Liver and Billiary Infections Dr V P C
")
Liver and Billiary Infections Dr. V. P. C. Rajakaruna MBBS(COLOMBO)

Cholecystitis • Cholecystitis is inflammation of the gallbladder, classified into acute (with or without calculi) and chronic. • The latter usually follows acute attacks, and infection
 in about 15% of patient,")
Acute cholecystitis • Acute cholecystitis is acalculous (‘without calculi’) in about 15% of patient, in over 85% of patients results from gallstones • Causative organisms include bowel flora, such as enterococci, aerobic Gramnegative rods, and anaerobes including Bacteroides fragilis and Clostridium perfringens.
 of")
Clinical features • Pain is usual anteriorly in the right upper quadrant (RUQ) of the abdomen, commonly in the back also. • Nausea, vomiting, fever and tenderness over the gallbladder are usual, but rigors, jaundice or hypo tension suggest complications such as ascending cholangitis

Confirmatory tests • Ultrasound - shows a dilated gallbladder and may show a dilated common bile duct. The HIDA scan (hepatobiliary iminodiacetic acid scan )shows no gallbladder in acute infection if the cystic duct is blocked

Complications • Cholangitis, • Perforation • Peritonitis

Management • Empiric therapy is against bowel flora, often triple ‘AGM’ (ampicillin, gentamicin and metronidazole). • Early laparoscopic cholecystectomy is safer than delayed surgery, and is imperative in complicated disease.

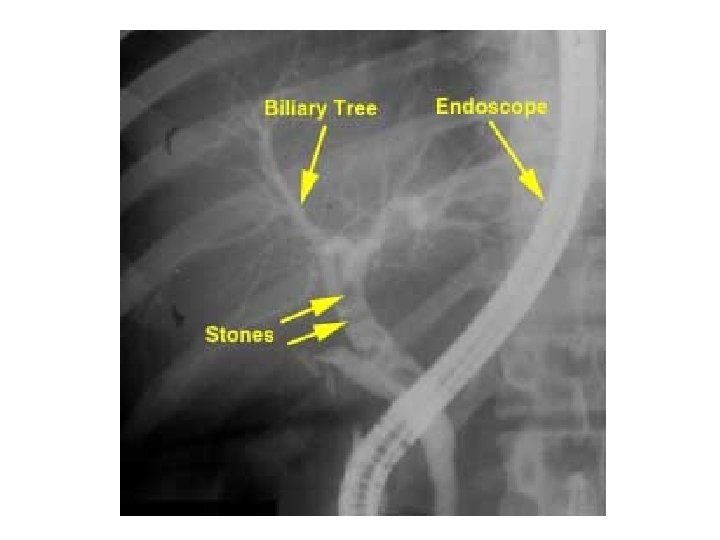
Cholangitis • Cholangitis is infection in the bile ducts, • A stone in the common bile duct is the commonest cause. • Causative organisms are usually bowel flora, but may be parasites: Ascaris lumbricoides, Clonorchis sinensis, Cryptosporidium spp

Clinical symptoms • In 85% of patients, Charcot’s triad – fever, rigors and jaundice – occurs, which progresses to shock and liver failure

Confirmatory tests • Ultrasound and • HIDA scans have diminished the need for percutaneous transhepatic cholangiography • Blood and bile cultures are essential

Management • Triple ‘AGM’ therapy • Surgery to remove obstruction is essential Control and prevention is by early treatment of precipitating factors, e. g. gallstones.

Liver infections, abscesses and cysts

• Diffuse liver infections occur in kala-azar, malaria and schistosomiasis , and viral hepatitis. In addition, the liver is damaged in cholangitis and many systemic infections • Disseminated liver infections occur in granulomatous hepatitis and in infections by mycobacteria (e. g. M. tuberculosis in miliary tuberculosis, and M. avium in AIDS), by fungi (e. g. , hepatosplenic candidiasis in disseminated candidiasis, ) and by other organisms (e. g. , hepatic pneumocystosis, ) • Localised liver abscesses and cysts occur in a number of infections

Amoebic liver abscess • Amoebic abscesses are a complication of Entamoeba histolytica infection • Can occur years after intestinal amoebiasis • Signs and symptoms include right upper quadrant pain and tenderness with fever are usual; only 25% have active amoebic dysentery. • Systemic features including weight loss are prominent. • Referred shoulder tip pain, pleural fluid and a raised right hemidiaphragm occur with abscesses near the diaphragm

Confirmatory tests • Neutrophilia is usual, not eosinophilia. • Ultrasound or CT scan show the abscess(es) • Stool microscopy for amoebae is usually negative unless diarrhoea is present.

Treatment • Metronidazole is the drug of choice
- Slides: 17