List of NIH Institutes Centers and Offices National
 — Est. 1937")
 — Est. 1950 The")
 — Est. in 1964 CIT incorporates the")






 Increase in")











 Cataract formation as assessed by lens opacity classification; (B) Oral glucose tolerance test")

- Slides: 40
List of NIH Institutes, Centers, and Offices National Cancer Institute (NCI) — Est. 1937 NCI leads a national effort to eliminate the suffering and death due to cancer. Through basic and clinical biomedical research and training, NCI conducts and supports research that will lead to a future in which we can prevent cancer before it starts, identify cancers that do develop at the earliest stage, eliminate cancers through innovative treatment interventions, and biologically control those cancers that we cannot eliminate so they become manageable, chronic diseases. National Eye Institute (NEI) — Est. 1968 The National Eye Institute’s mission is to conduct and support research, training, health information dissemination, and other programs with respect to blinding eye diseases, visual disorders, mechanisms of visual function, preservation of sight, and the special health problems and requirements of the blind. National Heart, Lung, and Blood Institute (NHLBI) — Est. 1948 The National Heart, Lung, and Blood Institute (NHLBI) provides global leadership for a research, training, and education program to promote the prevention and treatment of heart, lung, and blood diseases and enhance the health of all individuals so that they can live longer and more fulfilling lives. The NHLBI stimulates basic discoveries about the causes of disease, enables the translation of basic discoveries into clinical practice, fosters training and mentoring of emerging scientists and physicians, and communicates research advances to the public. National Human Genome Research Institute (NHGRI) — Est. 1989 NHGRI is devoted to advancing health through genome research. The Institute led NIH’s contribution to the Human Genome Project, which was successfully completed in 2003 ahead of schedule and under budget. Building on the foundation laid by the sequencing of the human genome, NHGRI’s work now encompasses a broad range of research aimed at expanding understanding of human biology and improving human health. In addition, a critical part of NHGRI’s mission continues to be the study of the ethical, legal and social implications of genome research. National Institute on Aging (NIA) — Est. 1974 NIA leads a national program of research on the biomedical, social, and behavioral aspects of the aging process; the prevention of age-related diseases and disabilities; and the promotion of a better quality of life for all older Americans. National Institute on Alcohol Abuse and Alcoholism (NIAAA) — Est. 1970 NIAAA conducts research focused on improving the treatment and prevention of alcoholism and alcohol-related problems to reduce the enormous health, social, and economic consequences of this disease. National Institute of Allergy and Infectious Diseases (NIAID) — Est. 1948 NIAID research strives to understand, treat, and ultimately prevent the myriad infectious, immunologic, and allergic diseases that threaten millions of human lives. National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS) — Est. 1986 NIAMS supports research into the causes, treatment, and prevention of arthritis and musculoskeletal and skin diseases, the training of basic and clinical scientists to carry out this research, and the dissemination of information on research progress in these diseases. National Institute of Biomedical Imaging and Bioengineering (NIBIB) — Est. 2000 The mission of the National Institute of Biomedical Imaging and Bioengineering (NIBIB) is to improve health by leading the development and accelerating the application of biomedical technologies. The Institute is committed to integrating the physical and engineering sciences with the life sciences to advance basic research and medical care. Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) — Est. 1962 NICHD research on fertility, pregnancy, growth, development, and medical rehabilitation strives to ensure that every child is born healthy and wanted and grows up free from disease and disability. National Institute on Deafness and Other Communication Disorders (NIDCD) — Est. 1988 NIDCD conducts and supports biomedical research and research training on normal mechanisms as well as diseases and disorders of hearing, balance, smell, taste, voice, speech, and language that affect 46 million Americans. National Institute of Dental and Craniofacial Research (NIDCR) — Est. 1948 NIDCR provides leadership for a national research program designed to understand, treat, and ultimately prevent the infectious and inherited craniofacial-oral-dental diseases and disorders that compromise millions of human lives.
