Localization of culprit artery in STEMI Dr Bijilesh

Localization of culprit artery in STEMI Dr Bijilesh u Senior Resident, Dept. of Cardiology, Medical College, Calicut

q q Careful analysis of the Surface ECG is highly useful in localizing the culprit vessel and immediate prognostication Helps in deciding the need for an aggressive reperfusion strategy
 – Left anterior descending")
Coronary circulation q Left Main or left coronary artery (LCA) – Left anterior descending (LAD) • diagonal branches (D 1, D 2) • septal branches – Circumflex (Cx) • Marginal branches (M 1, M 2) q Right coronary artery – – – Conus , sinoatrial branch RV branch Acute marginal branch (AM) AV node branch Posterior descending artery (PDA)

q LAD large MIs – Supplies the anterior, lateral, anterior two-thirds of septum, and frequently the inferoapical segments of the left ventricle, proximal part of bundle branches q RCA – Perfuses sinus node (55%), AV node, posteromedial papillary muscle, inferior part of LV, RV, and variably also the posterior and lateral segments

q Circumflex branch – Posterior wall and variably inferior and lateral segments – Posterior wall involvement usually underestimated and under treated.

q q q SA node – RCA in 55% AV node – RCA in 90% Bundle of His – mainly RCA RBB – LAD LBB – L Ant branch – LAD L Post branch – LAD & Postr Desend A

Dominance q q q Supplies circulation to the inferior wall & inferior portion of the interventricular septum Passes crux and interventricular septum, giving rise to posterolateral branches & PDA Dominant artery also gives rise to the AV nodal branch

RIGHT DOMINANT

LEFT DOMINANT

Dominance q q RCA - 70% LCX - 10% Co - dominant – 20% Identifies patients at risk for extensive myocardial damage with complications

ST VECTOR q q Direction and displacement of the ST segment sum of direction and magnitude of all ST vectors Resulting main vector point in the direction of the most pronounced ischemia - ST elevation in that area Opposite area record (reciprocal) ST depression Lead perpendicular to dominant vector will record an iso-electrical ST segment

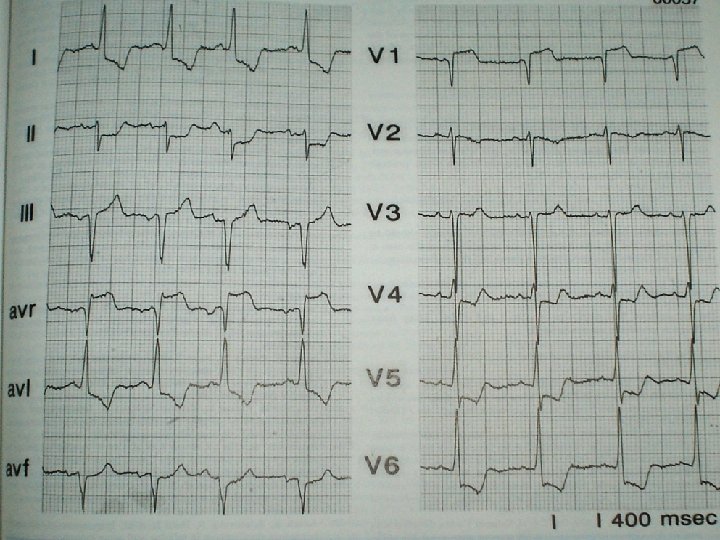
AWMI

ECG in AWMI q q STE in V 2, V 3, V 4 Behaviour of ST in other leads depends on the presence of ischemia in three vectorally opposite areas – Basoseptal area (1 st septal branch) – Basolateral area (1 st diagonal branch) – Inferoapical area ( when LAD wraps around apex)

Types of LAD occlusion q Proximal to 1 st septal and 1 st diagonal branch (40%) q Distal to S and D (40%) q Proximal to D 1 but distal to S 1 (10%) q Proximal to S 1 but distal to D 1 (10%)
")
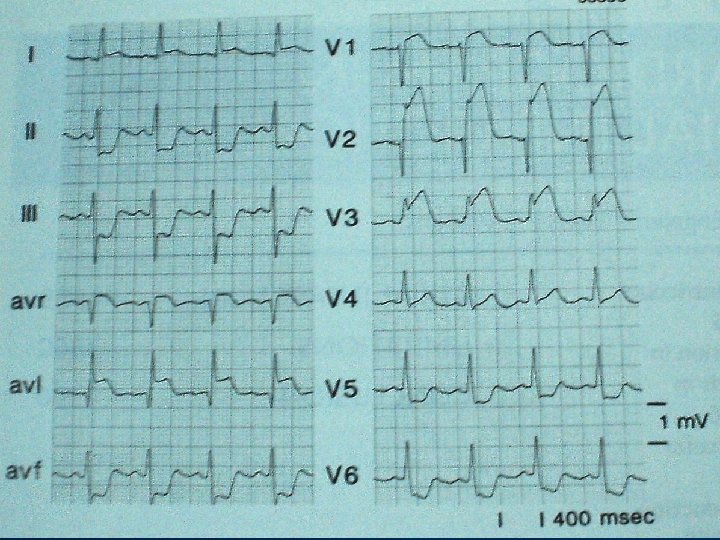
Proximal LAD occlusion (Dominance of Basal area)

