LGBTQ Clinical Competence and Affirmative Services Cultural Humility

LGBTQ+ Clinical Competence and Affirmative Services Cultural Humility and Growth • Dr. Markus P. Bidell, Ph. D. , LMHC Associate Professor of Clinical Neuropsychology & Counseling – City University of New York & Hunter College mbidell@hunter. cuny. edu

Bernie! Feel the Burn in your Bern! https: //www. youtube. com/watch? v=XLveuzoau. Bo
 - A New Framework Institute of Medicine published:")
IOM Framework • IOM Report (2011) - A New Framework Institute of Medicine published: The Health of Lesbian, Gay, Bisexual and Transgender People • LGBTQ+ Competent Health and Mental Healthcare 1. 2. 3. 4. Minority Stress Life Course Intersectional Social Ecological Perspective IOM (Institute of Medicine). 2011. The Health of Lesbian, Gay, Bisexual, and Transgender People: Building a Foundation for Better Understanding. Washington, DC: The National Academies Press. http: //www. nationalacademies. org/hmd/ Reports/2011/The-Health-of-Lesbian-Gay-Bisexual-and. Transgender-People. aspx

Social Ecological Perspective • Who are we serving? • Can we can think individually and collectively? • What kinds of data do we have?

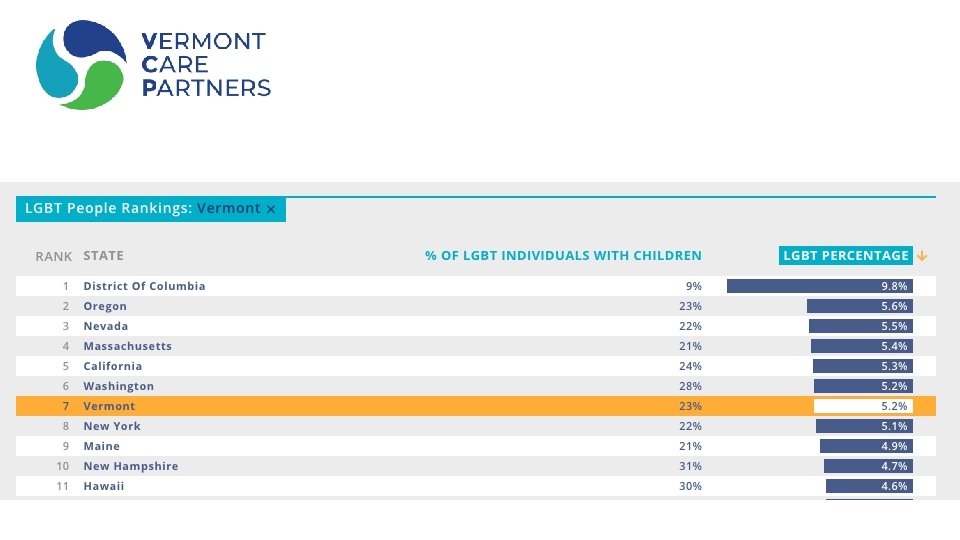
WE ARE EVERYWHERE There are more than 9 MILLION LGBTQ people in the United States. It’s fair to assume you see LGBTQ people regularly.

VT • https: //williamsinstitute. law. ucla. edu/visualization/lgbt-stats/? topic=LGBT#density

LGBT Population Data
 Acronym Acrobatics. Columbia Magazine. http: //magazine. columbia. edu/features/summer-2016/acronym-acrobatics")
Retherford, B. (2016) Acronym Acrobatics. Columbia Magazine. http: //magazine. columbia. edu/features/summer-2016/acronym-acrobatics

SOGI Sexual Orientation & Gender Identity Gender Biological Sex Gender Identity Gender Expression Sexual Orientation Behavior Attraction Identity

Gender identity The persistent internal sense of being a man or a woman or some other gender. • We all have a gender identity • For cisgender people, this gender identity matches the sex assigned at birth Transgender people have a gender identity that does not match the sex assigned at birth. • Our gender identity may or may NOT match our appearance, our body, or others’ perceptions of us

• “About 1. 4 million adults in the United States identify as transgender, double a widely used previous estimate” (NYT, June 30, 2016) AJPH 2017: Transgender Population Size in the United States 1+ Million and Growing (Esther L. Meerwijk and Jae M. Sevelius)

Key Gender Terms • cisgender: a person whose gender identity is the same as or similar to their sex assigned at birth. • transgender: a person whose gender identity is different from their sex assigned at birth (umbrella term). • gender-nonconforming: a person whose gendered expression is somehow different from what is traditionally expected of their biological /assigned sex and/or gender identity. • Non-binary: A person who identifies as neither male nor female. NB people usually use they/them pronouns, but some may choose neopronouns like ze/zir or hir.