National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) — Est. 1950 The mission of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) is to conduct and support medical research and research training and to disseminate science-based information on diabetes and other endocrine and metabolic diseases; digestive diseases, nutritional disorders, and obesity; and kidney, urologic, and hematologic diseases, to improve people’s health and quality of life. National Institute on Drug Abuse (NIDA) — Est. 1974 NIDA leads the nation in bringing the power of science to bear on drug abuse and addiction through strategic support and conduct of research across a broad range of disciplines and rapid and effective dissemination and use of the results of that research to significantly improve prevention and treatment and to inform policy as it relates to drug abuse and addiction. National Institute of Environmental Health Sciences (NIEHS) — Est. 1969 The mission of the National Institute of Environmental Health Sciences is to discover how the environment affects people in order to promote healthier lives. National Institute of General Medical Sciences (NIGMS) — Est. 1962 The National Institute of General Medical Sciences (NIGMS) supports basic research that increases understanding of biological processes and lays the foundation for advances in disease diagnosis, treatment and prevention. NIGMS-funded scientists investigate how living systems work at a range of levels, from molecules and cells to tissues, whole organisms and populations. The Institute also supports research in certain clinical areas, primarily those that affect multiple organ systems. To assure the vitality and continued productivity of the research enterprise, NIGMS provides leadership in training the next generation of scientists, in enhancing the diversity of the scientific workforce, and in developing research capacities throughout the country. National Institute of Mental Health (NIMH) — Est. 1949 NIMH provides national leadership dedicated to understanding, treating, and preventing mental illnesses through basic research on the brain and behavior, and through clinical, epidemiological, and services research. National Institute on Minority Health and Health Disparities (NIMHD) — Est. in 1993 The mission of NIMHD is to lead scientific research to improve minority health and eliminate health disparities. To accomplish its mission, NIMHD plans, reviews, coordinates, and evaluates all minority health and health disparities research and activities of the National Institutes of Health; conducts and supports research in minority health and health disparities; promotes and supports the training of a diverse research workforce; translates and disseminates research information; and fosters innovative collaborations and partnerships. National Institute of Neurological Disorders and Stroke (NINDS) — Est. 1950 The mission of NINDS is to seek fundamental knowledge about the brain and nervous system and to use that knowledge to reduce the burden of neurological disease. To accomplish this goal the NINDS supports and conducts basic, translational, and clinical research on the normal and diseased nervous system. The Institute also fosters the training of investigators in the basic and clinical neurosciences, and seeks better understanding, diagnosis, treatment, and prevention of neurological disorders. National Institute of Nursing Research (NINR) — Est. 1986 The mission of the National Institute of Nursing Research (NINR) is to promote and improve the health of individuals, families, communities, and populations. NINR supports and conducts clinical and basic research and research training on health and illness