Lipid Transport Lipoprotein Structure Function and Metabolism Introduction

Lipid Transport Lipoprotein Structure, Function, and Metabolism

Introduction • Fats are triacylglycerols containing saturated fatty acids - solid at room temp - usually from animal source (however, coconut & palm oil are saturated). • Oils are triacylglycerols containing mono- or polyunsaturated fatty acids - liquid at room temp - usually from plant sources (however, fish oils are polyunsaturated). • Phospholipids are triacylglycerols that have had a FA replaced with a phosphate linked FA group. • The major dietary sterol is cholesterol.

Health issues • Excessive dietary fat intake is associated with obesity, diabetes, cancer, hypertension and atherosclerosis. • Not more than 35% of energy intake should come from fat. Saturated fat should not make up more than 15% of the total fat intake. • Omega-3 fatty acids (20 carbons) from fish may protect against atherosclerosis. American Heart association recommends 2 -3 fish meals per weak. Fish oil supplements should be avoided because they may be contain concentrated toxins accumulated by the fish.

FUNCTIONS OF LIPIDS: • Major components of cell membranes. • Required to solubilise fat soluble vitamins • Biosynthetic precursors (e. g. steroid hormones from cholesterol) • Protection (e. g. kidneys are shielded with fat in fed state) • Insulation

LIPID DIGESTION • Stomach - lingual lipase and gastric lipase attack triacylglycerols and hydrolyse a limited number of FA. • Small Intestine - acid chyme (stomach contents) stimulates mucosa cells to release hormone (choleocystokinin) which stimulates gall bladder and pancreas to release bile and digestive enzymes respectively (bile acids help emulsify fat droplets thus increasing their surface area). • Other mucosa cells release secretin which causes pancreas to release bicarbonate rich fluid to neutralise chyme.

Enzymic digestion of lipids in small intestine 2 -monoacylglycerol

• Enzymic digestion generates more polar products that form mixed micelles of free fatty acids, 2 -monoacylglycerol, cholesterol & bile salts that are adsorbed (except bile salts which pass through to ileum – see later). • Once adsorbed fatty acids and 2 -monoacylglycerol are recombined to form triacylglycerol. • Triacylglycerol + cholesterol + phospholipid + proteins form a lipoprotein complex called a chylomicron which transports the lipids in the circulation.

Lipid transport in the circulation Lipids are insoluble in plasma. In order to be transported they are combined with specific proteins to form lipoproteins: Proteins (apoproteins) Cholesterol Non polar lipids in core (TAG and cholesterol esters) Apoproteins are only weakly associated with a particular lipoprotein and are easily transferred to another lipoprotein of a different class. Apoproteins have various functions including: • Structural role • Binding sites for receptors • Activators or co-enzymes for enzymes involved with lipid metabolism

The five classes of lipoprotein (all contain characteristic amounts TAG, cholesterol esters, phospholipids and apoproteins) Increasing density Class Diameter (nm) Major apoliproteins Source and function Chylomicrons (CM) 500 Intestine. Transport of dietary TAG A, B 48, C(I, III) E Very low density lipoproteins (VLDL) 43 Liver. Transport of endogenously synthesised TAG B 100, C(I, III) , E Low density lipoproteins (LDL) 22 Formed in circulation by partial breakdown of IDL. Delivers cholesterol to peripheral tissues B 100 High density lipoproteins (HDL) 8 Liver. Removes “used” cholesterol from tissues and takes it to liver. Donates apolipoproteins to CM and VLDL A, C(I, III), D, E

Apolipoproteins n n n Provide structural stability to Lp Serve as ligands for interaction w/Lp receptors that help determine disposition of individual particles Act as cofactors for enzymes involved in plasma lipid and Lp metabolism
 Apo B-100 VLDL, IDL, LDL")
There are many types of apolipoproteinsa Apoprotein Lipoproteins Function(s) Apo B-100 VLDL, IDL, LDL 1) Secretion of VLDL from liver 2) Structural protein of VLDL, IDL, and HDL 3) Ligand for LDL receptor (LDLR) Apo B-48 Chylomicrons, remnants Secretion of chylomicrons from intestine; lacks LDLR binding domain of Apo B-100 Apo E Chylomicrons, VLDL, IDL, HDL Ligand for binding of IDL & remnants to LDLR and LRP Apo A-I HDL, chylomicrons 1) Apo A-II HDL, chylomicrons Unknown Apo C-I Chylomicrons, VLDL, IDL, HDL Modulator of hepatic uptake of VLDL and IDL (also involved in activation of LCAT) Apo C-II Chylomicrons, VLDL, IDL, HDL Activator of LPL Apo C-III Chylomicrons, VLDL, IDL, HDL Inhibitor of LPL activity Major structural protein of HDL 2) Activator of LCAT