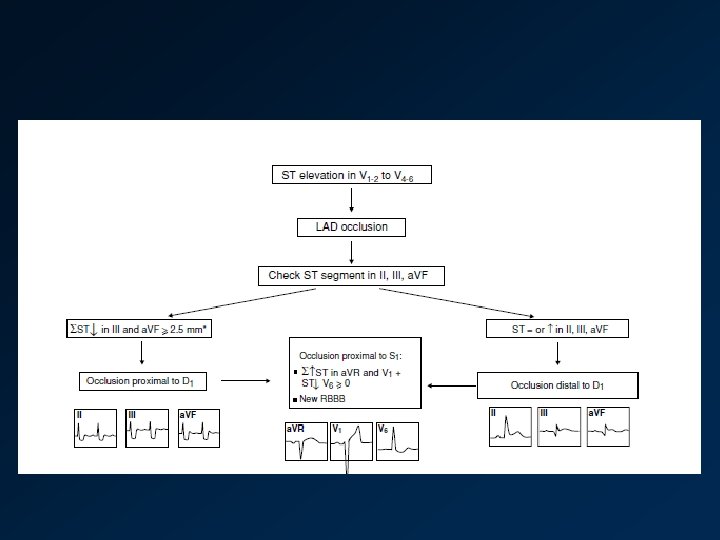
Direction of ST Vector and ECG Changes in Proximal LAD Occlusion
 q ECG… q RBBB q STE a.")
Proximal LAD occlusion (Dominance of Basal area) q ECG… q RBBB q STE a. VR and STE in V 1 > 2. 5 mm q ST depression in inferior leads and in V 5
")
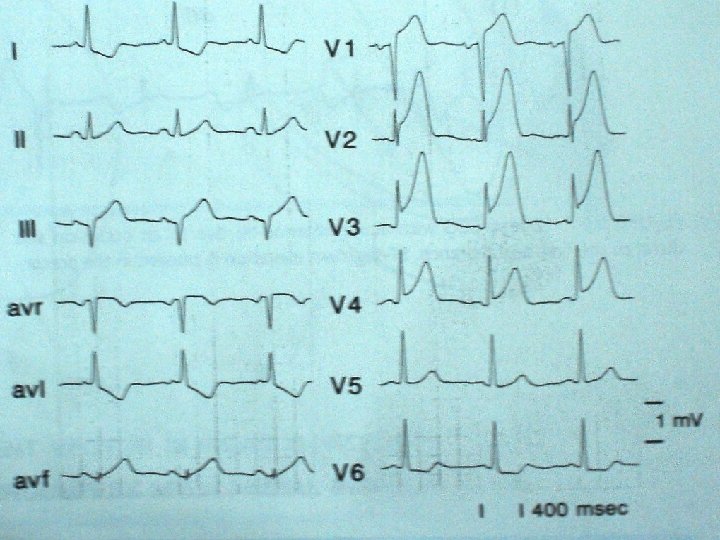
Distal LAD occlusion (dominance of inferoapical area)
 ECG… q Absence of ST depression in")
Distal LAD occlusion (dominance of inferoapical area) ECG… q Absence of ST depression in inferior leads q STE in inferior leads in addition to V 3 -V 6
--Proximal to S 1")
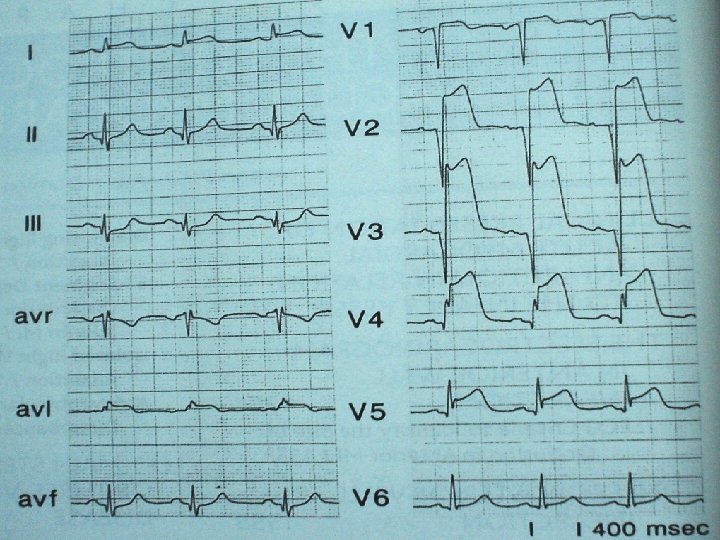
1 st Diagonal not involved (Dominance of septal area)--Proximal to S 1
 ECG… q STE in a.")
1 st Diagonal not involved (Dominance of septal area) ECG… q STE in a. Vr and > 2. 5 mm STE in V 1 q ST depression in V 5 q STE in V 3 R q ST depression in a. VL (Highly specific)
 – Proximal to D 1")
First septal branch not included (dominance of Lateral area) – Proximal to D 1
 ECG… q ST depression in")
First septal branch not included (dominance of Lateral area) ECG… q ST depression in Lead III > Lead II q ST elevation lead AVL & lead 1

