Liver Gallbladder Exocrine Pancreas KNH 411 Pathophysiology of

Liver, Gallbladder, Exocrine Pancreas KNH 411


Pathophysiology of the Liver Alcoholism Chronic consumption of > 80 g of ethanol/day - 250 CCs= I cup, hard liquor 6 1. 5 oz. shots, or 1 liter wine per day, 6 12 oz. Beers per day Alcoholic liver disease (ALD) - fatty liver, hepatitis and cirrhosis fall into this category Dependency may be evident as tolerance or withdrawal Ethanol rapidly and completely absorbed even with malabsorption (2 to 10% leaves system from kidneys) Cannot be stored – oxidized - absorbed from GI tract

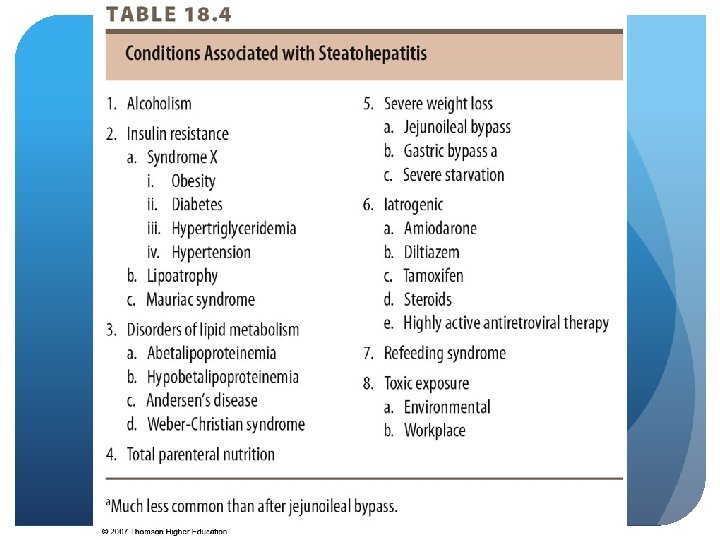
Pathophysiology of the Liver Fatty Liver – Etiology Liver increases in size and weight by 5% making it not possible to see lab values Steatohepatitis – inflammation in that area, related to ALD If alcohol not present – NASH NAFLD progresses to cirrhosis and hepatic carcinoma Strong association with obesity, diabetes, metabolic syndrome Most common type among adolescents

Pathophysiology of the Liver Malnutrition in the Alcoholic Malnutrition caused by displacement of nutrients** concern Maldigestion or malabsorption of nutrients d/t GI complications Vitamins ADE and K and macronutrients May need tube feeding or IV nutrition due to complications such as bloating, disorientation and anorexia

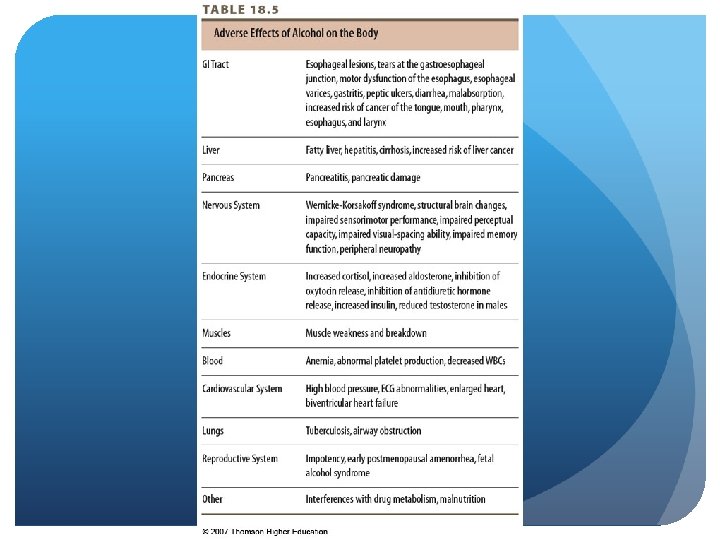
Pathophysiology of the Liver Malnutrition in the Alcoholic - GI Complications Esophagus – heartburn, reduced LES pressure, esophagitis, stricture, tears from vomiting Stomach - gastritis, duodenitis, atrophy of gastric mucosal barrier, hemorrage, PUD, pernicious anemia, stomach cancer - need to check B 12 status incase of lack of intrinsic factor and HCL