Plasma Lipoproteins Structure n LP core n n n Triglycerides Cholesterol esters LP surface n n n Phospholipids Proteins cholesterol
 Diameter (nm) Protein % Phospholi Triacylglycerol of dry wt")
Lipoprotein class Density (g/m. L) Diameter (nm) Protein % Phospholi Triacylglycerol of dry wt pid % % of dry wt HDL 1. 063 -1. 21 5 – 15 33 29 8 LDL 1. 019 – 1. 063 18 – 28 25 21 4 IDL 1. 006 -1. 019 25 - 50 18 22 31 VLDL 0. 95 – 1. 006 30 - 80 10 18 50 chylomicrons < 0. 95 100 - 500 1 -2 7 84 Composition and properties of human lipoproteins most proteins have densities of about 1. 3 – 1. 4 g/m. L and lipid aggregates usually have densities of about 0. 8 g/m. L

Plasma Lipoproteins Classes & Functions n Chylomicrons n n Synthesized in small intestine Transport dietary lipids 98% lipid, large sized, lowest density Apo B-48 n n Apo C-II n n Receptor binding Lipoprotein lipase activator Apo E n Remnant receptor binding

Chylomicron n n formed through extrusion of resynthesized triglycerides from the mucosal cells into the intestinal lacteals flow through the thoracic ducts into the suclavian veins degraded to remnants by the action of lipoprotein lipase (Lp. L) which is located on capillary endothelial cell surface remnants are taken up by liver parenchymal cells due to apo. E-III and apo. E-IV isoform recognition sites
 Mature chylomicron (+apo C & apo E)")
Chylomicron Metabolism n n Nascent chylomicron (B-48) Mature chylomicron (+apo C & apo E) Lipoprotein lipase Chylomicron remnant n n Apo C removed Removed in liver
 n n Synthesized")
Plasma Lipoproteins Classes & Functions n Very Low Density Lipoprotein (VLDL) n n Synthesized in liver Transport endogenous triglycerides 90% lipid, 10% protein Apo B-100 n n Apo C-II n n Receptor binding LPL activator Apo E n Remnant receptor
 n n n Synthesized")
Plasma Lipoproteins Classes & Functions n Intermediate Density Lipoprotein (IDL) n n n Synthesized from VLDL during VLDL degradation Triglyceride transport and precurser to LDL Apo B-100 n n Apo C-II n n Receptor binding LPL activator Apo E n Receptor binding
 n n Synthesized from")
Plasma Lipoproteins Classes & Functions n Low Density Lipoprotein (LDL) n n Synthesized from IDL Cholesterol transport 78% lipid, 58% cholesterol & CE Apo B-100 n Receptor binding

