Liver Pathologies Dr S Nishan Silva MBBS Outline
")
Liver Pathologies Dr. S. Nishan Silva ( MBBS )

Outline • • Normal liver – Structure and function Hepatitis Cirrhosis Cancer Hepatic Encephalopathy Alcoholic Liver Disease Fatty Liver Disease

Functions of the Liver: A Brief Overview • Largest organ in body, integral to most metabolic functions of body, performing over 500 tasks • Only 10 -20% of functioning liver is required to sustain life

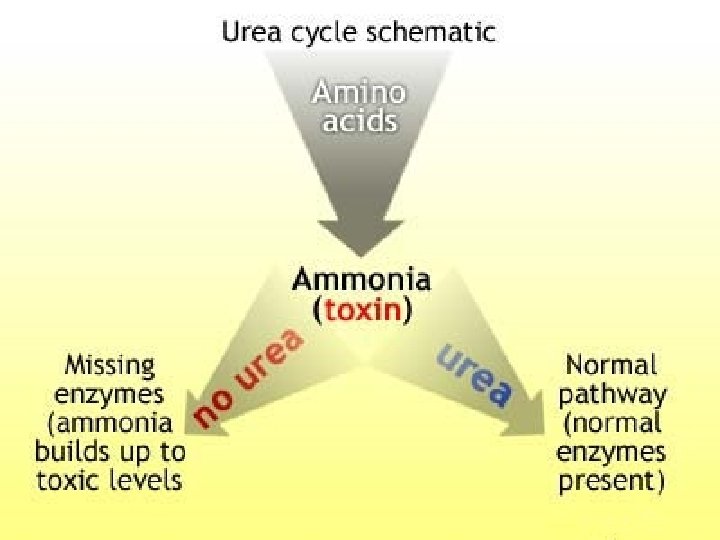
Functions of the Liver • Main functions include: – – – Metabolism of CHO, protein, fat Storage/activation vitamins and minerals Formation/excretion of bile Steroid metabolism, detoxifier of drugs/alcohol Action as (bacteria) filter and fluid chamber Conversion of ammonia to urea • Gastrointestinal tract significant source of ammonia • Generated from ingested protein substances that are deaminated by colonic bacteria • Ammonia enters circulation via portal vein • Converted to urea by liver for excretion

Classifications Liver Diseases • Duration w. Viral hepatitis A, B, C, D, E (and G) – Acute vs Chronic w. Fulminant hepatitis • Pathophysiology – Hepatocellular vs Cholestasic w. Alcoholic liver disease • Etiology w. Non-alcoholic liver disease – Viral – Alcohol w. Cholestatic liver disease – Toxin w. Hepatocellular carcinoma – Autoimmune • Stage/Severity w. Inherited disorders – End Stage Liver Disease (ESLD) – Cirrhosis
 • Encephalopathy within weeks of symptom")
Liver Diseases • Fulminant Hepatic Failure (“Shocked Liver”) • Encephalopathy within weeks of symptom • Multiple causes (ie, drug toxicity, hepatitis) • Malnutrition often not major issue • Chronic Hepatic Failure (“Subfulminant" Hepatic Failure) – At least 6 -month course of hepatitis – unresolving hepatic inflammation – Multiple causes: autoimmune, viral, metabolic, toxic
 – chronic cirrhosis due")
Liver Diseases Cholestatic Liver Diseases • Primary biliary cirrhosis (PBC) – chronic cirrhosis due to obstruction of the small intrahepatic bile ducts – 90% of patients are women – Nutritional complications • Osteopenia, hypercholesterolemia, fat-soluble vitamin deficiencies • Sclerosing cholangitis – Fibrosing inflammation of segments of extrahepatic bile ducts, – Nutritional complications • Inflammatory bowel disease, fat soluble vitamin deficiencies, hepatic osteodystrophy (steatorrhea)

Inherited Liver Disorders • Hemochromatosis • Wilson’s disease • α 1 -antitrypsin deficiency

Common Laboratory Tests Used to Test for Liver Function • Hepatic excretion —Total serum bilirubin, urine bilirubin • Cholestasis tests —Serum alkaline phosphatase • Hepatic enzymes —ALT, AST

Common Laboratory Tests Used to Test for Liver Function—cont’d • Serum proteins —PT, PTT, serum albumin • Markers of specific liver diseases —Serum ferritin, ceruloplasmin • Specific tests for viral hepatitis —Ig. M anti-HAV, anti-HBS, HCV-RNA

Discussion • • • 1. What are liver function tests? 2. What are liver enzymes? 3. What do each tell you? 4. Tests in liver cell damage 5. Tests in billiary obstruction

Hepatitis • Inflammation of the liver. • Caused by virus, bacteria, toxins, obstruction, parasites, or chemicals. • Viral hepatitis: caused by viruses A, B, C, D, or E; may have up to 10 more viruses.

