recommendations for specific contraceptive methods with certain medical conditions

MEC Categories of Safety

There’s an APP for that: - Can be downloaded on i. OS and Android operating systems (https: //www. cdc. gov/mobileapp. html)

Another helpful APP… • Contraceptive Point-of-Care App

Cases In LARC management

Shani • 21 years old • Post-partum 4 weeks • Asking about tubal sterilization because she’s not good with pills

Sterilization by Education • If graduated college, 13% had tubal ligation • If some college, 29% had BTL • If graduated HS, 42% had BTL • If no HS graduation, 55% had BTL

Young women and sterilization • 20% of women selecting sterilization at age 30 years or younger later express regret

What about an IUD for Shani? • Lower discontinuation rates in post-partum women • Insertion ok as early as 4 weeks post-partum, endorsed by CDC • Immediate post partum insertion also effective, now covered by most insurances • Non-patient-dependent method enhances adherence

Ultimate goal: Patient-Centered • If, after all the information, she still wants sterilization, we need to honor her decision making

IUD Options
 • No hormones • Menses continues • Menses")
IUD Comparison Copperu IUD (Para. Guard™) • No hormones • Menses continues • Menses can be heavier, more cramps • Effective as Emergency Contraception within 5 days • Duration 10 -12 years Levonorgestrel 52 mg IUD (Mirena™, Liletta™) Levonorgestrel 18. 5 mg IUD (Klyeena™) Levonorgestrel 13. 5 mg IUD (Sklya ™) • Progestin treats menorrhagia, anemia • Causes amenorrhea • Duration 3 - 7 years • Marketed for nulliparous women • Duration 5 years • No evidence yet for menorrhagia, anemia • Does not change menses • Duration 3 years
: 380 mm 2 copper exposed")
Mechanism of Action: Copper IUD Copper-releasing IUD (Para. Guard™): 380 mm 2 copper exposed on plastic T base • • • Interferes with sperm motility. Causes spermicidal foreign-body reaction. Alters uterine environment, “hostile” to sperm.

Mechanism of Action: Hormonal IUDs • Hormone-releasing IUD levonorgestrel on its arms and stem released at decreasing rate with time • Thickens cervical mucus (acting as a sperm barrier) • Thins uterine lining. • Partial inhibition of ovulation. • Presence of plastic alone may have some efficacy

Maggie • 35 years old • Heavy smoker

MEC Categories of Safety

• Age Concerns with Maggie… and evidence for safety – No restriction for IUD or implant – MEC Category 2 for women < 20 years old • Consider expulsion risk and baseline STI risk • Smoking status – Regardless of amount, NO restriction for any IUD

MEC Category 4 conditions for IUDs • Current PID, gonorrhea, chlamydia (Category 4 for initiation only) • Certain anatomic abnormalities (May interfere with proper IUD placement) • Endometrial cancer (Initiation only) • Active pregnancy • Unexplained vaginal bleeding (Suspicious for serious condition)

Krystal • 24 year old • G 2 P 1 • History of chlamydia as a teen

STIs and PID • IUDs do NOT increase rates of STIs – Screen for STIs at IUD insertion – Do not remove IUD for STI treatment – No need for antibiotic prophylaxis at IUD insertion • 0. 0001% PID risk transiently higher for 20 days after IUD insertion, then back to baseline population levels – Even low PID rates with good insertion technique and low baseline STI rate – Modern IUD strings do not facilitate ascent of infection – Do not remove IUD for initial PID treatment

STIs and IUDs • MEC category 4: – Current PID or current gonorrhea or chlamydia (insertion only) • MEC category 2: – PID, gonorrhea and chlamydia for continuation – Trichomonas and BV for insertion – Very high risk for STI or HIV • MEC Ctategory 1: – HIV infected or clinically well on ARV

Kerry • • 18 year old G 1 P 0 DM Type 1 Borderline HTN

Medical Eligibility • Progestin IUD or Implant does not alter glycemic control in patients with DM 1, does not affect blood pressure • Copper IUD is approved for almost all medical conditions: – Cardiovascular disease – Hypertension – Migraines – Smoking – Lipid disorders – Diabetes

Tammy • 35 year old • Heavy periods with anemia

LNG 52 mg IUD – Side Effects • Spotting, bleeding, cramping: increased in first 3 months • Amenorrhea common • Expulsion: 2 -12% in 1 st year • Perforation: < 0. 01% at time of insertion • Headaches, acne, mastalgia: < 3% in first month