LDL molecule
 + HDL (apo C & E) =")
VLDL Metabolism n n Nascent VLDL (B-100) + HDL (apo C & E) = VLDL LPL hydrolyzes TG forming IDL n n 75% of IDL removed by liver n n IDL loses apo C-II (reduces affinity for LPL) Apo E and Apo B mediated receptors 25% of IDL converted to LDL by hepatic lipase n Loses apo E to HDL
 n n n Synthesized")
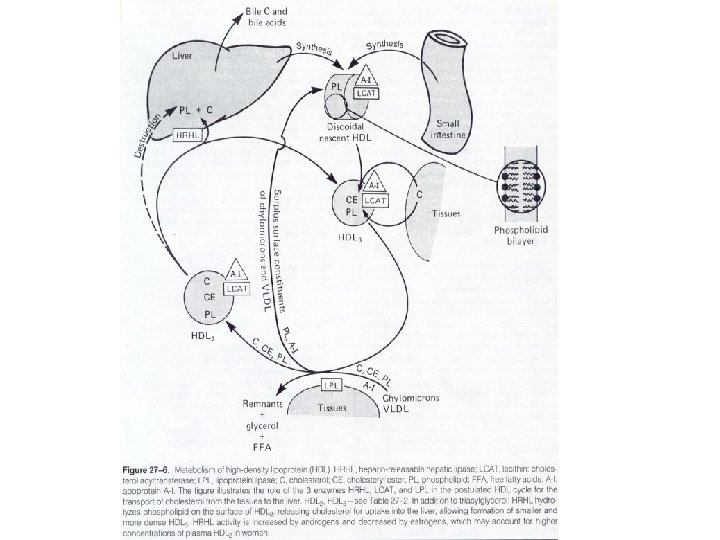
Plasma Lipoproteins Classes & Functions n High Density Lipoprotein (HDL) n n n Synthesized in liver and intestine Reservoir of apoproteins Reverse cholesterol transport 52% protein, 48% lipid, 35% C & CE Apo A n n Apo C n n Activates lecithin-cholesterol acyltransferase (LCAT) Activates LPL Apo E n Remnant receptor binding

Functions of HDL n n n transfers proteins to other lipoproteins picks up lipids from other lipoproteins picks up cholesterol from cell membranes converts cholesterol to cholesterol esters via the LCAT reaction transfers cholesterol esters to other lipoproteins, which transport them to the liver (referred to as “reverse cholesterol transport)

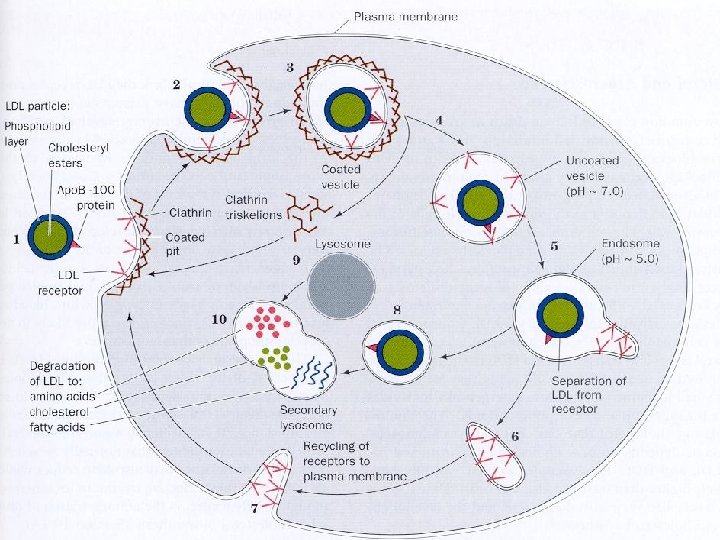

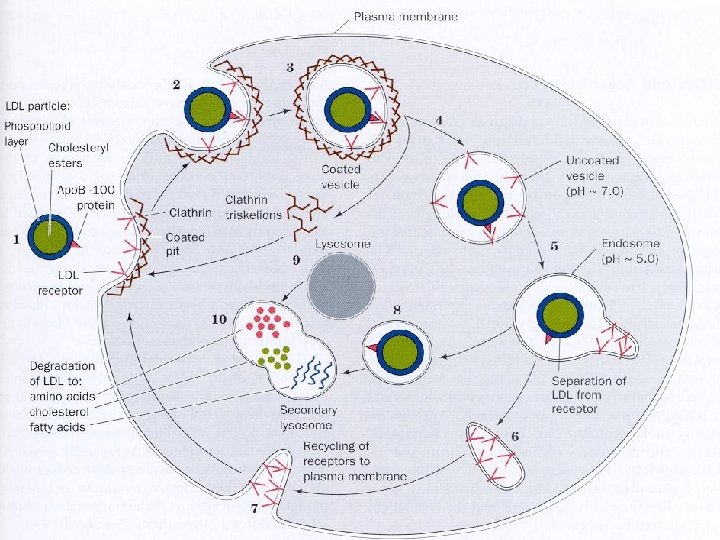
LDL Metabolism n LDL receptor-mediated endocytosis n LDL receptors on ‘coated pits’ n n Endocytosis n n n Clathrin: a protein polymer that stabilizes pit Loss of clathrin coating uncoupling of receptor, returns to surface Fusing of endosome with lysosome n Frees cholesterol & amino acids