across the lifespan to build the scientific foundation for clinical practice, prevent disease and disability, manage and eliminate symptoms caused by illness, and improve palliative and end-of-life care. National Library of Medicine (NLM) — Est. 1956 NLM collects, organizes, and makes available biomedical science information to scientists, health professionals, and the public. The Library’s Web-based databases, including Pub. Med/Medline and Medline. Plus, are used extensively around the world. NLM conducts and supports research in biomedical communications; creates information resources for molecular biology, biotechnology, toxicology, and environmental health; and provides grant and contract support for training, medical library resources, and biomedical informatics and communications research.
NIH Centers Center for Information Technology (CIT) — Est. in 1964 CIT incorporates the power of modern computers into the biomedical programs and administrative procedures of the NIH by focusing on three primary activities: conducting computational biosciences research, developing computer systems, and providing computer facilities. Center for Scientific Review (CSR) — Est. in 1946 The Center for Scientific Review (CSR) is the portal for NIH grant applications and their review for scientific merit. CSR organizes the peer review groups or study sections that evaluate the majority (70%) of the research grant applications sent to NIH. CSR also receives all grant applications for NIH, as well as for some other components of the U. S. Department of Health and Human Services (DHHS). Since 1946, the CSR mission has remained clear and timely: to see that NIH grant applications receive fair, independent, expert, and timely reviews — free from inappropriate influences — so NIH can fund the most promising research. Fogarty International Center (FIC) — Est. in 1968 FIC promotes and supports scientific research and training internationally to reduce disparities in global health. National Center for Complementary and Integrative Health (NCCIH) — Est. in 1999 The mission of NCCIH is to define, through rigorous scientific investigation, the usefulness and safety of complementary and integrative health interventions and their roles in improving health and health care. National Center for Advancing Translational Sciences (NCATS) — Est. in 2011 The mission of NCATS is to catalyze the generation of innovative methods and technologies that will enhance the development, testing, and implementation of diagnostics and therapeutics across a wide range of human diseases and conditions. NIH Clinical Center (CC) — Est. in 1953 The NIH Clinical Center, America’s research hospital, provides a versatile clinical research environment enabling the NIH mission to improve human health by investigating the pathogenesis of disease; conducting first-in-human clinical trials with an emphasis on rare diseases and diseases of high public health impact; developing state-of-the-art diagnostic, preventive, and therapeutic interventions; training the current and next generations of clinical researchers; and, ensuring that clinical research is ethical, efficient, and of high scientific quality. This page last reviewed on February 8, 2016
Calorie restriction and prevention of age-associated chronic disease Monkey 30% CR
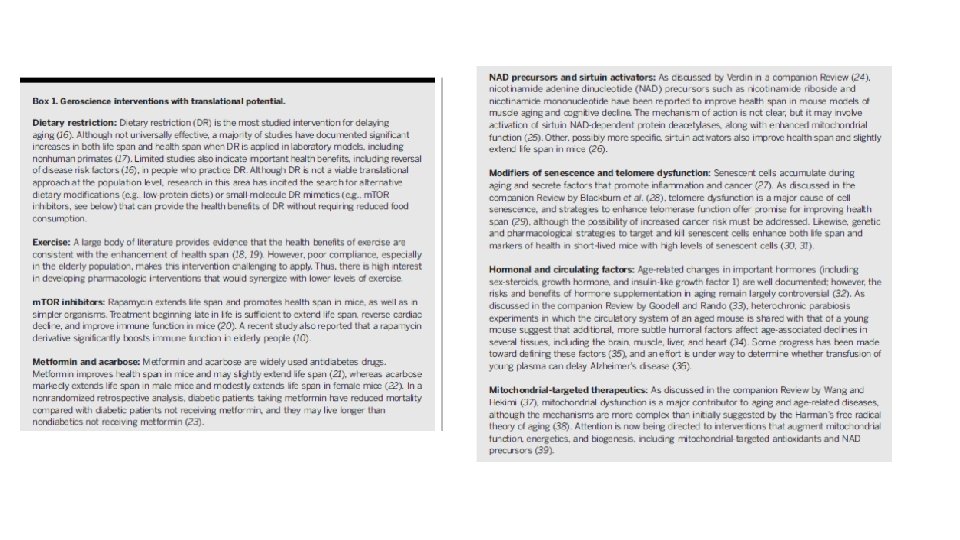
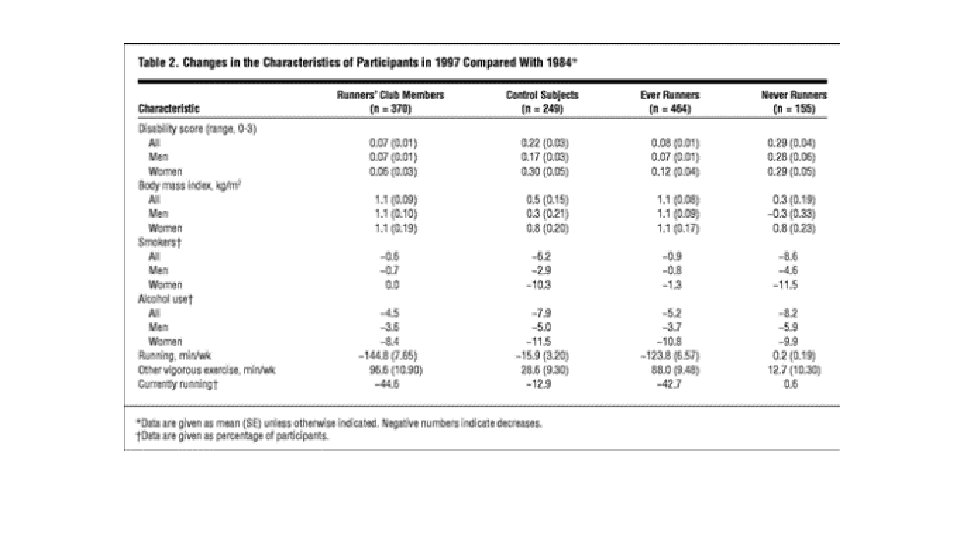
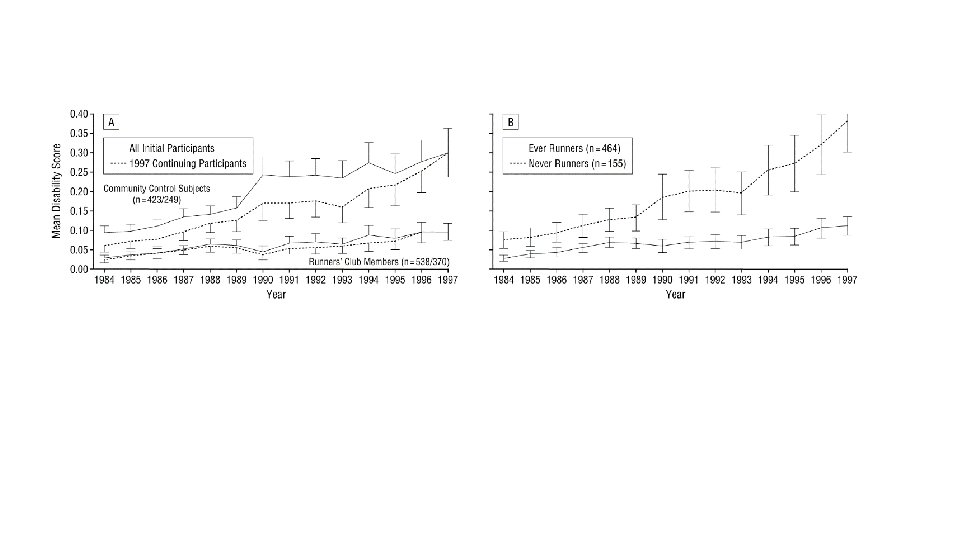
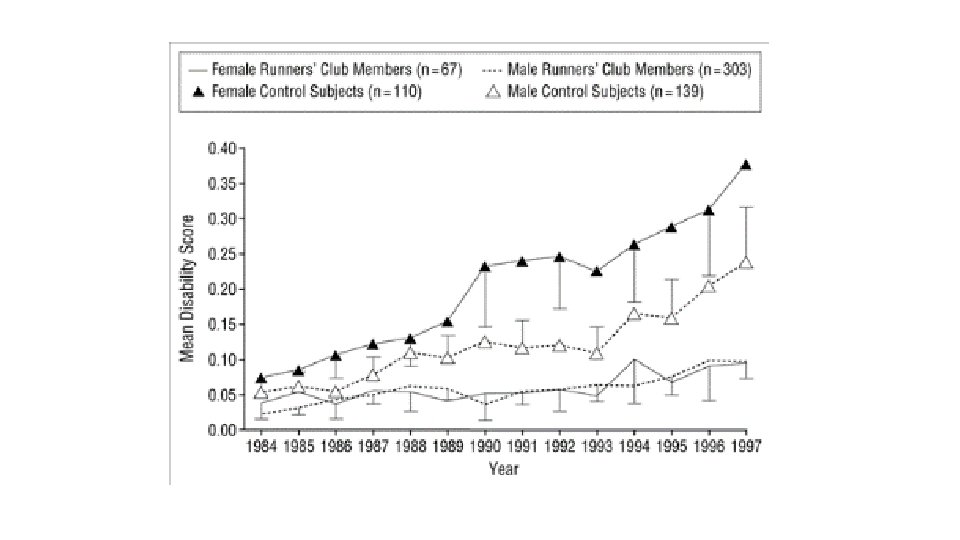
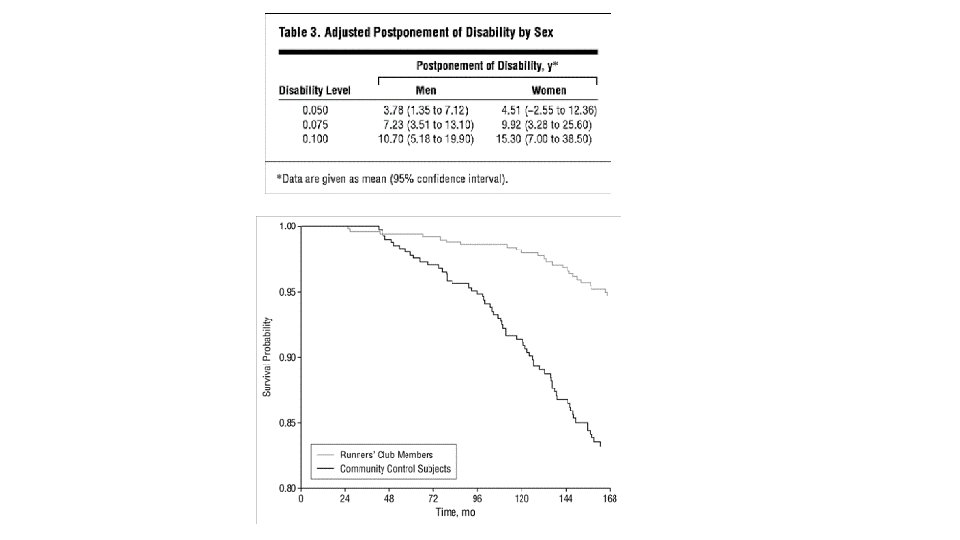
Exercise Postponed Development of Disability in Elderly Runners: A 13 -Year Longitudinal Study
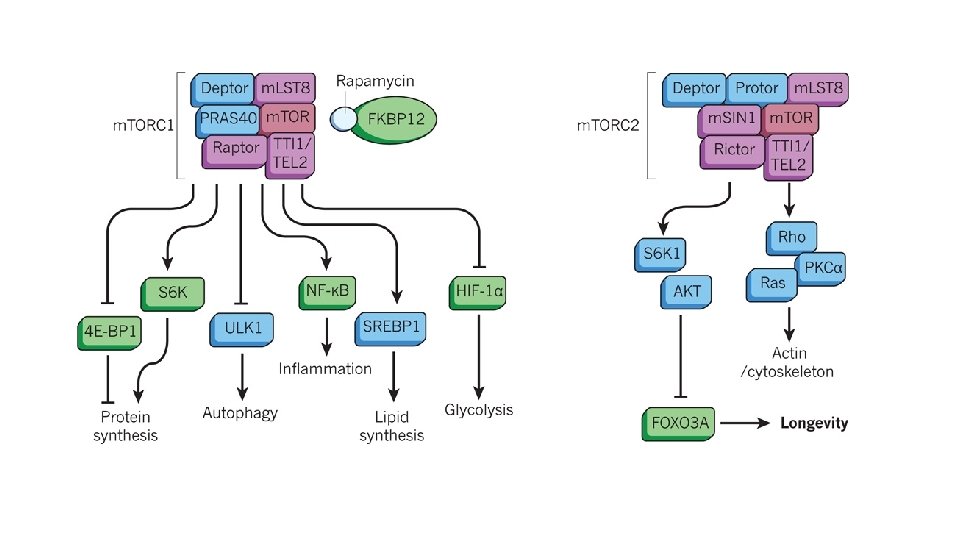