Common Symptoms ØJaundice ØDark urine ØAnorexia ØFatigue ØHeadache ØNausea ØVomiting ØHepatomegaly ØSplenomegaly ØBilirubin, alkaline phosphate, and serum AST are all elevated.


Hepatitis A Virus Hepatitis A: §Highly contagious. §Resolves within weeks. §Does not become chronic. § 80% of cases in children remain asymptomatic. §In adults, 1/3 of cases develop jaundice.
 ØSewage No special treatment…occasionally hospitalized. Rarely")
Hep A Contamination: ØDrinking water ØFood (especially seafood) ØSewage No special treatment…occasionally hospitalized. Rarely get acute liver failure. (Never Cirrhosis)

Hepatitis B Virus Transmitted through • Blood or blood-derived fluids • Improperly sterilized medical instruments, dental drills • Tattooing needles • Other skin-puncturing instruments that has comes in contact in contaminated blood. • Can be acute or chronic
 • Exposed to blood or bodily fluids from an infected persons.")
Hepatitis C (HCV) • Exposed to blood or bodily fluids from an infected persons. • Sharing needles • Hemodialysis patients, infants born to infected mothers • Cannot be prevented by vaccination.

Fulminant Hepatitis • Syndrome in which severe liver dysfunction is accompanied by hepatic encephalopathy

Cirrhosis • Final, common endstage for a variety of chronic liver diseases

Chronic Hepatitis • At least 6 -month course of hepatitis or biochemical and clinical evidence of liver disease with confirmatory biopsy findings of unresolving hepatic inflammation

Symptoms - Cirrhosis §Asymptomatic §Portal hypertension §Bleeding from esophageal varices §Elevated bilirubin and hepatocellular enzymes §Weight loss §Increased energy expenditure

• Causes portal hypertension


Alcoholic Liver Diseases • Alcoholic Liver Disease, Alcoholic hepatitis, and Cirrhosis – Diseases resulting from excessive alcohol ingestion characterized by fatty liver (hepatic steatosis), hepatitis, or cirrhosis (fibrous tissue) – Prognosis depends on degree of abstinence and degree of complications – Malnutrition often an issue in these patients – Most common liver disease in US

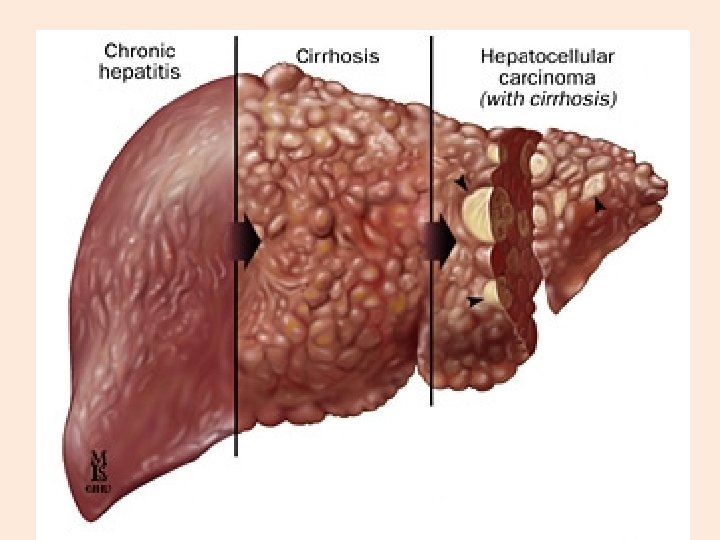
Progression of Liver Diseases

Normal Liver vs. Damaged Liver


Normal Liver

Alcoholic Fatty Liver

Cirrhotic Liver

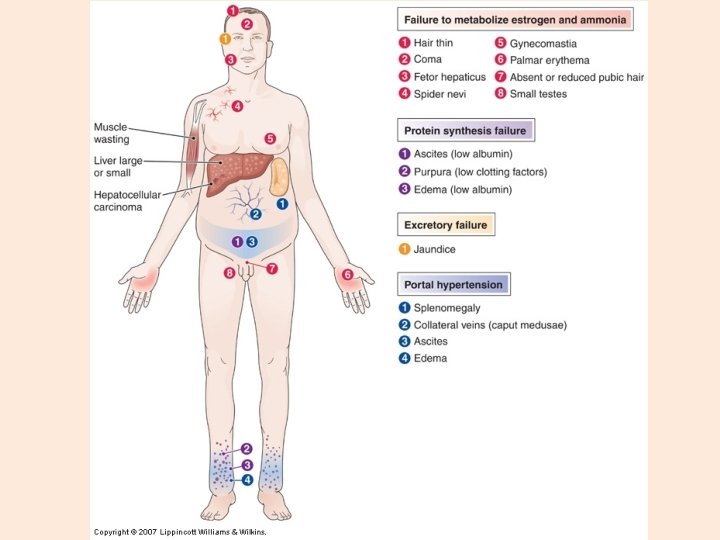
Clinical Manifestations of Cirrhosis


What is Hepatic Encephalopathy? • Broadly defined – All neurological and psychological symptoms in patients with liver disease that cannot be explained by presence of other pathologies • Brain and nervous system damage secondary to severe liver dysfunction (most often chronic disease) resulting from failure of liver to remove toxins • Multifactorial pathogenesis with exact cause unknown • Symptoms vary from nearly undetectable, to coma with decerebration – Characterized by various neurologic symptoms • Cognitive impairment • Neuromuscular disturbance • Altered consciousness • Reversible syndrome