Coordinate Control of Cholesterol Uptake and Synthesis n n Increased uptake of LDLcholesterol results in: inhibition of HMG-Co. A reductase n n stimulation of acyl Co. A: cholesterol acyl transferase (ACAT) n n n reduced cholesterol synthesis increased cholesterol storage TG + C -> DG + CE decreased synthesis of LDL-receptors n n “down-regulation” decreased LDL uptake

Heterogeneity of LDL-particles n Not all LDL-particles the same n n n Small dense LDL (diameter <256 A) Large buoyant LDL (diameter >256 A) Lamarche B, St-Pierre AC, Ruel IL, et al. A prospective, population-based study of low density lipoprotein particle size as a risk factor for Can J Cardiol 2001; 17: 859 -65. n n 2057 men with hi LDL, 5 year follow-up Those with elevated small dense LDL had RR of 2. 2 for IHD compared to men with elevated large buoyant LDL Detection expensive Treatment for lowering small dense LDL similar to lowering all LDL (diet, exercise, drugs) n Some drugs (niacin, fibrates) may be more effective at lowering small dense LDL.

LDL Particle Size and Apolipoprotein B Predict Ischemic Heart Disease: Quebec Cardiovascular Study 6. 2 (p<0. 001) Apo B 2. 0 1. 0 >25. 64 1. 0 <25. 64 LDL Peak Particle Diameter (nm) >120 mg/dl <120 mg/dl

HDL Metabolism: Functions n Apoprotein exchange n n provides apo C and apo E to/from VLDL and chylomicrons Reverse cholesterol transport
")
Reverse cholesterol transport n n Uptake of cholesterol from peripheral tissues (binding by apo-A-I) Esterification of HDL-C by LCAT n n n LCAT activated by apo. A 1 Transfer of CE to lipoprotein remnants (IDL and CR) by CETP removal of CE-rich remnants by liver, converted to bile acids and excreted

Cholesterol and lipid transport by lipoproteins

Cholesterol and lipid transport by lipoproteins

The LDL receptor n n n characterized by Michael Brown and Joseph Goldstein (Nobel prize winners in 1985) based on work on familial hypercholesterolemia receptor also called B/E receptor because of its ability to recognize particles containing both apos B and E activity occurs mainly in the liver receptor recognizes apo E more readily than apo B-100

Atherosclerosis n n hardening of the arteries due to the deposition of atheromas heart disease is the leading cause of death caused by the deposition of cholesteryl esters on the walls of arteries atherosclerosis is correlated with high LDL and low HDL

Factors promoting elevated blood lipids n n n n age n men >45 years of age; women > 55 years of age family history of CAD smoking hypertension >140/90 mm Hg low HDL cholesterol obesity >30% overweight diabetes mellitus inactivity/ lack of exercise

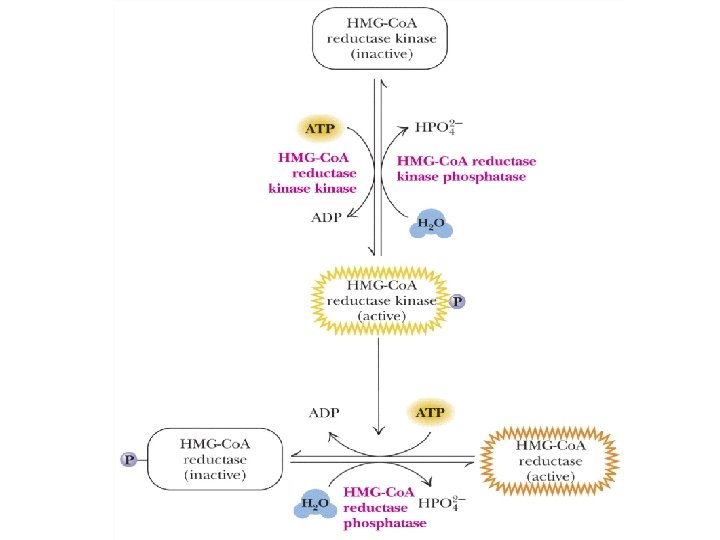
HMG Co. A reductase n 3 different regulatory mechanisms are involved: n n n covalent modification: phosphorylation by c. AMP -dependent protein kinases inactivate the reductase. This inactivation can be reversed by 2 specific phosphatases degradation of the enzyme – half life of 3 hours and the half-life depends on cholesterol levels gene expression: cholesterol levels control the amount of m. RNA