DEFINING OUR TERMS Sexual Orientation Behavior Attraction Identity

BEHAVIOR VS. IDENTITY 9. 4% of men who identified as “straight” had sex with another man in the prior year. They were more likely to… • Belong to minority racial/ethnic groups • Be of lower socio economic status • Be foreign born • Not use a condom 77 -91% of lesbians had at least 1 sexual experience with men 8% in the prior year

WHERE DO YOU FIT? Biological Sex Male Female intersex/DSD Attracte d to women Masculine Man Sexual Orientation attracted to both Gender Expression Attracted to men Feminine androgynous Gender Identity genderqueer/two spirit/third gender Woman

LGBT Glossary • To download a glossary that defines other LGBT terms, click here or go to: • http: //www. lgbthealtheducation. org/wp-content/uploads/LGBTGlossary_March 2016. pdf

Minority Stress • Chronically high levels of stress faced by members of stigmatized minority groups • SOGI health disparities explained by stress - stigmatization, bias, & oppression • The most well understood causes of minority stress are interpersonal prejudice & discrimination (IOM, 2011; Marshal et al. , 2008; Meyer, 2003; 1995; Mirowsky & Ross, 1989; Pearlin, 1989)

Intersectionality • Feminist Theory & bell hooks • “challenged the notion that 'gender' was the primary factor determining a woman's fate”* • Interlocking Systems Stratification • SES, Ethnicity/Race/Skin Color, SOGI, Disability, Religion, Immigration Status, etc… • Systemic whole – the totality of the person • Oppression of women of color initial focus, can be applied to all social categories (including those seen as dominant when considered independently) • Our stories are ‘socially mediated’ *hooks, bell (2014). Feminist Theory: from margin to center (3 rd ed. ). New York: Routledge. ISBN 9781138821668

country of origin Seen and Unseen Identities age gen iden der tity race sex Public Identities clas s caree r Health / ability Unseen. Identitie s religio n politics ge expnde res r sio ethnicity n

Stigmatization • Barriers to accessing high-quality care is personal & structural • Personal-level barriers are created by the attitudes, beliefs, & behaviors of individuals within the health care system—both providers and patients; Implicit or Unconscious Bias • Structural-level barriers are created at the macro or institutional level (restrooms, intake forms, policies, magazines ordered for waiting rooms, etc…)

Health & Mental Health Disparities 1. Mood, Anxiety, Eating, Substance Abuse Disorders (SUD, MDD, GAD, PD, PTSD/ASD) 2. Health Complications from Alcohol/Tobacco/Other Drugs 3. Certain Cancers 4. Certain Behaviors and Health Consequences

DATA on LGBT Minority Stress 1. Same-sex individuals 2 X as likely as heterosexuals to have experienced discrimination in their lifetime 2. 5 X more likely to indicate that discrimination had interfered with having a full and productive life 3. Perceived and actual discrimination correlated with mental disorders 4. Racial microaggressions were found to predict various types of physical health conditions, such as general health problems, pain, lower energy levels, and fatigue 5. Can result in higher levels of psychiatric symptoms anxiety, depression and burnout; and higher morning cortisol levels Kevin L. Nadal, Katie E. Griffin, Yinglee Wong, Kristin C. Davidoff & Lindsey S. Davis (2016) The Injurious Relationship Between Racial Microaggressions and Physical Health: Implications for Social Work, Journal of Ethnic & Cultural Diversity in Social Work, 26: 1 -2, 6 -17, DOI: 10. 1080/15313204. 2016. 1263813 Meyer, I. (2003) Prejudice, Social Stress, and Mental Health in Lesbian, Gay, and Bisexual Populations: Conceptual Issues and Research Evidence. Psychol Bull. 2003 September; 129(5): 674– 697.

Addressing Minority Stress • Trigger for Trauma • Health Risk Factor • Behavioral Risk Factor • Assisting Patients to Understand Mediate the Impact of Minority Stress

