Liver Biliary Pancreas Problems Introduction Liver is the

Liver, Biliary & Pancreas Problems

Introduction Liver is the largest organ of the body. n It’s a multifunctional organ plays important role in CHO, fat & protein metabolism. n

Functions of liver 1. 2. 3. 4. 5. 6. Protein metabolism Carbohydrate metabolism Lipid metabolism Mineral & vitamin metabolism Immunological functions Detoxification

Common Etiology 1. Dietary deficiencies: Protein deficiencies as in PEM High fat intake Diabetes, obesity 2. Infective agents: Viruses like type A, B, C, D, E cause hepatitis 3. Toxic agents: Alcohol Drugs and chemicals

Pathological changes in the liver Atrophy: Degeneration of hepatic cells n Fatty infiltration: Deposition of fat droplets in hepatic cells. Reversible but if severe or long lasting may be followed by necrosis or fibrosis. n Fibrosis: functional hepatic cells are replaced by connective tissue cells. n Necrosis: Death of hepatic cells n

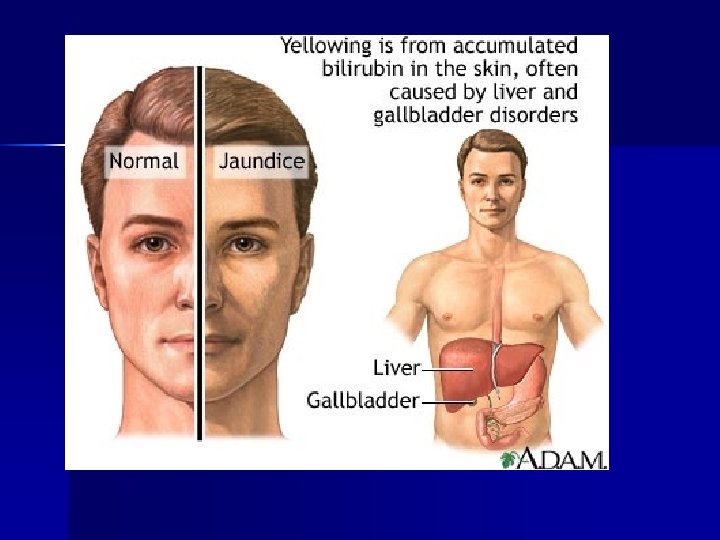
Jaundice A common symptom of all liver disease n Is a result of increased bilirubin level in blood. ( it is a breakdown product of RBC) Symptoms: n Yellow coloration of skin, conjunctiva & body tissues n


Types of jaundice 1. Hepatocellular jaundice: damage to hepatic cells interfering with uptake of bilirubin. 2. Prehepatic (hemolytic) jaundice: icreased bilirubin level in blood as a result of excessive destruction of RBC. n Common in inborn, neonatal jaundice n Congenital defects like sickle cell anemia, thalessaemia
 jaundice: obstruction of bile flow between liver")
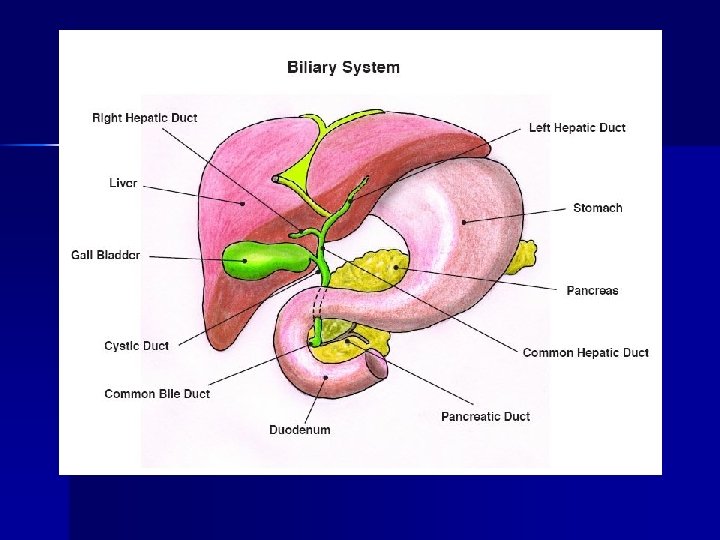
Types of jaundice 3. Post hepatic (obstructive) jaundice: obstruction of bile flow between liver & duodenum n patients suffering from gallstones or cancer of liver or pancreas