m. TOR inhibitors BOX 1 Key events for rapamycins in ageing • 1970 Soil samples containing rapamycin-producing Streptomyces hygroscopicus taken from the Polynesian island of Rapa Nui • 1975 Purification of rapamycin and identification of fungicidal activity • 1977 Immunosuppressive activity discovered • 1984 Antitumour activity discovered • 1991 TOR 1 and TOR 2 genes identified in yeast • 1994 m. TOR gene FRAP 1, now MTOR, identified in mammals • 1995 Mechanism of action of rapamycin discovered • 1999 Approved by US Food and Drug Administration (FDA) for use in preventing host-rejection in patients undergoing kidney transplantation • 2003 Approved by FDA for use in drug-eluting stents • 2006 Shown to extend lifespan in budding yeast • 2007 Approved by FDA for treatment of renal-cell carcinoma • 2008 Approved by FDA for treatment of mantle cell lymphoma • 2009 Shown to extend lifespan in mice • 2010 Shown to extend lifespan in fruitflies • 2010 Approved by FDA for treatment of tuberous sclerosis • 2011 Shown to improve outcome in mouse models of Alzheimer’s disease • 2011 Approved by FDA for treatment of pancreatic cancer • 2012 Shown to extend lifespan in nematodes • 2012 More than 1, 300 clinical trials under way or completed
Comparison of species in which genetic or pharmacological inhibition of an m. TORC 1 -pathway component extends lifespan Saccharomyces cerevisiae* Caenorhabditis elegans Drosophila melanogaster Mus musculus Rapamycin Yes 9, 10 Yes 11 Yes 12 Yes 13– 15 m. TOR gene mutation and knockdown Yes 8, 9 Yes 6 Yes 7 Yes 3 Raptor gene mutation and knockdown Not reported Yes 5 Not reported Tsc 1 and Tsc 2 activation Not applicable† Not applicable Yes 7 Not reported S 6 K gene mutation and knockdown Yes 4, 8 Yes 24 Yes 7 Yes 37 4 E-BP activation Not applicable Yes 18 Not reported Translation initiation factor mutation and knockdown Yes 44 Yes 17, 24, 75 Not reported Yes 44, 47, 76 Yes 17, 75 Not reported Ribosomal protein mutation and knockdown *Includes both replicative and chronological lifespan; †Not applicable is used in cases for which homologues have not yet been identified
Ageing drives the onset and progression of multiple disorders that are modulated by m. TORC 1 signalling. Data from animal and human studies indicate that some disorders (red arrows) are improved by rapamycins. However, for others (blue arrows), although influenced by rapamycins, evidence suggests there are both beneficial and detrimental consequences of m. TORC 1 inhibition
BOX 2 Effects of m. TORC 1 inhibition on age-related disease Inhibition of m. TORC 1 has positive, and sometimes negative, effects on the age-related pathologies in model organisms and, in some cases, humans. • Neurodegenerative diseases Protection against dopaminergic neuron death in fruitfly and mouse models of Parkinson’s disease 77, 78, delayed disease progression in mouse models of Alzheimer’s disease 79, 80 and frontotemporal lobar dementia 81, and improved spatial learning and memory in old-aged mice 41, 42. • Cancer Reduced growth of solid-tumour cell lines, but disappointing efficacy in clinical trials, with the exception of renalcell carcinoma, breast cancer and several rare forms of cancer 82. • Heart disease Widespread use to prevent restenosis following angioplasty. Reduced hypertrophy 83 and regression of failure 84 in mouse aortic-constriction model. Reduced cardiomyopathy in models of the zebrafish Daniorerio 85 and in mice 86. • Metabolic disease and obesity Resistance to diet-induced 60, 87 and age-associated 88 obesity in mice. However, inhibition is also associated with glucose intolerance and insulin resistance in mice 3, and dyslipidaemia in humans. • Immune function Rapamycins are used in combined immunosuppression therapies