ECG criteria to identify site of occlusion in the LAD q Engelen et al q J Am Coll Cardiol. 1999; 34: 389 -395

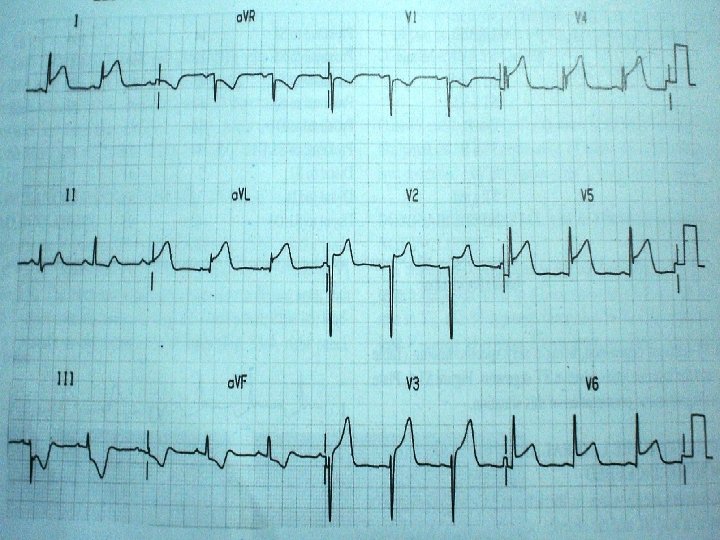
Inferoposterior wall MI
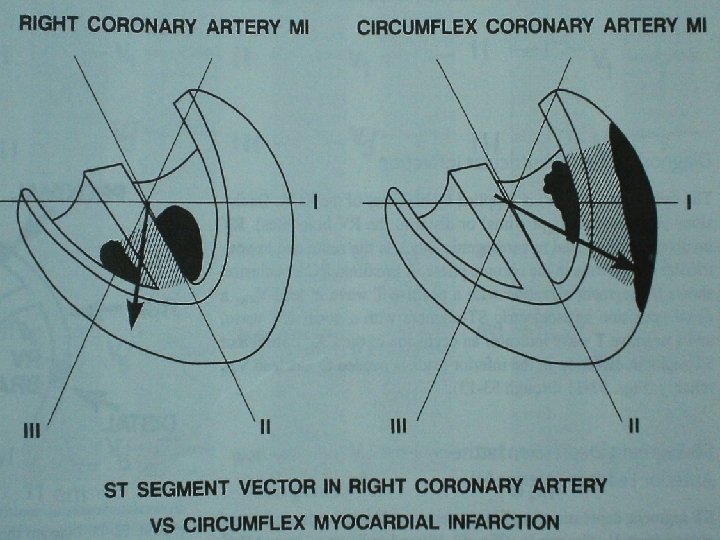

