LIVER LESION LIVER EMBRYOLOGY It starts as a

LIVER LESION

LIVER EMBRYOLOGY • It starts as a hepatic duct/diverticulum • The hepatic duct arises at the ventral aspect and rotates 90 degrees clockwise. • The diverticulum divides into: 1. Cranial part>>>> gives rise to CBD, right and left hepatic duct & the liver. 2. Caudal part (smaller)>>>>gives rise to the cystic duct and gallbladder

LIVER ANATOMY • It is the largest abdominal organ 1500 g and receives 1500 ml of blood per minute. • ribs & cc’s (6 -10 on R, 6 & 7 on L) • Two lobes Cantle’s line • Two surfaces : - Diaphragmatic surface ‘bare area’ of the liver - Visceral surface With the exception of the fossa of the gallbladder and porta hepatis, it is covered with peritoneum. • epiploic foramen

LIVER ANATOMY • Protected by rib cage • Glisson’s capsule • 8 ligaments : ligament Coronary ligament : anterior and posterior fold Triangular ligament : right and left Falciform ligament : Sickle-shaped Ligamentum teres Ligamentum venosum Lesser omentum : hepatogastric ligament, hepatoduodenal
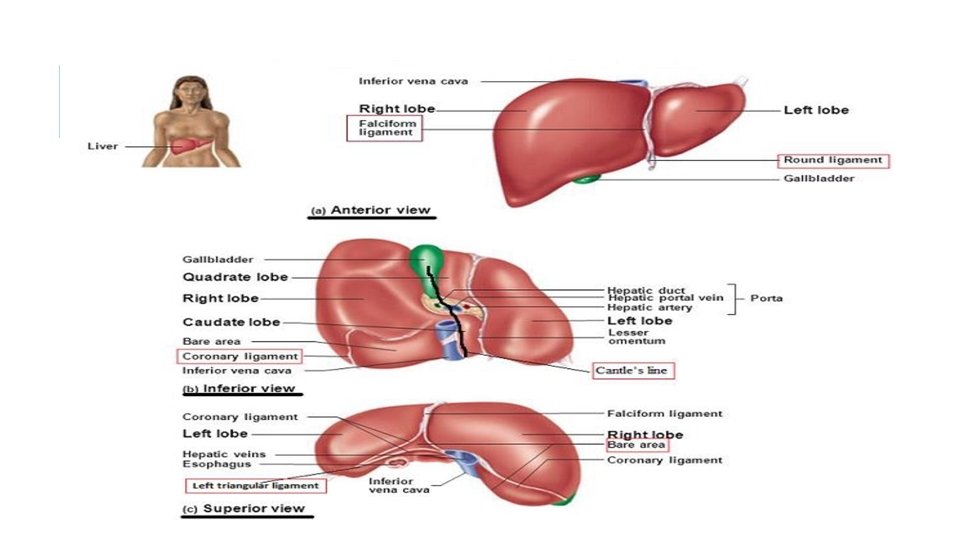

LIVER ANATOMY • 8 segments • Clockwise starting from segment 1 • French system. • Note that: segment 1 is the caudate lobe and (lower part of 4) is the quadrate lobe.

LIVER ANATOMY Hepatic artery 25% Dual supply : Portal vein 75% 72% of the Oxygen • venous drainage by the right, middle and left hepatic veins • Portosystemic anastomosis

PHYSIOLOGICAL FUNCTIONS § Production of : plasma protiens and coagulation factors. § Fat soluble vitamins metabolism § storage of : protiens(A. A), glucose(glycogen), fat(cholestrol) § Detoxification
 water Bile pigments")
BILIRUBIN METABOLISM • Bile: 800 ml per day (around I litre) water Bile pigments Bile salts Phospholipids (Lecithin) Cholesterol • Enterohepatic circulation
![JAUNDICE §Jaundice is clinically detected when Billirubin [>2. 5 -3 g/d. L. ] §Causes](http://slidetodoc.com/presentation_image_h2/ff7a537f185ef8d2aefefef2f4e3f04c/image-10.jpg "JAUNDICE §Jaundice is clinically detected when Billirubin [>2. 5 -3 g/d. L. ] §Causes")
JAUNDICE §Jaundice is clinically detected when Billirubin [>2. 5 -3 g/d. L. ] §Causes : • Overproduction by reticuloendothelial system. • Failure of conjugation or excretion. • Obstruction of biliary excretion into intestines.
 -hemolysis, multiple blood transfusions. -increased")
CLASSIFICATION OF JAUNDICE q. Prehepatic jaundice: serum haptoglobin. ) -hemolysis, multiple blood transfusions. -increased plasma unconjugated bilirubin( indirect LDH. q intrahepatic : It reflects liver dysfunction ( alkaline phosphatase, AST/ALT) Dubin-Johnson syndrome conjugated Gilbert syndrome. Criglar-Najjar syndrome. Viral hepatitis. Alcohol abuse. unconjugated cirrhosis. Medications: erythromycin/INH/phenytoin/valproate