in humans. Rapamycin pretreatment enhances immune function in tuberculosis 89, influenza 68 and antitumour vaccine responses in mice 90 and in vaccinia vaccine responses in non-human primates 91. • Kidney disease Decreased rejection and nephrotoxicity in allograft and renal-cancer therapies in patients 92. Improved outcome in animal models of polycystic kidney disease and diabetic nephropathy. • Other health effects Beneficial effects in animal models of age-associated retinopathy 93, and in a variety of disorders that are not obviously age-related, including cerebral ischaemia and reperfusion injury 94, depression 41, autism spectrum disorder 95, muscular dystrophy 86, epilepsy 96, food allergies 97 and autoimmune disorders 98. Decreased need for anti-VEGF intravitreal injections in humans with age-related macular degeneration 99. Reduced toxicity and enhanced clearance of progerin in cells from patients with Hutchinson–Gilford progeria syndrome 100. Negative effects include testicular degeneration and cataracts in mice 58, oral mucositis and stomatitis in humans, and impaired wound healing in humans and animal models.
m. TOR inhibition improves immune function in the elderly (Sci. Tran, Sci) Increase in antibody titers to influenza vaccine strains in RAD 001 -treated versus placebo cohorts. (A) Increase above baseline in GMTs to each of the three influenza vaccine strains (H 1 N 1 A/California/07/2009, H 3 N 2 A/Victoria/210/2009, and B/Brisbane/60/ 2008) 4 weeks after vaccination in RAD 001 -treated cohorts relative to the placebo cohort. The fold changes in GMTs relative to the placebo cohort are shown for all of the RAD 001 dosing cohorts in the intent-to-treat population. The bold black line indicates the 1. 2 -fold increase in titers relative to placebo that is required for two of three influenza vaccine strains in order to meet the primary endpoint of the study. Asterisks indicate that the increase in GMT relative to placebo exceeds 1. 0 with posterior probability of at least 80%. (B) The same data as in (A) are shown for the subset of subjects with baseline influenza titers ≤ 1: 40
Increase in antibody titers to heterologous influenza strains in RAD 001 -treated versus placebo cohorts. Increase above baseline in the GMTs to two heterologous influenza strains (A/H 1 N 1 strain A/New Jersey/8/76 and A/H 3 N 2 strain A/Victoria/361/11) that were not contained in the seasonal influenza vaccine for RAD 001 -treated relative to placebo cohorts, 4 weeks after vaccination. Asterisks indicate that the increase in GMT relative to placebo exceeded 1. 0 with a posterior probability of at least 80%.
Decrease in percent of PD-1–positive CD 4 and CD 8 T cells after RAD 001 treatment. The percent of PD-1–positive CD 4 and CD 8 T cells was determined by fluorescence-activated cell sorting analysis of PBMC samples at baseline, after 6 weeks of drug treatment (week 6), 6 weeks after study drug discontinuation, and 4 weeks after influenza vaccination (week 12). (A) There was a significant decrease of 30. 2% in PD 1–positive CD 4 T cells at week 6 in the pooled RAD 001 -treated cohort (n = 84) compared to the placebo cohort (n = 25) [P = 0. 03 (q = 0. 13)]. The decrease in PD-1–positive CD 4 T cells at week 12 in the pooled RAD 001 -treated cohort compared to the placebo cohort was 32. 7% [P = 0. 05 (q = 0. 19)]. (B) There was a significant decrease of 37. 4% in PD-1–positive CD 8 T cells at week 6 in the pooled RAD 001 -treated cohort (n = 84) compared to the placebo cohort (n = 25) [P = 0. 008 (q = 0. 07)]. The decrease in PD-1 –positive CD 8 T cells at week 12 in the pooled RAD 001 -treated cohort compared to the placebo cohort was 41. 4% [P = 0. 066 (q = 0. 21)].