Other symptoms of liver disease n n n n n Lassitude Weakness Fatigue Fever Anorexia Weight loss Abdominal pain Flatulence Nausea Vomiting n n n Hepatomegaly Edema Ascites

Hepatitis Inflammation & degeneration of liver cells. Types: 1. Viral / infectious hepatitis 2. Drug induced n

Viral Hepatitis Also known as infectious hepatitis. n Inflammation & degeneration of liver cells. n More common, occur as infectious or serum hepatitis. Types: Infectious / type A: virus transmitted through fecal contamination of food & water. Serum hepatitis / Type B: transmitted only by parental routes through blood contaminated with virus or poor sterilized needles. n

Hepatitis A n n n Fecal-oral route, outbreaks caused by fecal contaminated food or drinking water. Crowded conditions, poor sanitation & hygiene, undeveloped countries, shellfish from contaminated water Most infectious 2 wks before s/s & 1 wk after s/s start.

Hepatitis B Percutaneous, permucosal, or perinatal exposure, sexually transmitted disease. n 100 X more infectious than HIV n Carrier state - antigen HBs. Ag for 6 -12 mo. n Immunity – antigen anti-HBs-Ag n

Hepatitis C Transmission- pericutaneous n At risk: IV drugs, bld transfusion, hemodialysis, tattooing, hi risk sexual behavior, organ transplants, health care workers n

Hepatitis D Delta virus n Transmission - percutaneous n Can turn mild or chronic hep. B into severe, chronic, progressive, active hepatitis & cirrhosis n

Hepatitis E Transmission – fecal-oral route, esp contaminated drinking water. n Occurs in developing countries, epidemics in India, Asia, Mexico, Africa. In US rarely, only after a person traveled. n

Hepatitis G Recently discovered. n Found in blood donors & transmitted by transfusion. n Not associated with chronic hepatitis or cirrhosis. n

Symptoms of hepatitis n n n n n Initially non specific symptoms Anorexia Fatigue Nausea Vomiting Diarrhea Fever Weight loss Abdominal discomfort Usually precede by jaundice

Dietary modification Aim: regeneration of liver tissue & prevent further damage. High protein, high CHO & moderate fat diet. Calorie: Initially 1600 -2000 kcal, gradually increase to 20 -30% but as patient is at bed rest normal requirement will meet extra need. Protein: in mild & moderate hepatitis 1. 5 -2 gm /kg body weight. Fats: makes food more palatable & increase calorie intake. In severe cases 20 gm & in moderate 20 -30 gm. More emulsified fats.

Carbohydrate: high carbohydrate diet, 300 -400 gm in form of simple carbs like glucose, fruits, fruit juices, starches Vitamins & minerals: diet should provide all vitamin & mineral in adequate amounts. More Vit C for tissue healing Avoid: Fried & fatty foods Nuts & oilseeds Strongly flavored vegetables Alcohol

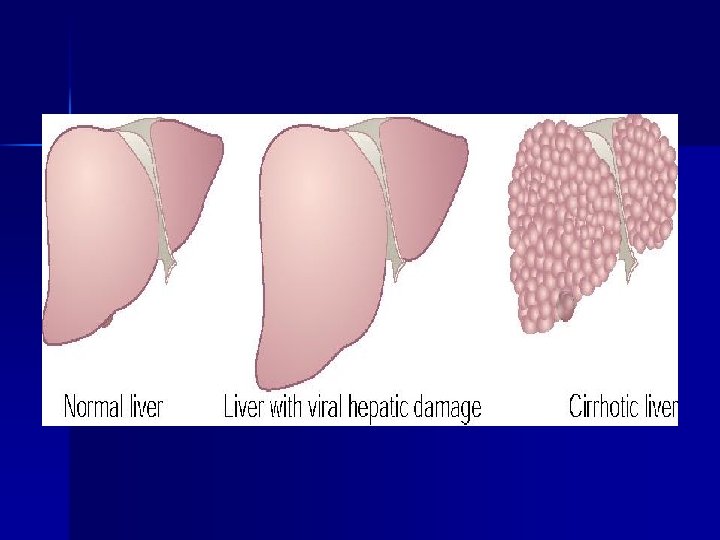
Cirrhosis of the Liver Characterized by diffuse degenerative changes, fibrosis & nodular regeneration of remaining liver cells. Irreversible disease Causes: n Infectious hepatitis in some n Chronic alcoholism with malnutrition n Metabolic disturbances like wilson’s disease, Hemochromatosis n Toxins like hepatotoxins from plants, fungi