HMG Co. A reductase inhibitors n Precaution: n n n mild elevation of serum aminotransferase (should be measured at 2 to 4 month intervals) minor increases in creatine kinase (myopathy, muscle pain and tenderness) do not give during pregnancy
 n n “Bad” cholesterol Delivers cholesterol to cells Can increase build-up")
Low-Density Lipoproteins (LDLs) n n “Bad” cholesterol Delivers cholesterol to cells Can increase build-up of plaque High levels of LDL associated with increased risk for cardiovascular disease
 n n n “Good” cholesterol Made by liver Circulates in the")
High-Density Lipoproteins (HDLs) n n n “Good” cholesterol Made by liver Circulates in the blood to collect excess cholesterol from cells Returns cholesterol to liver for excretion in bile Highest protein content

Overview of Lipoproteins

LDL n n n = Low Density Lipoprotein Made in: the Liver as VLDL Arise from: VLDL once it has lost a lot of its TG’s Secreted into: the bloodstream Rich in: Cholesterol Function: Deliver cholesterol to all body cells

HDL n n n = High Density Lipoprotein Made in: the Liver and Small Intestine Secreted into: the bloodstream Function: Pick up cholesterol from body cells and take it back to the liver = “reverse cholesterol transport” Potential to help reverse heart disease

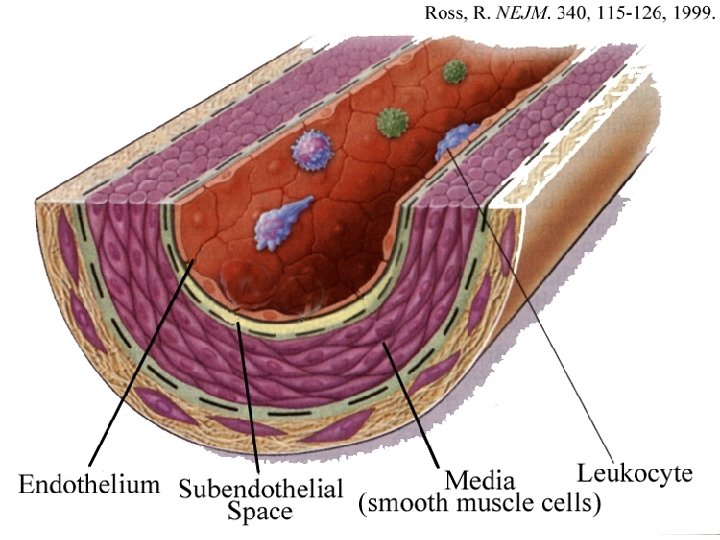
 n n n Main type of CVD is Atherosclerosis (AS) Endothelial")
Cardiovascular Disease (CVD) n n n Main type of CVD is Atherosclerosis (AS) Endothelial dysfunction is one of earliest changes in AS Mechanical, chemical, inflammatory mediators can trigger endothelial dysfunction: n High blood pressure n Smoking (free radicals that oxidatively damage endothelium) n Elevated homocysteine n Inflammatory stimuli n Hyperlipidemia

A Healthy Endothelium produces: áPGI 2 áNO Maintaining an anti-coagulant, anti-thrombotic surface