Metformin promotes lifespan through mitohormesis via the peroxiredoxin PRDX-2 Metformin increases lifespan according to the principle of mitohormesis, for which it requires PRDX-2. (A) Metformin treatment increases metabolic heat production (**P < 0. 01; n = 3 for untreated and n = 4 for treated worms) and respiration (* P < 0. 05; n = 3). Bars represent mean ± SEM. (B) Metformin induced a significant increase in H 2 O 2 release in day-1 adult worms after both continuous exposure during development (*P < 0. 05; n = 7) and after 24 h of exposure, starting from the young adult stage (*P < 0. 05; n = 7 for untreated and n = 5 for treated worms). Exposing the worms for 4 h before measurement did not result in a significant increase ( n. s. P > 0. 05; n = 7). Bars represent mean ± SEM. (C) The antioxidant NAC abolishes the lifespan-extending effect of metformin (***P < 0. 001; n ≥ 169 for each curve; Table S 1). (D) prdx-2 is required for metformin-induced lifespan extension. Metformin treatment significantly reduces lifespan of prdx-2 mutants (***P < 0. 001; n ≥ 127 for each curve; Table S 1). (E) Metformin treatment promotes the formation of PRDX-2 disulfide dimers (**P < 0. 01), implied to function in signal transduction. Bars represent mean ± SEM (n = 4). (F) PRDX-2 is required for metformin-induced phosphorylation of the p 38 MAP kinase PMK-1. Metformin treatment of wild-type worms induced phosphorylation of PMK-1, inferred from a larger band observed on the Western blot. This metformin-mediated induction of PMK-1 phosphorylation is absent in prdx-2 knockout worms. Histone H 3 levels were used as a loading control.
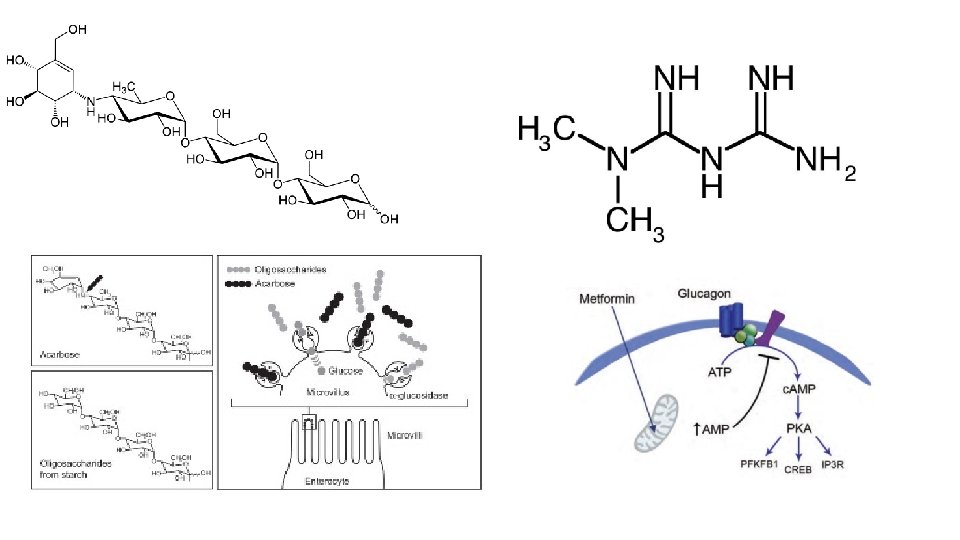
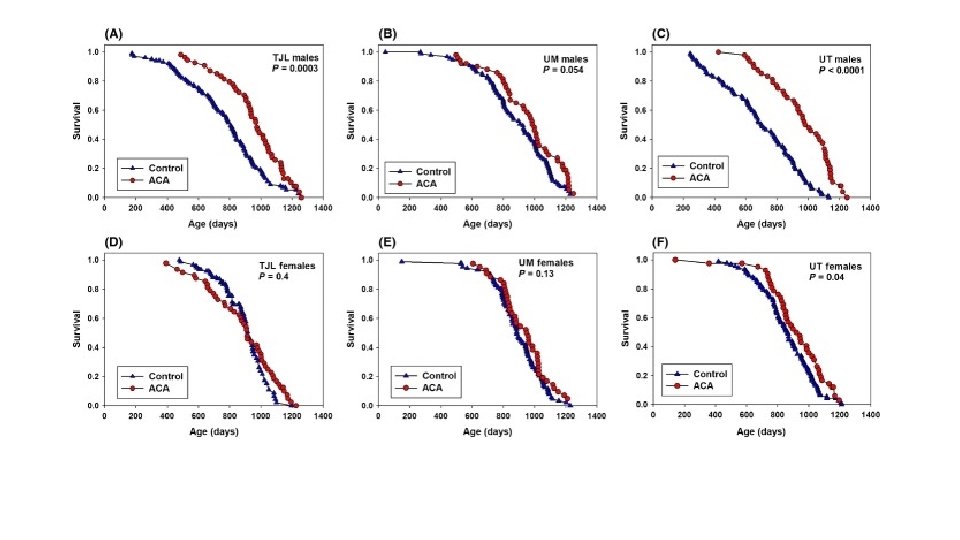
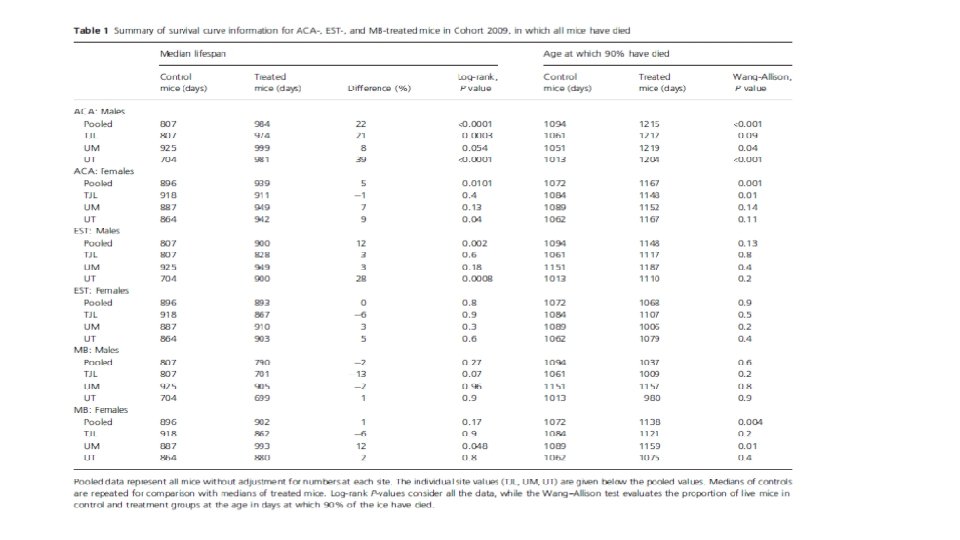
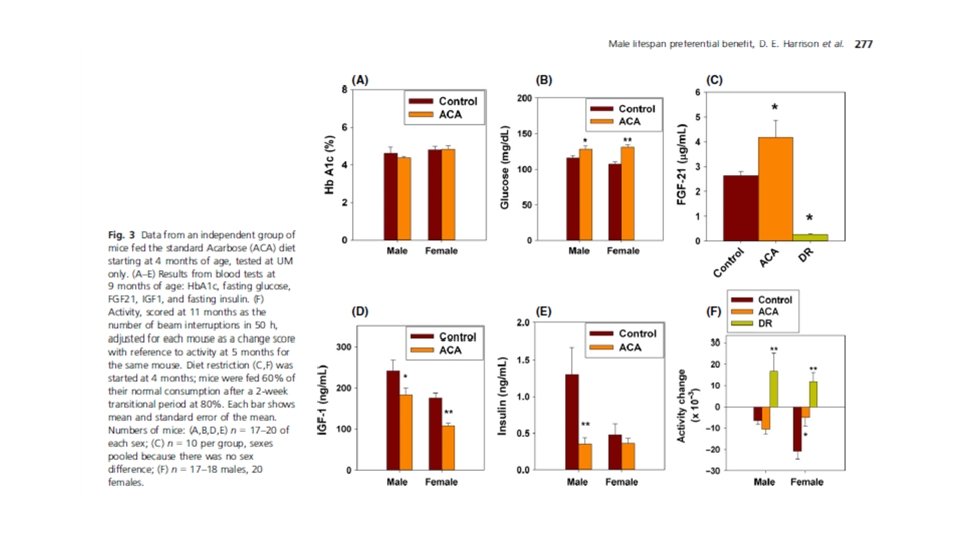
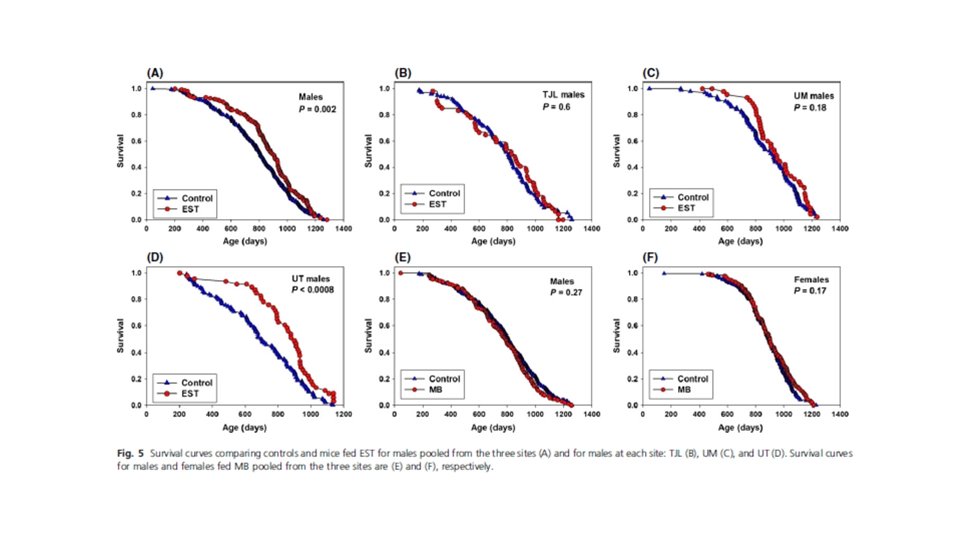
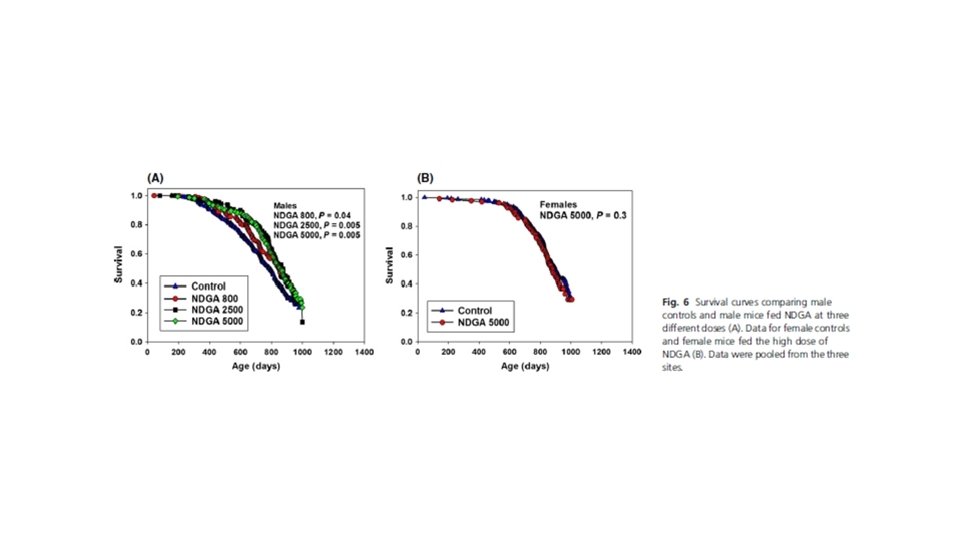
Acarbose, 17 -α-estradiol, and nordihydroguaiaretic acid extend mouse lifespan preferentially in males Aging Cell. 2014 Apr; 13(2): 273– 282.