LNG 52 mg IUD- Medical Advantages • Cramps and menorrhagia improve • 90% decrease in overall blood loss • Decreases number of invasive treatments for DUB, fibroids • Decreases risk of ectopic pregnancy • May protect against endometrial cancer • Decreases peri-menopausal symptoms

LNG 13. 5 mg • Only 6% have amenorrhea after one year • No evidence that lower dose means less progestin side effects • 50% of failures were ectopic pregnancies

Non-contraceptive benefits of LNG 52 mg IUD • Treatment of menorrhagia – Including in women with uterine fibroids and adenomyosis • Treatment of pain in women with endometriosis • Prevention of endometrial hyperplasia in perimenopausal women using estrogen therapy • Prevention of endometrial proliferation and polyps in breast cancer survivors taking tamoxifen

Myths about IUDs • Must IUDs be inserted during menses? • Can the IUD be used as emergency contraception?

Pamela • Has had an IUD for two years • Positive pregnancy test • You can feel the strings

IUD and Ectopic Risk • Ectopic pregnancy rate is the same in IUD users as in the general population, not higher • Pregnancy rate in IUD users is very low • However, if pregnant with IUD in place, one out of 2 -3 pregnancies in IUD users will be ectopic. URGENT NEED FOR ULTRASOUND TO LOCATE THE PREGNANCY.

Jennifer • 18 years old • Her mother was just diagnosed with a Pulmonary Embolism, she wants something other than pills • Not ok with having a pelvic exam.
 Inhibits ovulation Thins endometrium")
Etonogestrel Implant- Mechanism of action • • Hormone-releasing implant (Nexplanon®) Inhibits ovulation Thins endometrium Thickens cervical mucus
 – Breast cancer, active or")
Contraindications to implant • MEC Category 4 (Absolute contraindications) – Breast cancer, active or < 5 years ago – Pregnancy – Allergy • MEC Category 3 (Relative contraindications) – History of breast cancer > 5 years ago – Severe liver disease – Ischemic heart disease, history of CVA – Unexplained vaginal bleeding suspicious for serious cause – SLE + antiphospholipid antibodies
 Relatively")
Advantages of Implant High efficacy No need for pelvic exam (teens like this) Relatively simple insertion Decreases pain with dysmenorrhea and endometriosis • Just as effective in obesity • •

Side effects of implant • At insertion- bleeding, infection, bruising but all very low risk • Irregular and unpredictable bleeding – ~ 15% of patients remove implant by 1 year • Emotional lability, headaches, acne < 2%

Quick Start: Timing of insertion • < 7 days from LMP, insert today, backup for 1 week • > 7 days from LMP and unprotected sex since then, insert today if patient desires, use backup for 1 week, repeat urine hcg in 2 weeks

Nexplanon Insertion • Measure 8 -10 cm above the medial epicondyle • Mark that spot, then place a guiding mark 4 cm proximal • Inject lidocaine with epi along track between spots

Nexplanon Insertion

Nexplanon Insertion/removal challenges • Insertion – Insensitivity to anesthesia – Inserting device too shallow or deep • Removal – Deep insertion/IM placement – Migration – Broken device

Troubleshooting IUD issues • Bleeding pattern problems – Short term NSAIDs or OCPs plus time • Pain problems – NSAIDs plus time (check placement, pelvic exam and/or US) • String issues – Leave long (3 -4 cm, can always shorten), cut at right angle, tuck behind cervix.

Challenges with IUD insertion • Discomfort/difficulty with speculum placement • Visualizing the cervix • Extreme uterine position/uterine distortion • Prior c-sections • Tight cervical os • Vasovagal reactions • Perforation

Uterine Positions

IUD Placement Tips • Use as short a speculum as possible • Give lidocaine 2 -3 cc prior to tenaculum placement, or use a paracervical block if especially difficult • Put traction on the tenaculum to straighten out the uterus • Very gently advance the sound, letting it follow the smooth surface of the canal

Sound vs Sound with dilation

Os finders

Challenges: IUD Removal • Can’t see strings • Embedded IUD • Malpositioned IUD

Ultrasound • To confirm if IUD in place if patient returns with concerns

Take Home Messages • You can do this! • LARC is a good option for patients • The risks are minimal • The benefits are enormous

- Slides: 58