Limaging nella stratificazione prognostica dello scompenso cardiaco Gabriella

L’imaging nella stratificazione prognostica dello scompenso cardiaco Gabriella Locorotondo, MD Ph. D U. O. Diagnostica Cardiologica Non Invasiva Fondazione Policlinico Universitario A. Gemelli Roma
")
Does LV EF matter for risk stratification? Which risk? (arrhythmic / non-arrhythmic)
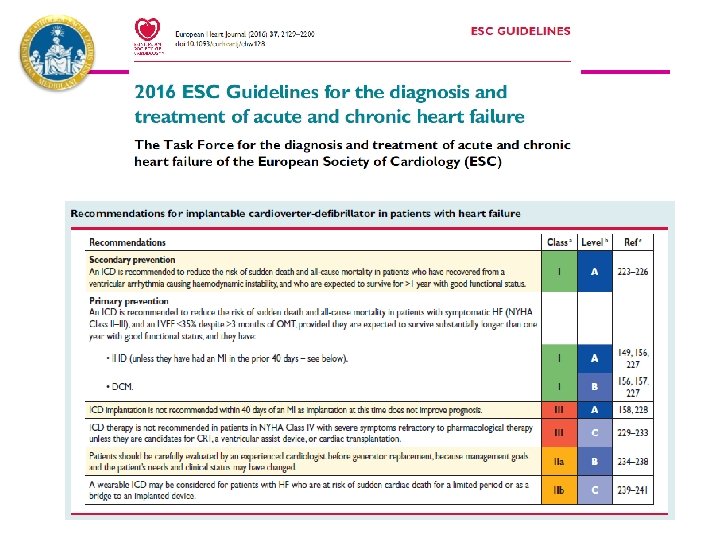

Benefit more for SCD in ischemic heart disease and NYHA II. In non-ischemic heart disease and NYHA class III no differences between ICD and placebo

CMR and myocardial fibrosis

Comprehensive Prognosis Assessment by CMR Imaging In Ischemic Heart Disease Eitel I, JACC 2014

Prediction of Life-Threatening Arrhythmic Events in Chronic Ischemic DCM Single-center prospective study in 52 pts with chronic ischemic DCM (> 40 days after MI), candidated to ICD implantation according to MADIT I and II criteria Boyè P, JACC Cardiovascular Imaging 2011

Should infarct size enter guidelines criteria? . . . Gaps in knowledge Boyè P, JACC Cardiovascular Imaging 2011

T 1 -mapping and Extracellular volume

Native T 1 Value in the Remote Myocardium Is Independently Associated With LV Dysfunction in Patients With Prior MI Nakamori S, J Cardiovasc Magn Reson 2017

58% in both group had CRT

CMR in non-ischemic DCM Gulati A, Pennell JD, Prasad S, JAMA 2013

Late Gadolinium Enhancement and the Risk for VAs or SCD in Non-ischemic DCM 2, 948 patients from 29 studies – Mean age 60 years - LVEFs: 20%-43% - Follow-up: 1 -5. 3 years Di Marco et al JACC Heart Failure 2017

Association Between Mid-Wall LGE and SCD in DCM and Mild-Moderate LV Systolic Dysfunction A LGE extent cut-off of >0% was the best discriminator of event-free survival time Halliday BP, Circulation 2017

Presence of Mid-Wall Fibrosis predicts efficacy of CRT-D vs CRT-P in Nonischemic Cardiomyopathy Leyva F, JACC 2017
 Prospective")
Cardiac Magnetic Resonance GUIDEd Management of Mild-moderate Left Ventricular Systolic Dysfunction (CMR_GUIDE trial) Prospective randomized, placebo-controlled trial of primary prophylaxis ICD therapy or implantable loop recorder insertion in patients with LVEF 36 -50% and LGE on CMR Controls: prospective observational registry of patients with LVEF 36 -50% and no LGE on CMR 1055 pts (700 in Australia and 355 in Germany and United Kingdom) Inclusion criteria: patients with CAD or non-ischemic cardiomyopathy (idiopathic, chronic post-myocarditis) on maximum tolerated doses of ACE inhibitors/ARBs and beta-blockers 36 months follow-up Primary end-point: SCD or VT leading to syncope Secondary outcome measures: SCD, syncopal VT, all-cause mortality, NYHA class, Qo. L, HF-related hospitalization, health economic evaluation costs Start Date: July 2015 Estimated completion date: March 2022 NCT 01918215

Role of GLS in HFp. EF Smiseth OA, Eur Heart J 2016

Extracellular Volume Fraction for Characterization of Patients With HFp. EF Rommel, JACC 2016

Interstitial Fibrosis, Functional Status, and Outcomes in HFPEF Duca F, Circ Cardiovasc Imaging. 2016

Prognostic value of stress E/e’ and PH Chi Young Shim, Heart 2011

Prognostic role of RV Dysfunction in HF: superiority of RV free waal strain over TAPSE Carluccio E, Circ Cardiovasc Imaging. 2018

Towards a personalized precision medicine

We must remember to treat the patient and not the disease or the echocardiogram Grazie per l’attenzione Gabriella Locorotondo, MD Ph. D U. O. Diagnostica Cardiologica Non Invasiva gabriella. locorotondo@policlinicogemelli. it

Impaired GLS and risk of SCD and non-sudden cardiac death Courtesy of Paiman EHM, Department of Radiology – Leiden University Medical Center, The Netherlands

T 1 mapping-based ECV independently predicts clinical outcome in non-ischemic DCM 117 patients Mean age 51. 9 Youn JC, Eur Rad 2017

Car. Diac Magn. Etic Resonance for Primary Prevention Implantable Cardio. Verter Defibrill. Ator Th. Erapy: an International Registry (DERIVATE) Multicenter prospective observational cohort study to: - determine CMR findings (LGE, T 1, ECV) that predict SCD and Vas - provide a comprehensive clinical and imaging score that effectively improves selection of patients who deserve a prophylactic ICD therapy. 4000 pts Inclusion criteria: patients with ischemic or non-ischemic DCM (LVEF < 55%) Target follow-up duration: minimum 12 moths Primary end-point: all-cause mortality Secondary outcome measures: SCD, HF death, sustained VTs, MACE, composite end-points Start Date: January 2010 Estimated completion date: March 2018 NCT 003352648

Predicting survival in heart failure by risk scores 39 372 patients from 30 studies (6 RCTs, 24 registries). 15 851 (40. 2%) patients died during a median follow-up of 2. 5 years http: //www. heartfailurerisk. org Pocock SJ, Eur Heart J 2013

GLS and ECV are independent diagnostic markers of HFp. EF Mordi, JACC Cardiovasc Imaging. 2017
- Slides: 29