Can people with type 2 diabetes live longer than those without? A comparison of mortality in people initiated with metformin or sulphonylurea monotherapy and matched, non-diabetic controls
Can people with type 2 diabetes live longer than those without? A comparison of mortality in people initiated with metformin or sulphonylurea monotherapy and matched, non‐diabetic controls Diabetes, Obesity and Metabolism Volume 16, Issue 11, pages 1165 -1173, 31 JUL 2014 DOI: 10. 1111/dom. 12354 http: //onlinelibrary. wiley. com/doi/10. 1111/dom. 12354/full#dom 12354 -fig-0003
NAD+ and Sirtuins in Aging and Disease Various uses of NAD+ for canonical redox and NAD+-consuming enzymatic reactions. Whereas NAD+ is converted to NADH by many metabolic enzymes (a), it is also used as a cosubstrate for NAD+-consuming enzymes, such as poly-ADP-ribose polymerases (PARPs) (b), sirtuins (c), and CD 38/157 ectoenzymes (d).
Absence of effects of Sir 2 over-expression on lifespan in C. elegans and Drosophila
Synthesis of NAD+ is regulated by the circadian clock and declines with age. The oscillating clock consists of the heterodimeric complex of core circadian transcription factors BMAL 1 and CLOCK. The BMAL 1/CLOCK complex controls the Nampt gene encoding the key NAD+ biosynthetic enzyme nicotinamide phosphoribosyltransferase (NAMPT), rendering NAD+ production and SIRT 1 activity circadian in peripheral tissues. SIRT 1 negatively regulates the transcriptional activity of the BMAL 1/CLOCK complex, completing a novel circadian-regulatory feedback loop. In the suprachiasmatic nucleus (SCN), SIRT 1 also regulates Bmal 1 and Clock expression levels via the complex with PGC-1α and RORα. Chronic inflammation, particularly induced by inflammatory cytokines such as TNF-α, might affect NAMPT-mediated NAD+ biosynthesis and BMAL 1/CLOCK-mediated circadian transcription in peripheral tissues and the SCN, causing a decline in the amplitude of the circadian clock with age.
Electron transport via NADH generates NAD+ in mitochondria and may decline with age. In young mitochondria, NADH, made by the citric acid cycle, readily donates its electrons to complex I of the electron transport chain (ETC) and thereby generates NAD+. During the aging process, DNA damage accumulates in the nucleus, causing PARP activation and NAD+ reduction. Consequently, SIRT 1 activity is reduced, resulting in increased PGC-1α acetylation and decreased TFAM levels. These nuclear events might reduce mitochondrial function in old mitochondria by affecting mitochondrial complex I and other mitochondrial components, or blocking the entry of electrons from NADH into the ETC, thereby creating an NAD deficiency.
The SIRT 1 activator SRT 1720 extends lifespan and improves health of mice fed a standard diet small molecule activators of SIRT 1, such as resveratrol and SRT 1720 (A) Kaplan-Meier survival curves for mice fed either a standard diet (SD) or high-fat diet (HFD) supplemented without or with SRT 1720 (SD-SRT 1720, HFD-SRT 1720); (B) Average body weight over the study; (C) Average daily caloric intake over the study; (D) Percentage fat mass measured by nuclear magnetic resonance spectroscopy at 13 months of age; (E) Respiratory Exchange Ratio (RER); (F) Rotarod performance. Data are shown as mean ± SEM. * p≤ 0. 05 compared to diet without SRT 1720.
(A) Cataract formation as assessed by lens opacity classification; (B) Oral glucose tolerance test with area under the curve (inset); (C) The homeostatic model assessment calculation of insulin resistance (HOMA-IR) and serum biochemical markers. Data are shown as mean ± SEM. * p≤ 0. 05 compared to SD diet without SRT 1720.
SRT 1720 elicits differential gene expression profiles in the liver and muscle of SD-fed mice. Principal component analysis (PCA) was performed on (A) liver and (B) skeletal muscle of SD-fed mice supplemented without and with SRT 1720. (C) Parametric analysis of gene-set enrichment (PAGE) analysis was performed on microarray data. Columns show significantly up - (red) and down-regulated (blue) pathways following SRT 1720 supplementation. (D) m. RNA expression analysis in liver and skeletal muscle by quantitative real-time PCR. Relative expression values were normalized to those of SD-fed control mice. (E) Serum tumor necrosis factor alpha (TNF-α) concentrations in SD-fed mice supplemented or not with SRT 1720. Data are shown as mean ± SEM. (F) Western blotting of liver lysates from SD-fed mice supplemented or not with SRT 1720. Upper left panel, representative blots; remaining panels, Signals associated with bands of interest were normalized to GAPDH and plotted. * p≤ 0. 05; ** p≤ 0. 01; *** p≤ 0. 001 when compared to SD-fed control animals.