Occlusion of the RCA q q ST-segment elevation in III > II ST-segment depression in I and a. VL - a. VL > I Herz I, Assali AR et al q q q Am J Cardiol 1997; 80: 1343 -1345 ST depression in the precordial leads is smaller than ST elevation in inferior leads When occlusion is proximal to RV branches ST elevation in V 1 > V 3 V 4 LAD occlusion ST elevation in V 3 V 4 > V 1
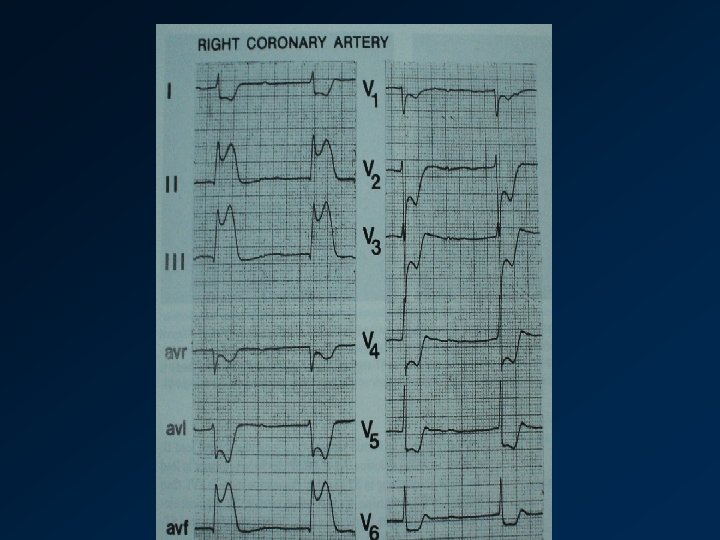

Dominance of RCA q q When RCA is dominant, ST-segment elevation is seen in V 5 and V 6 ST-segment elevation ≥ 2 mm - RCA very dominant Involvement of posterior wall PR prolongation. . AV nodal artery arises from dominant artery

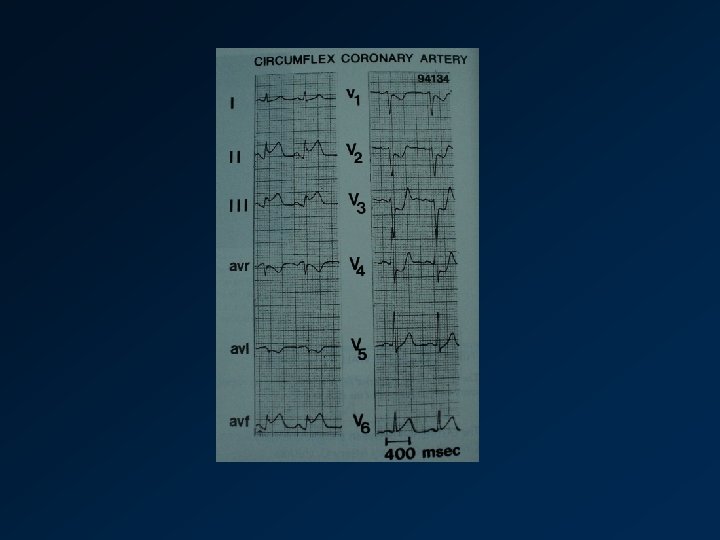
Occlusion of the LCX q q ST- elevation in II ≥ III ST elevation in I and a. VL. ST-segment elevation in II, III, and a. VF is usually smaller than the ST depression in right precordial leads When LCX is quite dominant - ST depression in a. VL, but very rarely in I

OM vs D 1 OCCLUSION 0 M q q ST elevation I, a. VL, and V 5− 6 Slight ST depression in V 1 -3 D 1 q q q ST elevation I, a. VL, and V 5− 6 ST-elevation in precordial leads ST-depression inferior leads.

RV infarction

RV infarction q STE >1 mm V 3 R and V 4 R q STE V 1 > V 2 q High degree AV block

Value of ST – T changes in V 4 R in acute infero posterior MI (RVMI) Braat SH, Gorgels APM, Bar FWHM, Wellens HJJ Am J Cardiol 1998; 62: 140 -142.
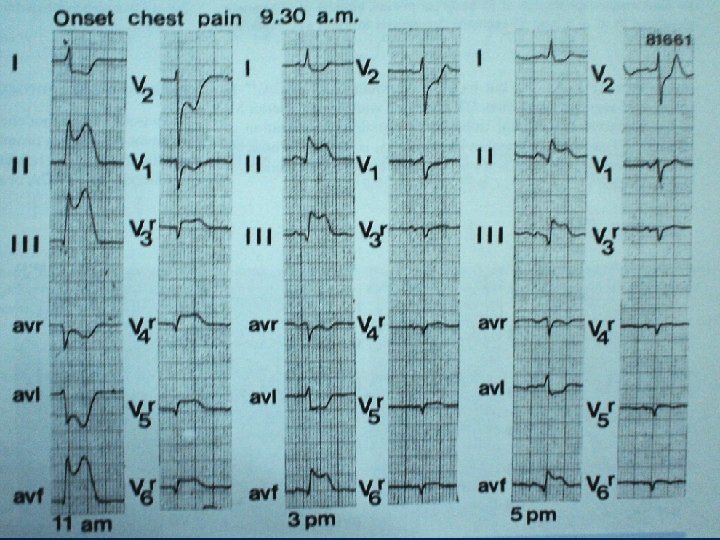