Pathophysiology of the Liver Malnutrition in the Alcoholic - GI Complications Intestine – structural and morphological changes, hemorrhagic lesions of villi tips, decreased motility, increased digestion time (relating to dumping syndrome), bacterial overgrowth (always adding alcohol and no nutrients)

Pathophysiology of the Liver Alcoholism - Nutrition Implications Hepatitis, cirrhosis Significant caloric contributions – obesity Irregular eating habits Decreased appetite – weight loss Kcal derived from ethanol 0. 8 X proof X ounces = kcal

Pathophysiology of the Liver Alcoholism – Malnutrition PEM: look at Poor dietary intake, malabsorption, hypercatabolic state, altered energy storage, biochemical changes (biochemical changes, total bilirubin, albumin status) Vitamin deficiency ADE and K Major cause of liver damage and resulting dysfunction

Pathophysiology of the Liver Alcoholism - vitamin and mineral deficiencies Folate- alcohol interferes with metabolism Thiamin- interferes with uptake and utilization Wet and dry beri Wernicke-Korsakoff syndrome- altered mental status if can’t feed themselves Low plasma pyridoxine- inadequate intake Vitamin C- deficient; 175 to 500 mg/day of ascorbic acid to replace what has been lost Vitamin D – impairs osteoblastic activity

Pathophysiology of the Liver Alcoholism - vitamin and mineral deficiencies Vitamin K - clotting factors, due to fat malabsorption and pancreatic insufficiency Vitamin A – night blindness Interaction between vitamin A and zinc Iron – altered response to infection Calcium – bone density and bone mass Potassium – hypokalemia due to poor intake because of diarrhea and vomiting, may need potassium in IV Recommend multivitamin 2 X RDA High Pro and calories

Pathophysiology of the Liver Alcoholism – nutritional effects Imbalanced diet and/or anorexia Maldigestion and malabsorption - Inflammation of the stomach, pancreas, and intestine cause this Increased catabolism of visceral protein and skeletal muscle Increased excretion of vitamins

© 2007 Thomson - Wadsworth

Pathophysiology of the Liver Hepatitis – inflammation of the liver caused by virus, bacteria, toxins, obstruction, parasites or drugs HAV – via oral-fecal route HBV – blood transfusions, blood-derived fluids, or improperly sterilized medical equipment HCV – exposure of blood or body fluids from infected person; no vaccine HDV, HEV

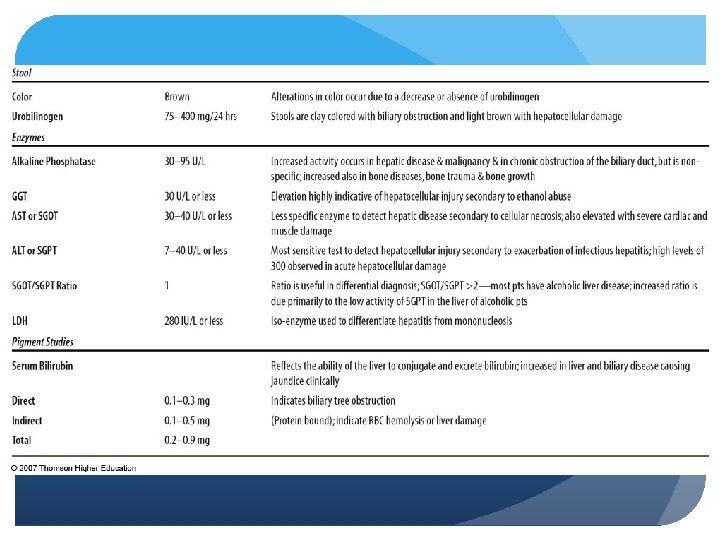
Pathophysiology of the Liver Hepatitis – clinical manifestations Jaundice, dark urine, anorexia, fatigue, headache, nausea, vomiting, fever Hepatomegaly and splenomegaly Bilirubin, alkaline phosphatase, serum AST elevated