CLASSIFICATION OF JAUNDICE Posthepatic : ALT. conjugated bilirubin - alkaline phosphatase & GGT. - ±AST, extrinsic or intrinsic obstruction of the biliary tree. ➢ Clinical presentation: 1. jaundice 2. pale color stool (due to absence of fecal bilirubin) 3. Dark urine ( conjugated bilirubin) 4. Itching. ➢ Diagnostic test of choice is ultrasound.

IMAGING - USS - CT - MRI - PET - Angiography

HYDATID DISEASE OF THE LIVER §It is a parasite disease of dog tape worm (Echinococcus) §affects humans in 2 forms depending on the larval stage: I. Cystic Echinococcus : most common caused by Echinococcus granulosus II. Alveolar Echinococcus : caused by Echinococcus multilocularis §The disease affects both humans and animals like: dogs, pigs, camels, sheep, rodents, and horses

LIFE CYCLE
 intermediate host is the sheep (also pigs, horses,")
• The major (most common) intermediate host is the sheep (also pigs, horses, and camels). • The major definitive host is the DOG (also foxes, and wolves) • Infection of the intermediate host occurs after the ingestion of food contaminated with eggs containing embryos (onchospheres) passed from feces of the definitive host. • Humans are infected via 2 ways: 1) direct contact with dogs 2) eating products contaminated by the feces of the definitive host • Humans are accidental intermediate host.
 in 70% of")
HYDATID DISEASE OF THE LIVER I. The liver is affected (diseased) in 70% of the cases while the lungs are affected in 30% of the cases but it can present any where. II. The Right lobe of the liver is mostly affected.

COMPONENTS OF THE CYST §The cyst has got 3 layers covering it from outside to inside➔ I. Outer adventitial layer (pseudocyst) : fibrous tissue due to reaction of the liver to the parasite. (coming from the host) II. 2 inner layers coming from the parasite: �Outer laminated membrane (ectocyst). �Inner germinal epithelium (endocyst). • The cavity is filled with Hydatid fluid (if it reach the tissue may cause anaphylactic shock ) and scolices ( which are infective.

SIGNS AND SYMPTOMS § usually asymptomatic the cyst remain uncomplicated §symptoms related to the pressure or mass : 1. RUQ pain: most common symptom. 2. Liver enlargement or palpable mass 3. Jaundice and pressure symptoms. 4. Sometimes the cyst ruptures or leaks some of its contents which may cause anaphylactic reactions which can be fatal or subclinical manifestations.
")
DIAGNOSIS: q. Eosinophilia : positive in 30% of patient. q. LFT q. ELISA (Weinburg) : (enzyme linked immunosorbent assay) positive in 80% of patient. q. Casoni (complement fixation test) q. Eosinophilia 30%

IMAGING Plain X ray: Ultra sound : cyst Eggshell appearance in calcified cyst Hydatid sand sign ( scolices appear as sand) CT scan : Determines size, location, number, and presence of intrahepatic lesions. MRI

IMAGING Plain X ray: CT scan : if it chronic will become calcified signet ring sign

TREATMENT: §Albendazole §Mebendazole § Indications of medical treatement: �Inoperable or unfit patient. �patients with multiple cysts in more than 2 organs �Multiple small liver cyst or cysts deep in the liver. �Peritoneal cyst. �Patients following incomplete surgery or relapses