A Dysfunctional Endothelium has decreased: âPGI 2 âNO Increased: pro-inflammatory molecules: áMCP-1 áTNF áVCAM-1 Shifting to a pro-coagulant, prothrombotic surface
 Inflammatory cytokines =")
Pro-Inflammatory Molecules n n Chemokines = monocyte chemoattractant protein 1 (MCP-1) Inflammatory cytokines = tumor necrosis factor (TNF ) Adhesion molecules = intercellular adhesion molecule 1 (ICAM-1), vascular cell adhesion molecule 1 (VCAM-1) Overexpression of all these inflammatory mediators is commonly seen in atherosclerotic lesions.
 n âendothelial synthesis of PGI 2")
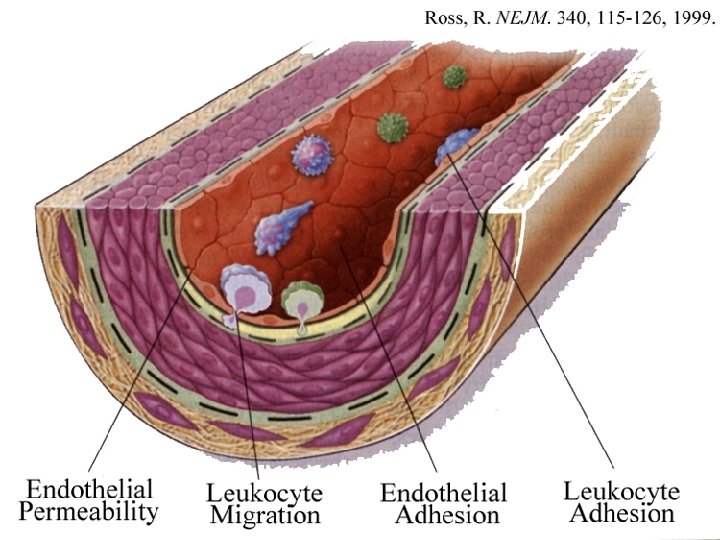
Endothelial Dysfunction ( endothelial activation, impaired endothelial-dependent vasodilation) n âendothelial synthesis of PGI 2 (prostacylcin), & NO (nitric oxide) n n PGI 2 = vasodilator, âplatelet adhesion/aggregation NO = vasodilator, âplatelet & WBC (monocyte) adhesion áAdhesion of monocytes onto endothelium -> transmigration into subendothelial space (artery wall) --> change to macrophages Endothelial dysfunction --> increased flux of LDL into artery wall
 n n Oxidation = process by which free radicals")
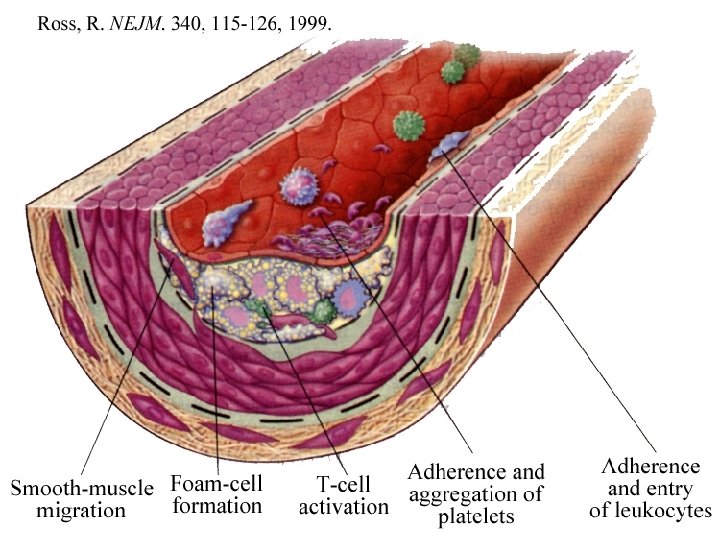
Oxidation of LDL (ox. LDL) n n Oxidation = process by which free radicals (oxidants) attack and damage target molecules / tissues Targets of free radical attack: n n DNA Proteins SFA’s - carbohydrates - PUFA’s>>> MUFA’s>>>>> LDL can be oxidatively damaged: PUFA’s are oxidized and trigger oxidation of apo. B 100 protein --> ox. LDL Ox. LDL is engulfed by macrophages in subendothelial space
 Accumulation of ox. LDL")
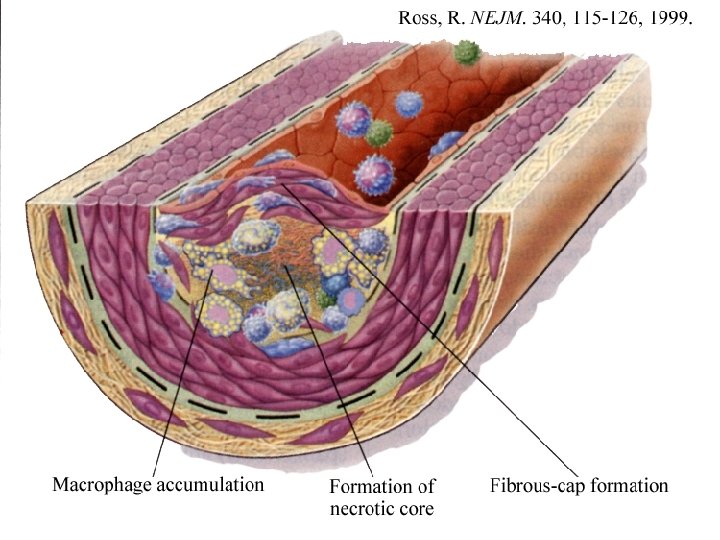
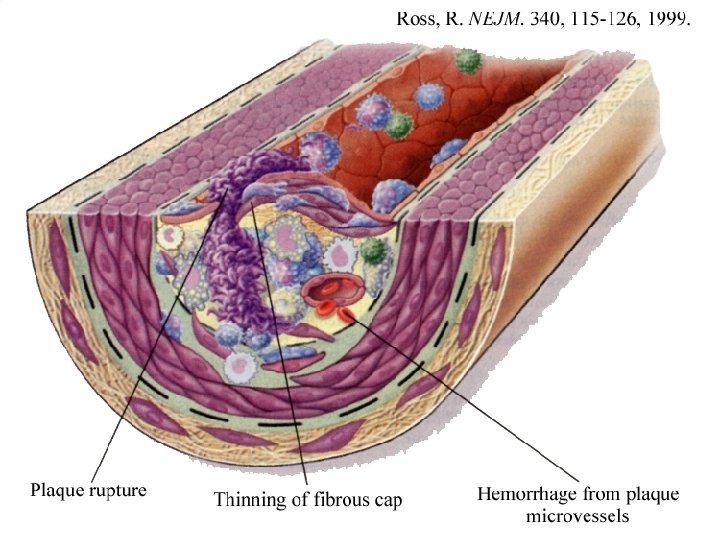
Atherosclerotic Plaque n n n Continued endothelial dysfunction (inflammatory response) Accumulation of ox. LDL in macrophages (= foam cells) Migration and accumulation of: n n n smooth muscle cells, additional WBC’s (macrophages, T-lymphocytes) Calcific deposits Change in extracellular proteins, fibrous tissue formation High risk = áVLDL (áTG) áLDL âHDL