Pathophysiology of the Liver Hepatitis – Nutrition Therapy Spare liver and provide nutrients for regeneration Adequate rest, fluids, good nutrition, avoidance of further damage - IV line will give vit. , minerals, dextrose, lipids Increase dietary intake 30 -35 kcal/kg body weight (≥ 3000 kcal) D 10 (glucose) can only be given in 10 to 12% peripheral vein Small, frequent meals May want 50% enterally, 50% IV

Pathophysiology of the Liver Hepatitis – Nutrition Therapy Adequate protein 1 -1. 2 g/kg body weight, . 8 average healthy person 30 -40% of kcal from fat May not be well tolerated Supplemental vitamin K- prothrombin time Potassium and sodium if vomiting and diarrhea

Pathophysiology of the Liver Alcoholic hepatitis - toxic liver injury associated with chronic ethanol consumption Increased susceptibility to infections - Usually come with pneumonia Fatigue, weakness, anorexia, fever, hepatomegaly - All show inadequate intake of calories

Pathophysiology of the Liver Alcoholic Hepatitis - Treatment/ Nutrition Therapy Abstention from alcohol Treatment of withdrawal symptoms - concern: delirium tremens Correction of nutritional deficiencies Multivitamin – B 12, folate, thiamin, pyridoxine, vitamins A & D Multimineral – zinc, magnesium, calcium, phosphorus Adequate kcal and protein is goal

Pathophysiology of the Liver Cirrhosis - chronic liver disease in which healthy tissue is replaced by scar tissue, blocking the flow of blood, resulting in loss of liver function Most common causes – chronic alcoholism and HCV Steatosis is first stage- fatty liver

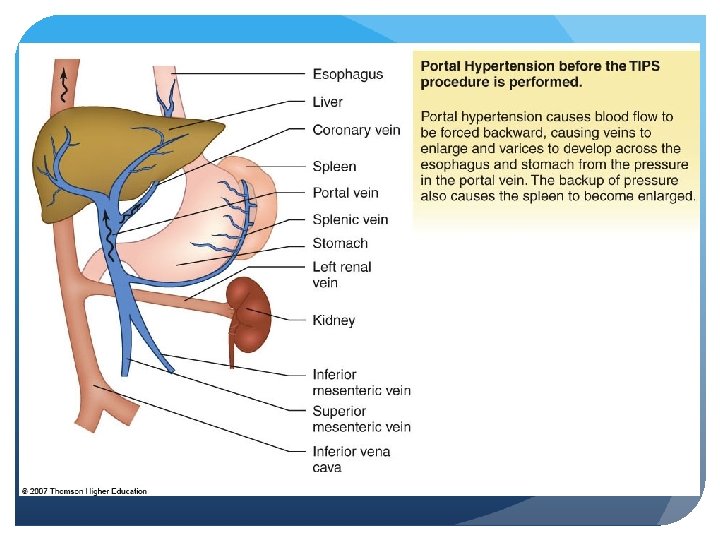
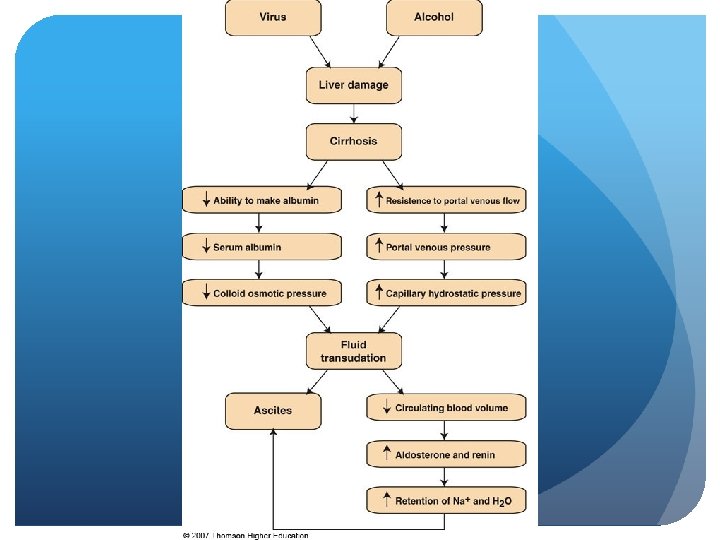
Pathophysiology of the Liver Cirrhosis – etiology Associated with alcoholism Scar tissue forms Conversion of fat to lipoprotein impaired Accumulation of fat in the liver Portal hypertension may develop (death of liver/compromised liver) Esophageal varices- streaks of bleeds in esophageal area Rupture with hemorrhage