TREATMENT: qsugery: the mainstay of treatment q. Inform the anesthesiologist it’s a hydatid disease ( anaphylaxis risk) q. Open or laparoscopic surgery q. Isolate the area q. Injecting scolicidal solutions into the hydatid cyst and packing the operative field with sponges soaked in scolicidal agents : hypertonic saline, hydrogen peroxide, 95% ethyl alcohol, polyvinylpirrolidoneiodine qpericystectomy. / Marsupialization / capitonnage.
")
LIVER CIRRHOSIS Any liver injury to liver (chemical or physical or any thing ) start in fibrosis end with cirrhosis so it the final sequela of chronic hepatic insult Gross morphology two type : Micro nodular Macro nodular important in physical examination to mention 1 - how its far from costal margin 2 - the edge is regular or irregular 3 - the surface soft or nodular 4 - liver to check its normal or enlarged or shrunk-ed

ETIOLOGY:

PORTAL HYPERTENSION: §sustained elevation of venous portal pressure more than 10 mm. Hg (15 -20 mm. Hg ) §Normal pressure 5 -10 mm. Hg §There are 6 potential routes of portal –systemic collateral blood flow (ares of communication):

Region Name of clinical condition Portal circulation Systemic circulation Esophageal varices Esophageal branch of left gastric vein Esophageal branches of azygos vein Rectal varices Superior rectal vein Middle rectal veins and inferior rectal veins Paraumbilical Caput medusae Paraumbilical veins Superficial epigastric vein Splenic vein Renal vein, suprarenal vein, paravertebral vein, and gonadal vein Right colic vein, middle colic vein, left colic vein Retroperitoneal veins of Retzius Hepatic pseudolesions[5] Perihepatic veins of Sappey Superior epigastric vein Patent ductus Left branch of portal Splenorenal shunt[3] Retroperitoneal (no clinical Intrahepatic name)[4] Inferior vena cava
 Splenic vein thrombosis Splenomegaly Splenic A-V fistula Intrahepatic")
ETIOLOGY: 1. Presinusoidal Extrahepatic : ) Splenic vein thrombosis Splenomegaly Splenic A-V fistula Intrahepatic : Schistosomiasis (Egypt Congenital hepatic fibrosis Idiopathic portal fibrosis Myeloproliferative disorders scardiosis

ETIOLOGY… 2. Sinusoidal Posthepatic 3. Post sinusoidal Intrahepatic Budd Chiari Cardiac cirrhosis IVC web Congestive Hepatopathy Primary Thrombosis Secondary Compresion

SIGNS & SYMPTOMS §Splenomegaly §esophageal varice §Caput medusa §Hemorrhoids §spider angioma, palmer erythema §Ascitis §asteraxis (hepatic flap) §fetor hepaticus §Jaundice §confusion and drowsiness

SIGNS & SYMPTOMS… qesophageal varices : q 30% of patients with compensated cirrhosis q 60% of patients with decompensated cirrhosis (development of jaundice, ascites, variceal hemorrhage, or hepatic encephalopathy ) q 1/3 of all patients with varices will experience variceal bleeding q. Each episode 20 -30% mortality if untreated q 70% of patients who survive the initial episode will experience recurrent haemorrhage within 2 years

ESOPHAGEAL VARICES

TREATEMENT OF ESOPHAGEAL VARICES : Management can be divided into : I. the active bleeding episode, II. the prevention of rebleeding, III. the prophylactic measures to prevent the first hemorrhage

INITIAL MANAGEMENT OF ACTIVE BLEEDING EPISODE I. Resuscitation: • IV line insertion ( 2 large bore cannulas) and IV fluid • Admission to ICU • Obtain blood for grouping and crossmatching (blood transfusion without over transfusion just until hemoglobin 9) • Correct coagulopathy: use fresh frozen plasma /Platelets/ coagulation factors • Antibiotics • Vasopressin • (octreotide) / IV II. Urgent endoscopy: both diagnostic and therapeutic (Variceal banding / Injection sclerotherapy)