Antioxidant Defense Systems n 1. Prevent oxidation from being initiated n 2. Halt oxidation once it has begun n 3. Repair oxidative damage
 n Flavanoids and other phytochemicals")
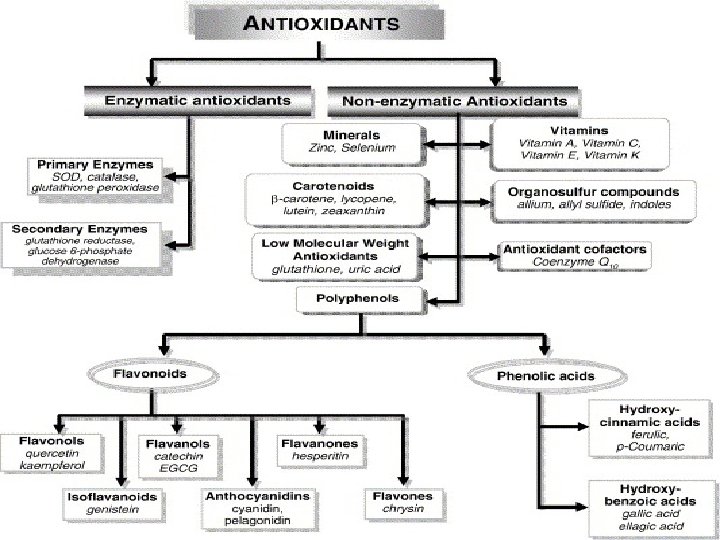
Antioxidant Mechanisms n Antioxidant vitamins (vitamins C, E, carotenoids) n Flavanoids and other phytochemicals n Antioxidant enzyme systems n Minerals required: Mn, Cu, Zn, Se