Pathophysiology of the Liver Cirrhosis – clinical manifestations Enlarged liver from necrosis Ascites and edema- 1 to 2 L in abdominal area of excess fluid and protein, sodium, and potassium when fluid is removed) SGOT elevated, BSP clearing time reduced- compromised BP Vitamin deficiencies (vitamins A, D, B), depressed hgb, hct Jaundice, lack of appetite, delirium tremens Fever, gallstones, ulcers, GERD, gastritis, diarrhea - TPN if this case

Pathophysiology of the Liver Cirrhosis – complications Portal hypertension- abnormal pressure present in portal venous system Ascites- fluid buildup in abdominal cavity, protein potassium, and sodium are lost when removed Hepatic encephalopathy- cannot give enteral if aren’t aware of surroundings, tube feeding preferred or TPN

Pathophysiology of the Liver Cirrhosis – portal hypertension Always present with ascites Decrease in hepatic vascular bed; obstruction, increased resistance, arteriovenous anastomoses
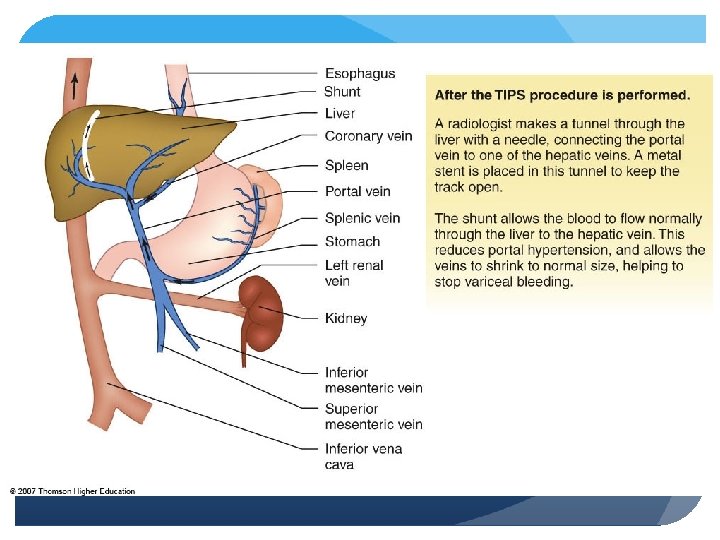

Pathophysiology of the Liver Cirrhosis – ascites Accumulation of fluid in peritoneal cavity; most common complication (1. 5 - 2 liters fluid taken off or about 1 g protein per 100 CCs) Hepatic fibrosis, reduced osmotic pressure, increased retention of sodium

Pathophysiology of the Liver Cirrhosis – ascites: nutrition therapy Encourage oral proteins/ supplements Restricting salt to 2 g/d – patients are hyponatremic Restricting fluid to 1500 cc (5 to 6 cups/day) Adequate kcal - 25 to 35 g calories/kilo Diuretics - lasics-potassium wasting so need to be replaced in IV - Promod: 4 g/T (carnation instant breakfast)
")
Pathophysiology of the Liver Cirrhosis – hepatic encephalopathy (end stages associated with liver failure) Syndrome of impaired mental status and abnormal neuromuscular function 2 types graded onto 4 clinical scales; Child-Pugh score The Glasgow coma scale: look at functions 3 -15, 3 worst “Flap” - asterixis
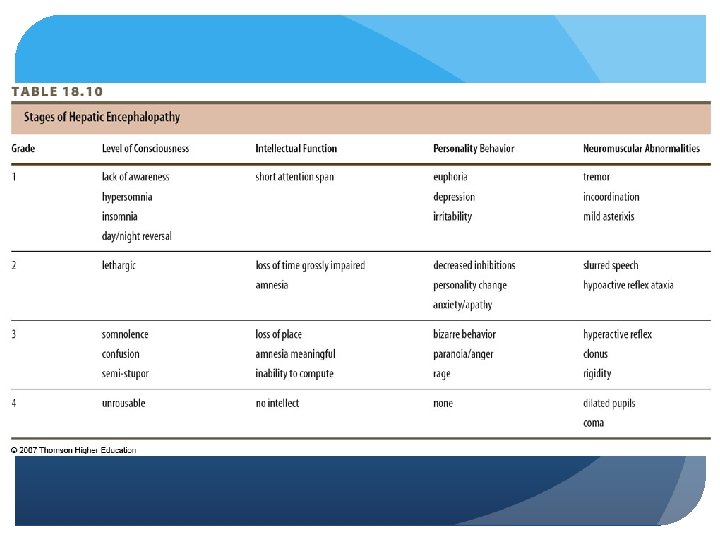