Clinical Manifestations of HE Cerebral edema Brain herniation Progressive, irreversible coma Permanent neurologic losses (movement, sensation, or mental state) • Increased risk of: • • – – Sepsis Respiratory failure Cardiovascular collapse Kidney Failure

Clinical Manifestations of Cirrhosis

Precipitants of Hepatic Encephalopathy Drugs • Benzodiazepines • Narcotics • Alcohol Dehydration • Vomiting • Diarrhea • Hemorrhage • Diuretics Portosystemic Shunting • surgical Increased Ammonia Production, Absorption or Entry Into the Brain • Excess Dietary Intake of Protein • GI Bleeding • Infection • Constipation Primary Hepatocellular Carcinoma

Fatty Liver • 1 st sign of alcohol injury/ or not • aka steatosis • Can be 2 -3 X its size, yellow, greasy • Usually asymptomatic • May have elevated enzymes • Histologically, see Councilman bodies, Mallory bodies
 Steatosis: defined as a")
Non-alcoholic fatty liver disease Wide spectrum of liver damage: a) Steatosis: defined as a liver that contains 540% of the liver’s weight in triglycerides. § Hepatomegaly § Can be reversible § May still cause liver damage
 Non-alcoholic steatohepatitis (NASH): § Resembling alcoholic hepatitis, but not due to alcohol §")
b) Non-alcoholic steatohepatitis (NASH): § Resembling alcoholic hepatitis, but not due to alcohol § Overweight women § Associated with insulin resistance* § Very common, mild § May advance to cirrhosis and end-stage liver disease
 in free fatty acids of the stores in the liver,")
Steatosis occurs when: 1) in free fatty acids of the stores in the liver, 2) in liver synthesis of fatty acids, 3) in -oxidation of free fatty acids because of mitochondrial damage, 4) triglycerides production from fatty acids in the liver, 5) triglyceride removal from the liver.

Primary Biliary Cirrhosis • Autoimmune disease • Usually have another autoimmune disease • Evolves from inflammatory destruction of intrahepatic bile ducts • Early on see accumulation of lymphocytes around bile ducts • Death due to hepatic failure & portal HTN

Wilson Disease • Autosomal recessive disorder • Toxic accumulation of copper mainly in brain & liver • Copper absorbed in GI tract & excreted in bile – albumin transports to liver – bound to ceruloplasmin then secreted – if biliary excretion decreases, accumulates in liver & brain • Manifests as behavioral oddities, psychosis, tremors, abnormal gait • Diagnosis confirmed by liver biopsy • Early diagnosis critical • Chelation therapy

Metastatic Carcinoma • Most common neoplasm in the liver • Usually from colon, lung, breast

Hepatocellular Carcinoma • • Usually related to HBV & HCV Hematogenous metastases are common High levels of alpha fetoprotein Prognosis is grim

Cholelithiasis • • Gallstones in the gallbladder or biliary tree Form in gallbladder Usually have multiple stones About 1 million new cases/yr in US – 50% require surgery

• Cholesterol gallstones • 80% of cases • Bile saturated with cholesterol • Conditions associated with their development – age & gender – weight – ethnic, hereditary, & geographic factors – drugs – acquired conditions

• • Pigment gallstones 20% of cases Form in gallbladder & in biliary tree Composed of bilirubin & bile substances other than cholesterol

Acute Cholecystitis • Most common major complication of gallstones – 90% associated with obstruction of the neck • Gallbladder is enlarged, tense, & inflamed • Persistent rather mild RUQ pain to very severe pain

Chronic Cholecystitis • Do not have to have a history of acute attacks • Almost always associated with gallstones although obstruction not necessary • Mild to moderate RUQ pain • Nausea/vomiting • Intolerance of fatty foods

Obstruction of the Extrahepatic Bile Ducts
 • Definition: Hyperbilirubinemia refers to an excessive level of accumulated bilirubin")
Neonatal Jaundice (Hyperbilirubinemia) • Definition: Hyperbilirubinemia refers to an excessive level of accumulated bilirubin in the blood and is characterized by jaundice, a yellowish discoloration of the skin, sclerae, mucous membranes and nails. • Unconjugated bilirubin = Indirect bilirubin. • Conjugated bilirubin = Direct bilirubin. NJ - 55

NJ - 56
- Slides: 56