Factors Associated with CVD n Genetic Variables n n n Being male Being post-menopausal female Family history of heart disease before the age of 55 (some are associated with genetic defects in LDL receptors)

Factors Associated with CVD • Dietary 1. Elevated levels of LDL --More LDL around to potentially oxidize and accumulate in artery wall 2. Low levels of HDL --HDL carries cholesterol from artery walls back to the liver 3. Low levels of antioxidant vitamins --Vit. E, Vit. C, Beta-carotene 4. Low levels of other dietary antioxidants --Phenolics, flavanoids, red wine, grape juice, vegetables, fruits

Factors Associated with CVD n High blood pressure • Damages the artery wall allowing LDL to enter the wall more readily Cigarette Smoking n n n Cigarette smoke products are oxidants and can oxidize LDL Cigarette smoking compromises the body’s antioxidant vitamin status, especially Vit. C Damages the artery wall Activity Level n Exercise is the most effective means of raising HDL levels Obesity

Homocysteine Levels n n n Normal byproduct of certain metabolic pathways Normally metabolized to other products Elevated levels cause damage to artery walls = increased the oxidation of LDL Elevated homocysteine levels are significantly correlated with increased risk to heart disease. Vitamins B 6, B 12, and Folic acid normalize homocysteine levels.
 Enzymes B 12, Folate Homocysteine SAM Enzym e B")
Diet Methionine (a. a. ) Enzymes B 12, Folate Homocysteine SAM Enzym e B 6 cysteine CH SAH sulfate 3 1. Norepinephrine 2. Guanidinoacetate 3. Serotonin 4. Serine 1. Epinephrine 2. Creatine 3. Melatonin 4. Choline

Dietary/Lifestyle Prevention/Intervention of Heart Disease Maintain Endothelial Function Platelet Activity Decrease LDL Increase HDL Increase Antioxida nts âHigh Blood Pressure á w-3 PUFAs â w -6 PUFA âSaturated Fat áMUFA/ â PUFA á MUFA/ â w -6 PUFA âHomocysteine B 6, B 12, Folic Acid á Phytochemicals âCholesterol áw-3 PUFAs (fish) áVegetables áPhytochemicals Aspirin áw-3 oils (fish) á Exercise áFruits Stop smoking áFiber Stop smoking âTrans Fats âBody weight if overweight áFiber

Know Your Lipid Profile Fasting Blood Level Ideal, Healthy Level Total Cholesterol < 200 mg/dl LDL-Cholesterol < 100 mg/dl HDL-Cholesterol ≥ 60 mg/dl Triglycerides < 150 mg/dl
 Blood Glucose <")
Know Your Diabetes, Metabolic Risk Fasting Diabetes Healthy Pre-Diabetes (Metabolic Syndrome) Blood Glucose < 110 mg/dl 110 -125 mg/dl ≥ 126 mg/dl 2 hr GTT < 140 mg/dl 140 -200 mg/dl > 200 mg/dl Triglyceride < 150 mg/dl > 150 mg/dl Typically elevated ≥ 60 mg/dl M < 40 mg/dl F < 50 mg/dl Typically low HDL

The Metabolic Syndrome Abdominal Obesity Men Women Triglycerides > 40 inch waist > 35 inch waist ≥ 150 mg/d. L HDL cholesterol Men Women < 40 mg/d. L < 50 mg/d. L Blood Pressure ≥ 130/ 85 mm Hg Fasting Blood Glucose 110 -125 mg/d. L
 Diastolic (mm/Hg) Normal 120 or less 80")
Know Your Blood Pressure Category Systolic (mm/Hg) Diastolic (mm/Hg) Normal 120 or less 80 or less High Normal 130 -139 85 -89 High Blood Pressure 140 or more 90 or more Strive for blood pressure of 120/80 or less
- Slides: 74