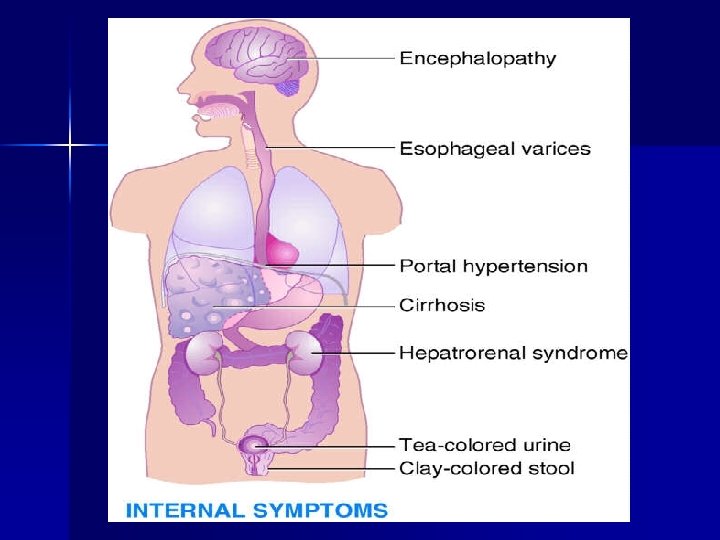
Symptoms n n n Onset may be gradual with GIT disturbances such as anorexia, nausea, vomiting, pain. As disease progress, jaundice Ascites, accumulation of abnormal amount of fluid in abdomen. Esophageal varices (varicose vein), varices in the esophagus & upper part of stomach Hemorrhage, itself may be fatal or Blood may provide accumulation of ammonia & subsequent hepatic coma.

Dietary modification High protein, high CHO diet, moderate or restricted fat, which help in regeneration of liver & help to prevent ascites. n Energy: require high calorie diet because of prolong under nutrition, 2000 -2500 kcal n Protein: in absence of hepatic coma 1. 2 gm/kg of BW can be given. Protein diet varies with the symptoms. If patient is in precoma or coma, protein should be stopped. n Fats: about 20 gm is given.

n n CHO: should be supplied liberally so that liver can store glycogen. 60% calorie should come from CHO Vitamins & minerals: liver is the major site for storage & conversion of vitamins into their metabolic active form. In cirrhosis, all these functions are impaired. Supplementation is required. Sodium is restricted if edema or ascites present. Iron supplementaion

Hepatic coma n Complex syndrome ch. by neurological disturbances develop as a complication of severe liver disease. n Entrance of ammonia in cerebral circulation without being metabolized by liver.

Symptoms Precoma n Confusion n Restlessness n Irritability n Inappropriate behavior n Drowsiness n When extended: incordination & tremors n Electrolyte imbalance n Patient may go in coma n Breath has fecal odor

Diet treatment Reduce protein intake thus decrease the amount of ammonia produced n Calories: about 1500 -2000 kcal to prevent breakdown of tissue protein for energy & given chiefly in form of CHO & fats. n Protein: some omit completely for 2 -3 days & some allow 20 -30 gm. As patient improves gradually it is increased to 1 gm/kg BW under observation. 40 -50 gm protein can be given for long period of time.