Pathophysiology of the Liver Cirrhosis – hepatic encephalopathy Pathogenesis unknown; inability to eliminate products toxic to brain 4 major hypotheses: Ammonia- high levels created are toxic to brain and generated through catabolism of liver Synergistic neurotoxin- created by bacteria with individual with liver failure False neurotransmitter- causes increase in phenylananine GABA benzodiazepine- levels toxic to brain

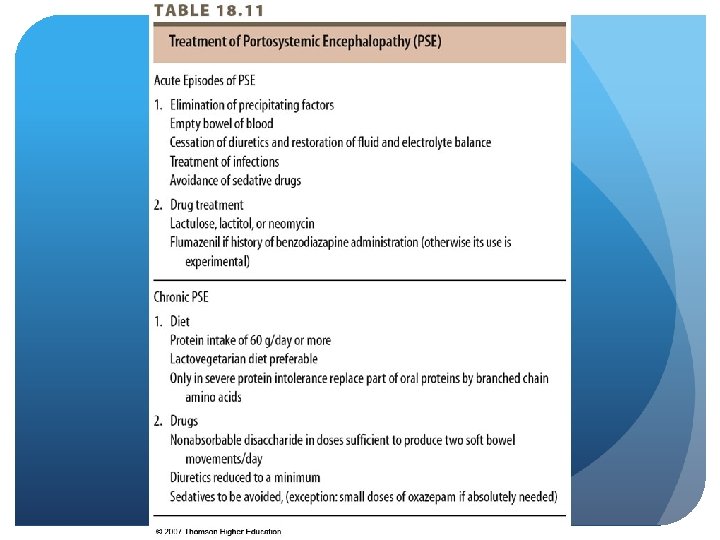
Pathophysiology of the Liver Cirrhosis – hepatic encephalopathy Treatment depends on type, extent of neurological damage, presence of precipitating factors Treatments Dietary protein restriction (minimum 50 g/d), plant sources, increased fiber, milk and cheese, BCAAs Monitor serum potassium level Correct hypoglycemia, vitamin deficiencies (increase dextrose in solution, B, D and E vitamins)

Pathophysiology of the Liver transplant – considered in cases where effects of disease have higher potential mortality than transplant With alcoholism - six months abstinence to qualify for transplant Psychological and nutritional evaluations Usually 1 year survival rate after transplant

Pathophysiology of the Liver Transplant – Nutrition Therapy Individualized Pretransplant Kcal 34 -45 kcal/kg; protein 1 -1. 5 g/kg Normalize macro- and micronutrients Normalize blood sugar, nitrogen balance (assess protein needs), relevant labs

Pathophysiology of the Liver Transplant – Nutrition Therapy Posttransplant Regualr diet – slightly lower kcal and pro. Other nutrients individualized based on immunosuppressant drug regimen May cause hyperglycemia (avoid simple sugars, cho=50 to 60% range), sodium retention (2, 000 to 4000 mg), potassium retention Provide DRI for vitamins 30 -35 kcals/kg 1 g pro/kg
 - inherited disorder of epithelial")
Pathophysiology of the Liver Cystic fibrosis-associated liver disease (CFALD) - inherited disorder of epithelial transport Mutated gene codes for defective protein 2 nd most common cause of death among CF patients Cl is prevented from leaving cell and water cannot exit Mucus thickens, cilia cannot function, bacteria collect on the cells infections