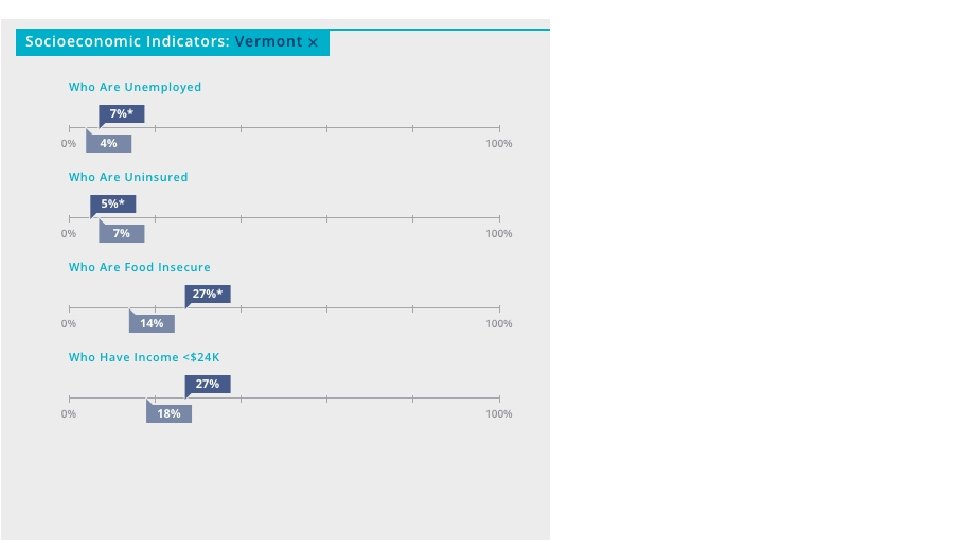
Lifespan Approach & Developmental Context Youth and Adolescents Later Adulthood and Seniors Adulthood https: //www. cdc. gov/lgbthealth/index. htm https: //www. ncbi. nlm. nih. gov/pmc/articles/PMC 5478215/ https: //www. kff. org/report-section/health-and-access-to-care-and-coverage-lgbt-individuals-in-the-us-health-challenges/

OVERVIEW OF LGBTQ WELL BEING LGBTQ people report lower “well being” in five areas: FINANCIAL SECURITY PHYSICAL HEALTH SENSE OF PURPOSE SOCIAL LIFE COMMUNITY 2014 Gallup Poll ATTACHMENT

WHO ARE LGBTQ ELDERS? There are 3 million LGBTQ older adults in the U. S.

LGBT Elders • At higher risk for the previously reviewed health and mental health concerns • Higher levels of depression and suicidality • Social isolation and discrimination (Nursing Home Care) • Increased rates of HIV infection for older gay men and transgender women • Long-term impacts of minority stress and discrimination

• Lesbian & bisexual women report poorer overall physical health Lesbian, Gay and Bisexual Adults • Lesbian and bisexual women report heightened risk for and diagnosis of some cancers and higher rates of cardiovascular disease • Gay men remain at higher risk of HIV and other STDs, especially among communities of color; higher rates of cancer • Bisexual women are more likely to be overweight or obese Transgender/Non-Binary Adults • Transgender women, particularly of color, have a significantly high prevalence of HIV/STDs • Higher rates of violence, mental health issues, and suicide and • Less likely to have health insurance and access to transgender competent care than heterosexual or LGB individuals

• Increased risk of physical health problems and a lack of LGBT informed health care • 2 to 3 times more likely to attempt suicide LGBT Youth • LGBT youth are more likely to be homeless • Higher rates of violence: • including having been threatened or injured with a weapon, been in a physical fight, or injured in a fight • 60 -70% report feeling unsafe at scholl
 Event Occurs Behavior/Identity Earlier Studies* More")
SEXUAL IDENTITY: AGE OF ONSET Average Age (Years) Event Occurs Behavior/Identity Earlier Studies* More Recent Studies** Males Females 13 14– 16 Males Females 9 10 First same- sex experience 15 13– 14 14– 15 First self- identified as lesbian or gay 19– 21 21– 23 14– 16 15– 16 First awareness of same-sex attraction 20 *Studies of adults who remembered their experiences as children and adolescents **Studies of adolescents who described their experiences as they were happening or right after they happened

Video - CBS

Violence 23 Year High Video - CBS https: //www. wcax. com/video? vid=505330492

Violence Video - CBS

LGBTQ+ Policies & Best Practices

10 Things to Discuss with your Health Provider Gay/Bisexual Men 1 Lesbians/Bisexual Women 2 Transgender 3 Come Out to your Healthcare Provider Breast Cancer Access to Healthcare HIV/AIDS, Safe Sex Depression/Anxiety Health History Hepatitis Immunization & Screening Heart Health Hormones Diet and Exercise Gynecological Cancer Cardiovascular Health Substance Use/Alcohol Diet & Exercise Cancer Depression/Anxiety Tobacco Alcohol and Tobacco STDs Alcohol Depression Prostate, Testicular, and Colon Cancer Substance Use Injectable Silicone Tobacco Intimate Partner Violence Alcohol and Tobacco HPV Sexual Health Diet & Exercise 1 Tonia Poteat, MMSc, PA-C, MPH, Ph. D. Revised May 2012. J Winn, MD AAHIVM. Medical Director, Mazzoni Center. Philadelphia, PA. Revised May 2012. 3 Rebecca A. Allison, MD. Board of Directors, GLAMA. Revised May 2012 2 Robert

Best Practices in Clinical Care for LGBTQ Patients • Open ended questions • Know health/mental health needs and issues • Know terminology • Know about stigma and minority stress • Know that LGBTQI+ people are also people • Consider appropriate screenings • Take a sexual history • Awareness and assistance with impact of minority stress, unconscious bias, micro aggressions, family and partner issues