If initial attempt failed Blackmore-Sengstaken tube for temporary blood bleeding control four ports 1 - for gastric aspiration 2 - for gastric balloon ( 500 ml) 3 - for esophageal balloon (200 ml) 4 - for esophageal aspiration prevent aspiration pneumonia do not leave it in situ for more than 24 -36 h (risk of perforation and necrosis)
: an expandable covered metal shunt Used when bleeding")
▪ TRANSJAGULAR INTRAHEPATIC PORTOCAVAL SHUNT (TIPS): an expandable covered metal shunt Used when bleeding cannot be stopped after 2 sessions of endoscopic therapy within 5 days. Advantages: it reduces the portal vein pressure by creating a total shunt and doesn’t have the risk of general anesthesia and surgery. Disadvantages: increased risk of portosystemic encephalopathy.
 Mesocaval stent Distal lienorenal")
▪ SURGICAL SHUNT: q. Shunting: Portocaval (increase incidence of encephalopathy) Mesocaval stent Distal lienorenal (Warren) (most used q. Non shunting: Sigiura ( bleeding uncontrollable) q. Liver transplant

LIVER ABSCESS mass filled with pus inside the liver Classified into : q • Pyogenic liver abscess: which is most often polymicrobial, accounts for 80% of hepatic abscess. q • Amoebic liver abscess: due to Entamoeba histolytica accounts for 10% of cases. q • Fungal abscess: most often due to Candida species, accounts for less than 10% of cases. q • Iatrogenic abscess: caused by medical interventions

PYOGENIC ABSCESS • Multiple organisms are usually isolated; however, they commonly include Escherichia coli, Staphylococcus aureus and anaerobes. Causes: v • biliary stasis then get infected most common cause(e. g. ascending cholangitis) v • Infection may spread through the portal vein from abdominal sepsis (e. g diverticulitis / appendicitis / it was the second most common but reduce with proper use of antibiotic and surgical care ). v • by direct spread from a contiguous organ. v • may follow blunt or penetrating injury.

PRESENTATION: • Classic triad of pyogenic liver abscess: Fever , Malaise & Right upper quadrant pain • Other symptoms : Anorexia and weight loss , Nausea and vomiting. • Respiratory symptoms may be present if the inflammation reached the overlying pleura resulting in pleural effusion • Physical examination: - Jaundice - Tender hepatomegaly - Intercostal tenderness - Epigastric tenderness - Decreased breath sounds in right lower lobe of the lung - Features of sepsis - The symptoms of pyogenic liver abscess are often non-specific (e. g. , fever, weight loss, etc. )
. o Plain")
INVESTIGATIONS: o Labs: CBC , LFT, ESR, CRP, Blood culture(+ive in 50%). o Plain radiographs : elevation of the diaphragm, pleural effusion and basal lobe collapse. o USS or CT is used to define the abscess (which is often irregular and thickwalled) and to facilitate percutaneous aspiration for culture. o ERCP may be useful if biliary obstruction is thought to be responsible.

MANAGEMENT : • Multible small abscesses : antibiotics alone • Solitary abscess : 1. percutaneous drainage. 2. open or laproscopic drainage. 3. Broad spectrum antibiotics can be used for up to 8 weeks (IV for 2 weeks followed by 6 weeks oral).

AMEBIC ABSCESS • Entamoeba histolytica enter mesenteric venules. • travel to the liver where they typically form one or more abscesses. • The right lobe of the liver is more commonly affected than the left lobe. • amebic abscess have characteristic chocolate appearance.
 to detect")
Investigation: CBC, LFT, Direct and indirect serological tests (CF, IHA and ELISA) to detect amoebic protein, stools examination for amebae trophozoites or cysts. Imaging: USS and CT: usually large, solitary, thin-walled, poorly defined abscess in the right lobe.

MANAGEMENT: o Empirical tx in areas where the problem is endemic. o metronidazole with chloroquine phosphate usually results in rapid resolution. o Needle aspiration if : -No clinical response within 72 hours abscess). -There was superinfection (treated as pyogenic -The abscess is large.