Pathophysiology of the Liver CF – Nutrition Therapy Counseling on risks associated with alcohol and herbal therapies Kcal needs increase 20 -40% May need MCT Do not restrict protein (unless encephalopathic) Assess status of fat-soluble vitamins every 6 mnths - MCT Pancreatic enzyme supplements with meals and supplements

Pathophysiology of the Liver CF – Nutrition Therapy Vitamin A - risk for night blindness and conjunctival xerosis – 24 X DRI, but avoid hypervitaminosis Vitamin E – protection of lungs from oxidative stress 15 -25 IU/d Vitamin D – 2 -4 µg/d. L/day - Don’t see w/ children because more access to outside Vitamin K – 2. 5 -10 mg/daily EFA supplementation (supplement PUFAs)

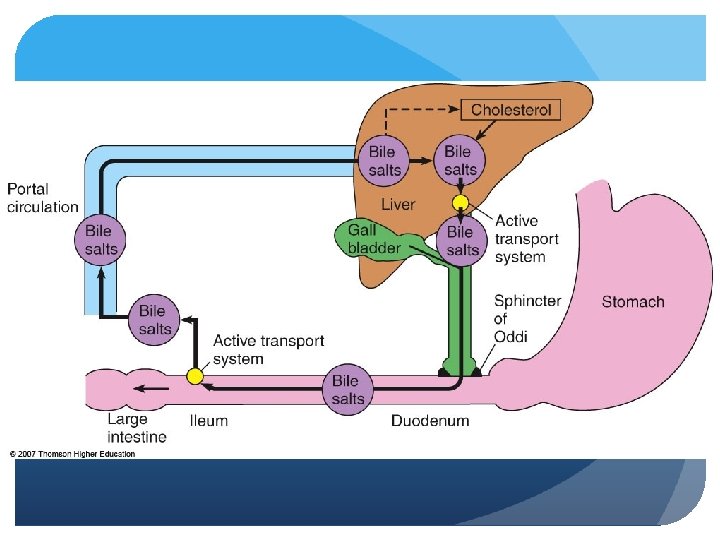
The Gallbladder Stores, concentrates and secretes bile Removal of water and electrolytes – increasing concentration Storage Control of delivery of bile salts to duodenum Main functions: excreting it in presence of food to help digest fat Complications: gallstones- will but on low-fat diet to relieve pressure
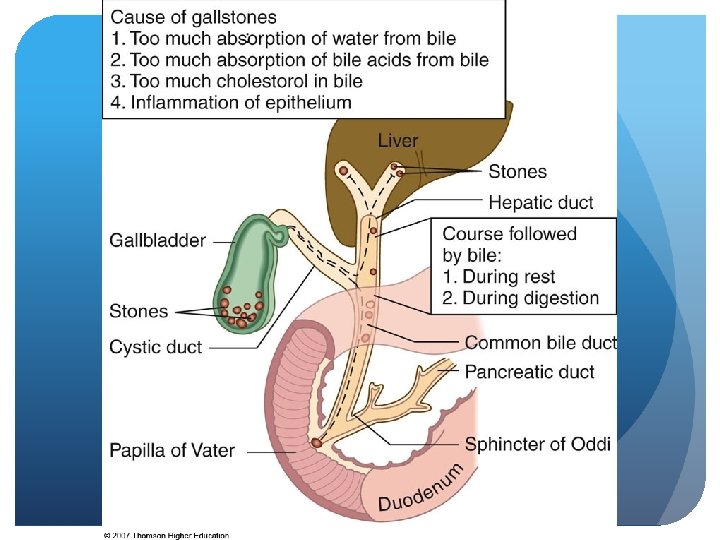

The Gallbladder Cholelithiasis – Nutrition Therapy Assess alcohol intake Increase complex CHO and insoluble fiber - Avoid hyperglycemia Assess vitamin C intake- inverse relationship w C levels and cholelithiasis ? Low-fat diet (if remove stones, can go back to a normal diet) Counsel on lifestyle habits- exercise Plain, simple foods best tolerated - Minimize sweets, increase fruits, veggies, whole grains, drink in moderation
 NPO and complete")
The Gallbladder Cholelithiasis – Nutrition Therapy Acute attack (keep gallbladder inactive) NPO and complete bowel rest Parenteral nutrition as needed (IV nutrition after few days) Advance as tolerated to liquids, low fat diet, skim milk and diary Limited amounts of fats and solid foods added Progress to regular diet
 Weight reduction")
The Gallbladder Cholelithiasis – Nutrition Therapy Chronic condition Low fat (25% kcal) Weight reduction (gradual) Adjust pro and CHO for weight Water-soluble forms of fat-soluble vitamins to alleviate concern with bile and processing fat soluble vitamins Quick weight loss may result in gallstones