Isolated RVMI q q Minor changes in inferior leads, STE prominent in leads V 1 and V 2 , V 3 R and V 4 R Small or collaterally filled RCA Occlusion of an RV branch only

ST depression in anterior leads in IWMI q Implies posterior wall involvement q May extend from V 1 to V 6 and indicate larger MI q Maximal ST depression in V 4 – V 6 is seen more in three vessel disease and lower LVEF Birnbaum Y, . J Am Coll Cardiol 1996; 28: 313 -318 q Can occur both in RCA and Cx artery invt q Absence indicates RCA

ST depression in anterior leads q Isolated ST depression – Cx occlusion with a true PWMI or nonocclusive myocardial ischemia q Max ST depression in V 2 and V 3 is predictive of Cx q V 7 –V 9 shows ST elevation

True PWMI q ST depression in V 1, R/S >1, and upright T wave V 1 V 9

AV conduction disturbances q q AV nodal delay and block occurs with proximal RCA invt, frequently with RVMI Higher in-hospital morbidity & mortality

Sub AV conduction disturbances q RBBB with or without hemiblock during acute AWMI indicates proximal LAD q BBB or CHB indicates poor prognosis q LAHB in acute IWMI indicates additional LAD disease

LEFT MAIN STEM OCCLUSION OR TRIPLE VESSEL DISEASE q q q Acute LMCA occlusion rare but causes serious hemodynamic deterioration More commonly, subtotal occlusion occurs with collaterals filling from RCA presents as Unstable angina ECG of subtotal occlusion similar to triple vessel disease

LEFT MAIN STEM OCCLUSION OR TRIPLE VESSEL DISEASE q Marked downsloping ST depression in I, II, and V 4 – V 6 and STE in a. VR q a. VR STE occurred more in LMCA than in LAD q V 1 STE was less in LMCA than LAD q High mortality rate in those with higher STE in Avr Yamaji H et al J Am Coll Cardiol 2001; 38: 1348 -1354

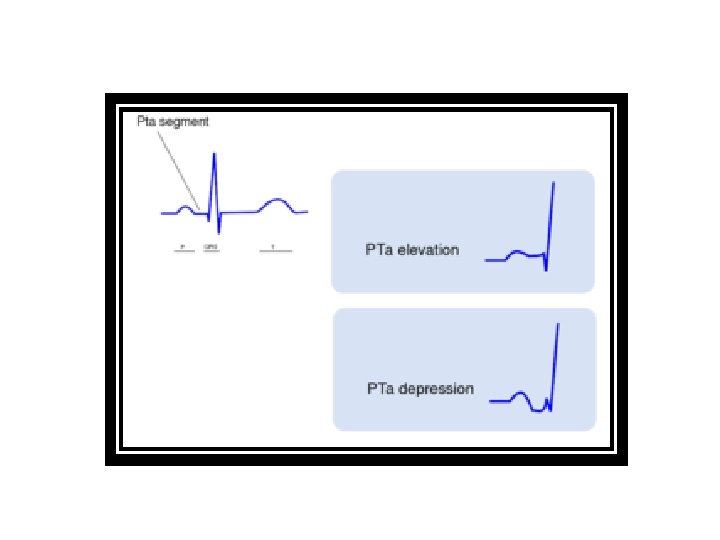
Atrial infarction q q Signs of atrial MI are seen in PTa segment elevation occurs in I, III, V 5 or V 6 or a depression in precordial leads q Occurs in 10 % of inferoposterior MI q Isolated occurrence is rare q Proximal RCA or Cx

RCA vs LCX

Limitations q q Assessment of the site of occlusion of coronary vessel by ECG is most reliable in case of 1 st MI Impaired – Multivessel disease – Collateral circulation – When ventricular activation is prolonged as in • • LVH Preexistent LBBB Preexcitation Paced rhythm

REFERENCE q q Bayes de Luna, Antman - The 12 lead ECG in STEMI Hein J J Wellens, Anton P M Gorgels, Pieter A Doevendans: The ECG in Acute Myocardial Infarction and Unstable angina – diagnosis and risk stratification Y. Birnbaum Bj Drew – Ecg in STEMI - correlation with coronary anatomy and prognosis YAMAJI H - Prediction of acute left main coronary artery obstruction by 12 -lead electrocardiography. ST segment elevation in lead a. VR with less ST segment elevation in lead V(1)
- Slides: 55