SCHISTOSOMIASIS § parasitic disease caused by blood flukes § exposure to infested water § Presentation: abdominal pain, diarrhea, bloody stool, hepatomegaly. § Dx: detection of parasite eggs in stool or serum antibodies. § Causes Perisinosoidal portal HT § Tx: Praziquantel Single dose 40 -70 mg/kg. Education Hygiene

ASCARIASES: Ascaris lumbricoides, roundworm. Retrograde locomotion into the bile ducts

TREATMENT: v. Piperazine citrate v. Albendazole v. Mebendazole v. ERCP

LIVER CYSTS: q Congenital. Benign cystadenoma Polycystic liver disease : look like a cluster of very large grapes q. Secondary (traumatic) Seromas Bilomas

LIVER CYSTS: choledochal cyst Caroli’s disease Biliary lithiasis 33%, Cholangitis, Biliary abscesses, Cholangiocarcinoma 7%

TUMORS OF THE LIVER q Most common liver Cancer is metastasis fromn the GI tract) q Most common primary malignant liver tumor is hepatocellular q Most common primary benign liver tumor is hemangioma

TUMORS OF THE LIVER

. HEMANGIOMA qbenign vascular tumor of the liver. q. Signs & symptoms: Asymptomatic in 85%/ RUQ pain/ mass/ Bruits. q. Complications: 1. Pain. 2. Congestive heart failure due to AV shunt. 3. Coagulopathy due to sequestration of platelets. 4. Kasabach-Merritt syndrome: hemangioma, thrombocytopenia, and consumption coagulopathy. q ➢ Diagnosis: 1. CT scan with IV contrast (hypoperfusd lesion)/ MRI /Ultra Sound q Note: biopsy shouldn’t be performed due to risk of hemorrhage with biopsy common in female (95% small and we just observe them and tell them to prevent trauma)

ADENOMA This tumor histologically consists of normal hepatocytes without bile duct or kuppfer cells ➢ Risk factors: 1. Female. 2. Birth control. 3. Anabolic steroids. 4. Glycogen storage disease. ➢ Signs & symptoms: 1. RUQ pain/ mass/fullness/Bleeding ➢ Complications: Rupture with bleeding. (important during pregnancy) Risk of hepatocellular carcinoma.

➢ Diagnosis: 1. CT. 2. Ultra Sound. 3. ±biopsy but role out hemangioma with tagged red blood cells scan first. ➢ If small➔ stop pills ➔ it may regress ➔ If didn’t regress➔ surgical resection is necessary. ➢ If large (>5 cm)/ bleeding/ painful/ rupture➔ surgical resection. ❖ Note: average age: 30 -35 years of age.
 AKA: HEPATOMA. The 5 th common malignancy 1. Viral hepatitis 2.")
HEPATOCELLULAR CARCINOMA (HCC) AKA: HEPATOMA. The 5 th common malignancy 1. Viral hepatitis 2. Alcoholic cirrhosis: 5% of patients with cirrhosis will develop. Most HCC. important 3. Aflatoxin (fungi toxin of Aspergillus Flavus). 4. α 1 –antitrypsin deficiency 5. Hemochromatosis. 6. Wilson 7. Anabolic steroids. 8. Glycogen storage disease. risk factors

SIGNS & SYMPTOMS: Dull RUQ pain / Hepatomegaly/ Abdominal mass/ Weight loss/ Paraneoplastic syndrome/ Signs of cirrhosis: portal hypertension/ Ascites/Jaundice. Investigation: 1. Tumor marker: Alpha-fetoprotein (AFP). (not specefic but must be done more than 5000 unit is significant ). 2. Ultra Sound. 3. CT. 4. Angiogram. 5. tissue biopsy with CT / Ultra Sound/ or laproscopic guidance : the most common way to diagnose HCC

MANAGEMENT q. Surgery. q. Raditherapy. q. Chrmotherapy. q. Liver transplant. q 5 year survival rate is less than 10%.
: in the small bile ducts")
CHOLANGIOCARCINOMA adenocarcinoma of the biliary tree q. Intrahepatic (Peripheral): in the small bile ducts within the liver q. Extrahepatic (central): hilar cholangiocarcinoma (Klatskin tumor). 50% distal cholangiocarcinoma. Risk factors : chronic parasitic infestation of the biliary tree choledochal cysts (caroli’s disease). Ulcerative colitis sclerosing cholangitis

PRESENTATION Jaundice pain hepatomegaly.

questions ?
- Slides: 62