The Gallbladder Cholelithiasis – Nutrition Therapy Postoperative Cholecystectomy - Absence of gallbladder Oral feedings resumed once bowel sounds return Advance as tolerated to regular diet Increased fiber to manage diarrhea Manage digestive symptoms: fatty food intolerances, heartburn, nausea
 - Bowel rest, decrease amt.")
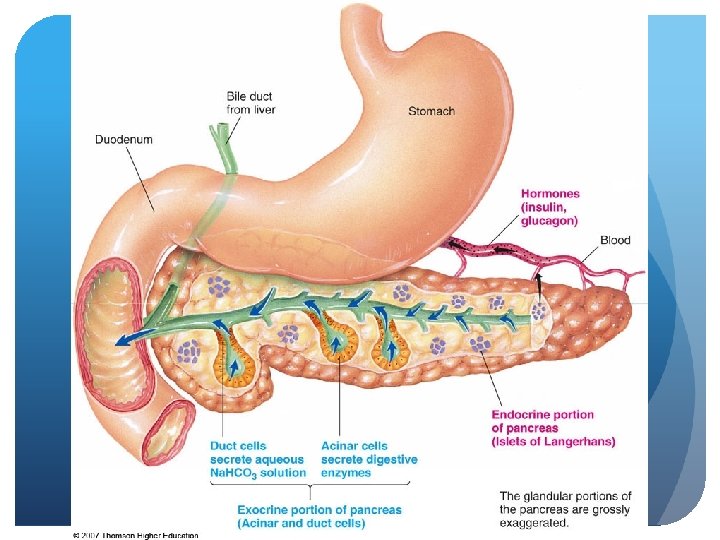
The Pancreas Pancreatitis - nutrition therapy (looking at exocrine) - Bowel rest, decrease amt. of nutrients it has to process Provide minimal stimulation of affected systems Severe attacks – oral feedings withheld Less severe - clear liquid diet, progress as tolerated; low fat Small, frequent meals divided into 6 feedings while decreasing amt. of fat intake

The Pancreas Pancreatitis - Nutrition Support for Acute Provide adequate kcal & protein, minimize nitrogen losses, manage imbalances (usually will be increased glucose and triglycerides- watch fat so tolerate IV lipids; Ca, Mg, ADEK deficiencies- supplement or address levels with PO intake) Protein needs increase 8% (~1. 5 kg/kilo), 20% increase calories - want 40 kcal/kg Enteral preferred method Maintain gut integrity Reduce septic and metabolic complications Less costly Goal is to preserve muscle mass

The Pancreas Pancreatitis - Nutrition Support for Acute Enteral support below ligament of Treitz via nasogastric tube (tissue connecting duodenum to diaphram) Nasogastric feed- nose to stomach Nasojejunum tube- nose to jejunum Initiate feeding 25 m. L/hour, advance to 25 kcal/kg over 24 -48 hrs. (25 CCs/hr) - 70% fats should be MCT Nearly fat-free elemental formulas Advance to oral diet when amylase and lipase decrease towards normal

The Pancreas Pancreatitis - Nutrition Support for Acute Parenteral – only considered in pts. for whom enteral access not possible or not tolerated - Gut rest Mixed fuel, volume increased slowly to 25 kcal/kg Intralipid less than 15 -30% of kcal, protein individualized

The Pancreas Pancreatitis - Insufficiency Frequent, small meals moderate to low in fat Pancreatic enzymes taken with food (treat steatorrhea- decreased absorption of fat) Alcohol, coffee, tea, spices, irritant condiments avoided MCT may be added Maintain weight Monitor fat and water-soluble vitamins Medical management of p. H Treat with insulin if indicated
- Slides: 60