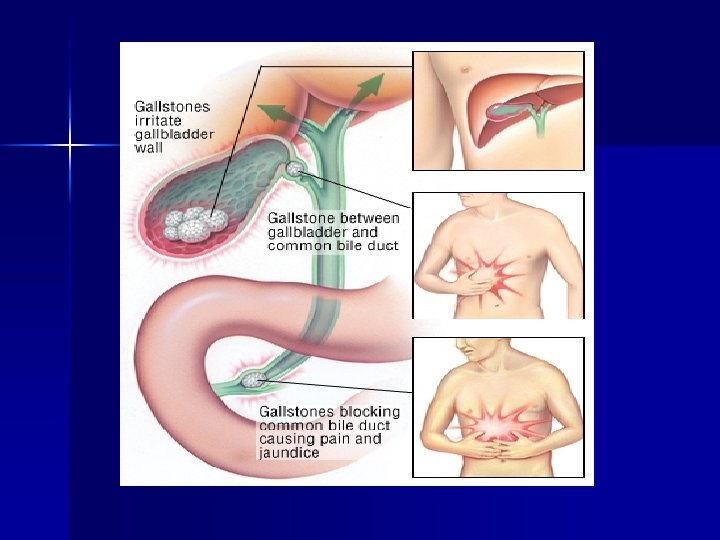
Disease of gall bladder Inflammation of gall bladder is known as cholecystitis. n Gall stone formation is known as cholelithiasis occurs when cholesterol, bile pigments, bile salts, calcium & other substances precipitate out of the bile. n Stones lodged in common duct is known as choledocholithiasis n

Symptoms Mere presence of stone does not produce symptoms n Inflammation & obstruction of duct by stone may cause severe pain whenever gall bladder contracts n Impaired fat digestion n Removal of gall bladder is known as cholecystectomy. n

Risk factors Obesity n Diabetes n Women over 60 n Cholesterol lowering drugs n

Dietary treatment n n If the patient is obese then weight loss is advisable. Fat is main cause of contraction of organ so it must be reduced to 20 gm/day. Energy should be taken mainly from CHO. Foods included: cereals in soft form, milk, curd, cooked & pureed vegetables, pulses, tender meat, fruits , soft cooked eggs etc

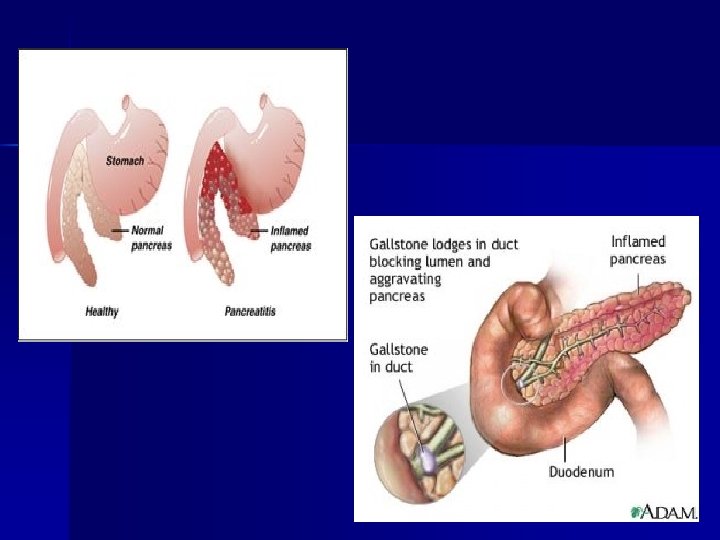
Pancreatic disorder Acute pancreatitis: acute inflammatory disease of pancreas Result from interference with blood supply to the organ or obstruction in flow of pancreatic juice. Causes: 1. Alcoholism 2. Biliary tract disorder 3. Or due to trauma, virus infection, tumors, metabolic disorder

Symptoms: Severe upper abdominal pain radiating to back n Increased after eating n Constipation n Nausea n Vomiting n Distention n

Treatment Aim is to keep pancreatic activity at minimum & replace fluid and electrolytes n Nothing by mouth during acute attacks n Progression from clear liquid to soft diet afterwards. n

Chronic pancreatitis Recurrent attack of burning epigastric pain especially after meals containing alcohol and fat Other symptoms: 1. Flatulence 2. Anorexia 3. Weight loss 4. Nausea 5. Vomiting n

6. Chronic changes lead to destruction of pancreas, fibrosis, pancreatic calcification 7. Steatorrhea

Dietary treatment Diet during attack is same as acute pancreatitis After that a soft diet, high in protein and calorie and low in fat should be given Supplement pancreatic enzymes & fat soluble vitamins Six small meals are better tolerated than large ones.
- Slides: 44