Using Open Ended Questions “How do you describe your sexual orientation? ” • Asking separately from sexual practice will help strategize for counseling conversations about risk reduction “How do you describe your current gender identity? ” • This question may start a conversation with the client about their medical history around transition “What are the genders of your sexual partners? ” • This question will also start a conversation about sexual practice “What is the sex on your original birth certificate? ” • This question helps elicit further gender history, though you will hopefully already know the answer from earlier discussions

Taking a History • Family – Relational - Sexual • Ask open ended questions with gender neutral language • Be prepared for lots of different answers! Too Often, LGBTQ Clients do not Come-out to Their Providers or do not Return After Initial Appointments Gelman et al. Principles for Taking an LGBTQ-Inclusive Health History and Conducting a Culturally Competent Physical Exam. In: Fenway Guide to Lesbian, Gay, Bisexual, and Transgender Health. 2 nd ed. Philadelphia: American College of Physicians; 2015.

What is Unconscious Bias? Mental associations w/out: • Awareness • Intention • Control These often conflict with our conscious attitudes, behaviors, and intentions.

If you make a mistake… Apologize! • Clearly, it is not always possible to avoid making mistakes, and simple apologies can go a long way. • If you do slip, you can say something like: “I apologize for using the wrong pronoun/ name. I did not mean to disrespect you. ”
 Collecting SOGI Data LGBT Brochures")
Systemic Changes Developing Policies, Trainings, and Practices (Posting Them) Collecting SOGI Data LGBT Brochures and Literature Gender Neutral Bathrooms and Changing Rooms Wearing Something LGBTQ+

Collecting SOGI Data • Gathering SOGI data • • • Understand, target, & reduce LGBTQ health disparities Healthy People 2020, IOM, Joint Commission recommends Help track health outcomes in the LGBT population Help inform interventions to reduce LGBT health disparities Helps us know our clients/patients • Hesitant to disclose information about sexual orientation or gender identity due to fears about confidentiality and privacy

Collecting SOGI Data Example 1: • What is your gender identity? ☐ Male ☐ Female ☐ Transgender man / Transman ☐ Transgender woman / Transwoman ☐ Genderqueer / Gender nonconforming ☐ Additional identity (fill in) _______ ☐ Decline to state • What sex were you assigned at birth? ☐ Male ☐ Female ☐ Decline to state Example 2: • Do you think of yourself as ☐ Lesbian, Gay or Homosexual ☐ Straight or Heterosexual ☐ Bisexual ☐ Something else ☐ Don’t Know

Vanessa Goes to the Doctor https: //www. youtube. com/watch? v=S 3 e. DKf 3 PFRo
 • Sally is a 42 year old")
Case Examples Case 1 Bullying Assessment (Video) • Sally is a 42 year old Lesbian who identifies as cisgender and is having severe anxiety and depression symptoms, especially related to her work. She is a librarian at a local community library and there are major budget cuts and she feels people want her to be let go. Case 2 Lesbian Couple (Story. Corps) • Bobbi and Sandi Cote-Whitacre have been together for nearly 40 years and were married 5 years ago. Bobbi is part Native American and Sandi identifies as white and both are cisgender(ish). Sandi has been recently diagnosed with pancreatic cancer. Case 3 Assessing Minority Stress (Video) Suzie is a 51 year old African American Queer and does not identify as totally cisgender. She has had very negative experiences regarding health and mental healthcare services. She has 4 other siblings and her mother just diagnosed with lung cancer and has a very negative prognosis. Suzie is experiencing a lot of sadness and has a Hx of alcoholism.
 • Madison and her mother are")
Case Examples Cntd’ Case 1 Family Counseling (Video) • Madison and her mother are attending a family counseling session. Joe is working on her undergraduate college degree and has just come out as queer to her mom. She is concerned about how this will impact her family and their support. She has been very anxious about this situation. Case 2 Trans Couple (Story Corp) • Vickie and Sissy Goodwin live in a rural part of Vermont and have been married over 46 years. Vickie is 64 and Sissy is 65, both identify as White. They have been dealing with Sissy’s consideration of starting hormones and possibly having feminization surgery. They have worked on Sissy’s wearing women’s clothes, but now Sissy is identifying as female. Case 3 & Case 4 Daniel (Video) • Daniel is 17 and having problems in high school. She is struggling with her sexuality and has started to use alcohol and drugs. Her academic performance is problematic and her parents wanted her to seek counseling. She identifies as White and as cisgender. Case 5 Joe (Video) Joe is a 48 y. o. gay male originally from Ireland. He tested positive for HIV about twenty years ago and his partner died of AIDS in the early 90 s. He has a history of substance abuse disorder. He is having a ‘mid-life’ crisis.
- Slides: 48