LIVER ABSCESS o Occurs when bacteriaprotozoa destroy hepatic

LIVER ABSCESS

o Occurs when bacteria/protozoa destroy hepatic tissue, produces a cavity which fills up with infective organisms, liquefied cells & leucocytes. Necrotic tissue then falls off the cavity from rest of the liver.

Pyogenic abscess Amoebic abscess Prasitic abscess

PYOGENIC ABSCESSClassification o Ascending cholangitis-due to obstruction-gall stones , cancer, sclerosing cholangitis and biliary srtictures. o Portal pyemia-spread from GITappendicitis, empyema of gall bladder, diverticulosis, pancreatitis, infe cted haemorrhoids and neonatal umbilical vein sepsis.

o Septicaemia-spread by hepatic artery o Direct infection resulting in solitary liver abscess-adjascent perinephrc abscess, metastasis and hepatoma following trauma o Iatrogenic causes-liver biopsy, surgical drainage.

Pyogenic abscess o Male preponderance o Average – between 43 & 60 years o Infective organisms invade liver directly after liver wound or spread from lungs, skin or other organs by hepatic artery, portal vein, biliary tract
 E.")
Bacteriology o Majority derived from GI tract in >75% cases o Aerobic: a) E. coli – most common cause b)Klebsiella pneumoniae c)Others: Pseudomonas aerogenosa, Morganella morganii, Serratia marsecens, etc.
 Bacteroides fragilis (most common) b) Others: Fusobacterium spp. , anaerobic Streptococci,")
o Anaerobic: a) Bacteroides fragilis (most common) b) Others: Fusobacterium spp. , anaerobic Streptococci, Clostridium spp. , Actinomyces spp.

Clinical features o Symptoms: Fever Abdominal pain Chills Anorexia Weight loss Nausea, Vomiting Right shoulder pain / irritable cough
")
o Signs: Hepatomegaly Tenderness Rebound tenderness Jaundice (late)

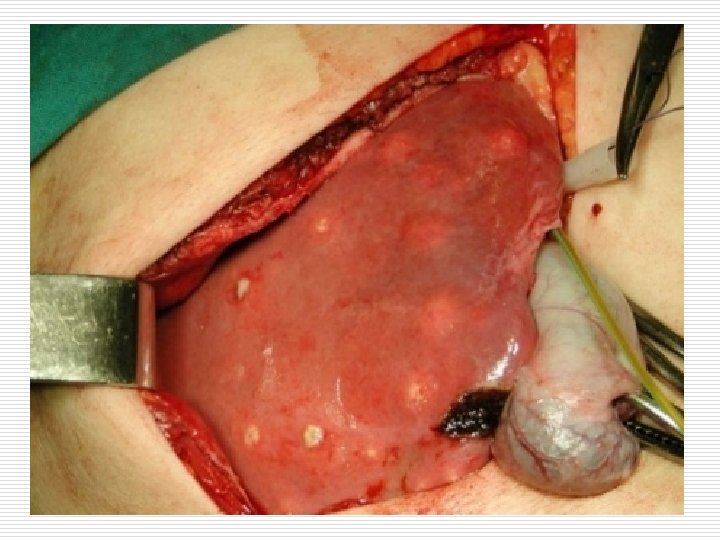
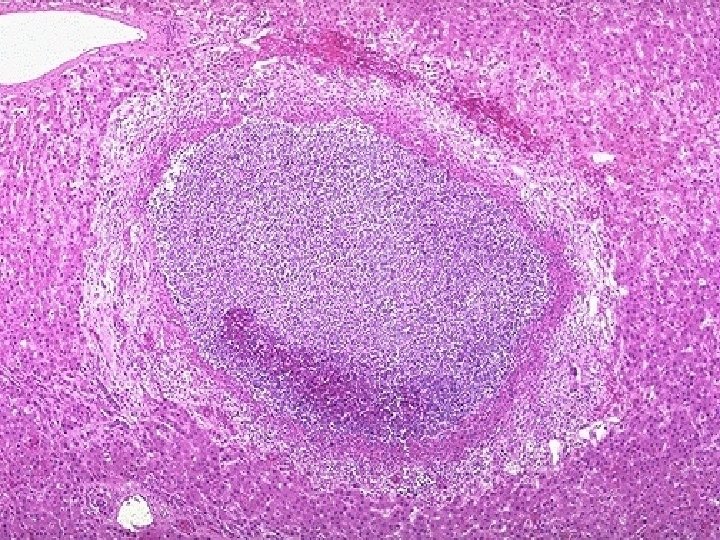
o Gross-single or multiple. 1 cm or more in an enlarged liver. has a thick fibrous capsule common in right lobe. o Microscopy-multiple small neutrophilic abscesses with areas of necrosis of the liver parenchyma. Adjascent viable area shows pus and blood clots in the porta vein.

Inflammation and congestion and fibroblast proliferation. o Extention causes subphrenic or pleuropulmonary suppuration.

Amoebic Abscess o Commonest extra-intestinal presentation of amoebiasis o Common in alcoholics o Caused by Entamoeba histolytica o Entry by faeco-oral route



Pathology o Amoeba multiply-block in intrahepatic portal radicles-focal infarction of liver cellsproteolytic enzymes releaseddistroying liver parenchyma

o Gross-solitary , in rt lobe posterosuperiorly. size varies. centre of the abscess contains large necrotic area which is liquefied into thick reddish-brown pus (Anchovy sauce pus) due to liquefied necrosis, thrombosis of blood vessels, lysis of liver cells


Histology Necrotic area containing degenerated liver cells, leucocytes, RBCs, connective tissue strands, debris & amoebae are found in the liver tissue at the margin of the abscess

Clinical features o Symptoms: High grade fever with rigor Weight loss Upper quadrant pain ( Initially dull aching, later on stabbing) Jaundice (not common)
 Consolidation in right lower zone of lungs Pleurisy")
o Signs: Hepatomegaly (tender) Consolidation in right lower zone of lungs Pleurisy
 Rupture into lung/pleura a) Empyema b) Hepatobronchial fistula c) Pulmonary abscess d)")
Complications 1) Rupture into lung/pleura a) Empyema b) Hepatobronchial fistula c) Pulmonary abscess d) Pneumonitis e) Pleural effusion
 3) 4) 5) Rupture into pericardium Intraperitoneal rupture Rupture into portal vein (rare)")
2) 3) 4) 5) Rupture into pericardium Intraperitoneal rupture Rupture into portal vein (rare) Secondary infection

HYDATID DISEASE o Larval cyst stage of the tape worm, echinococcus granulosus. o Definite host-dog. o Intermediate host-man, sheep and cattle.

Morphology-Hydatid cyst o Size of over 10 cms in 5 rears. o CYST WALL o Pericyst-outer most-inflammatory reaction. o Ectocyst-intermediateacellular, chitinous laminated hyaline material

o Endocyst-inner germinal layer, contains daughter cyst and scolices projecting into the lumen. o Hydatid sand-grain like material containig scolices present in the hydatid fluid.

Complications o Rupture-to peritoneal cavity, bile duct and lungs. o Secondary infection o Hydatid ellrgy.

Thank You
- Slides: 31