Leschs Typology for AUDs Tim Robinson LPC CPCS

Lesch’s Typology for AUDs Tim Robinson LPC, CPCS, CAS-F LPCA CONVENTION 5 -11 -2018 678 -237 -1530 supervisionrobinson@yahoo. com

Expectations and Take Homes Please silence cellphones. If you must leave, please be discrete. Speak up If you can’t hear me. Interrupt me at any time. Understand the typologies of AUDs. Identify how they can benefit you. Gain an understanding of biology, medication and therapy

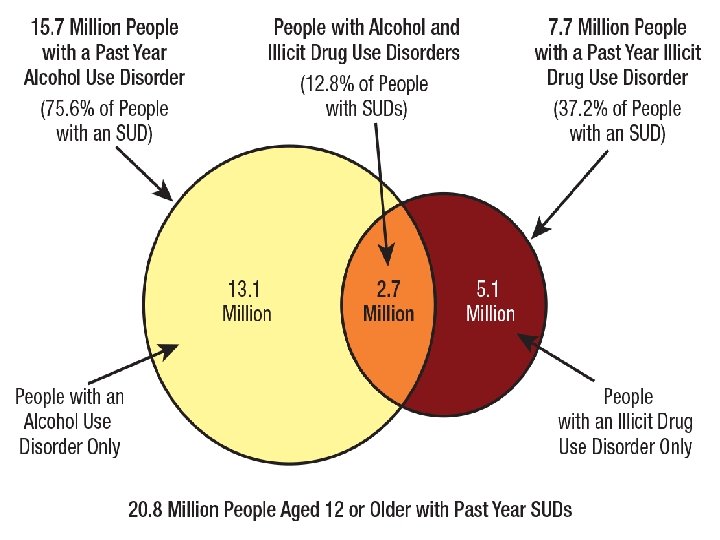
“most used intoxicating substance in US. 82% of people age 12 and older have used at least once. Nearly half have used in past month. ” 1 WHO

Why Type Individuals ? 18 Get at etiology, familial, environmental and mental health factors that may shed light on the development of the disorder and that can play a role in determining the severity of the disorder, the levels of care and effective treatments. This has been done with Alcohol Use Disorders since 1960. No two individuals are alike and not all treatments work for all clients-and all work for some. Treatment matching.

Predisposing Factors for Developing AUD 2, 3 Genetics. Environment. Age of first use. Adverse childhood experiences. Mental health issues.
. Environmental exposures and social context. Symptom")
Typing Should Address Etiology. Family history (genetic etiology). Environmental exposures and social context. Symptom profiles. Psychological or Psychiatric comorbidities. Treatment and relapse.
 3. Twin studies 4. Adoption")
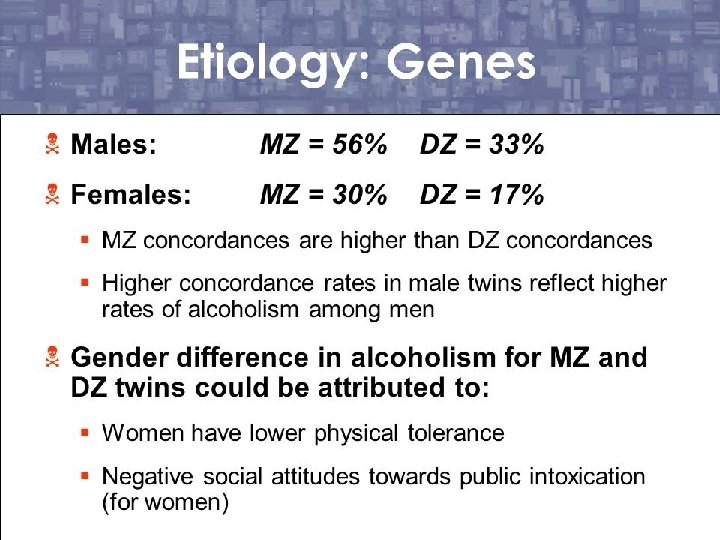
Genetics 2 1. Animal models 2. Family pedigree (Caution) 3. Twin studies 4. Adoption studies 5. Ethnicity-good example of environmental role Genetics have been cited to play a role in the genesis of AUDs in the range of 40 -60 % ACOA

Stress and Drug Use The use of alcohol, cigarettes and cannabis increased among Manhattan residents after the 9/11 attacks. Vlahov et al. reported that 3. 3 % of the population started smoking, 19. 3 % drank that week but not the week before, 2. 5 % started Cannabis 19.

Oklahoma City bombing, 1995 34% of survivors had PTSD 4 -8 months later 63% of those with PTSD also had a comorbid condition 32% drank alcohol to cope. Of those with a non-PTSD diagnosis 40% drank alcohol to cope. 27% took medications.

Biology/genes Biology/ Environment Interactions Environment
 demonstrated that abuse and high levels")
Adverse Childhood Experiences The ACE study (n=17, 000) demonstrated that abuse and high levels of stress in adolescence predicted the development of several disorders, including substance use disorders. 3, 14 Age of first use plays a role in developing an Alcohol Use Disorder.

Prevalence of Lifetime Alcohol Dependence by Age of First Alcohol Use and Family History of Alcoholism: Have Drug Talk

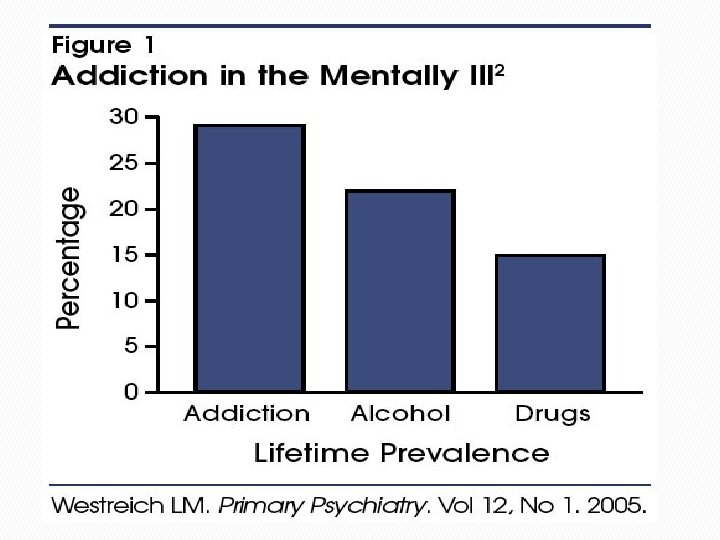
Psychiatric Co-Morbidity Data collected since the 1980’s demonstrates the high instance of co-morbidity…“persons diagnosed with mood or anxiety disorders are about twice as likely to suffer also from drug use disorder (abuse or dependence) compared with respondents in general” Dr. Volokow 4. Intoxication and withdrawal from alcohol can mimic other disorders. Disorder may precipitate SUD or SUD precipitates D/O.

Gender Differences 5, 16 Women become more intoxicated than men from drinking the same amount of alcohol. This is due to the gastric process of enzymes in mens’ stomachs, not because women have a higher fat to water ratio. Physical and other problems occur more quickly once women begin problem drinking: “telescoping effect. ” When they quit, they heal faster.

Gender and Anxiety 6 2014 Female Males Female: Male Panic 6. 2% 3. 1% 2. 0 Generalized Anxiety 7. 1% 4. 2% 1. 7 Any Anxiety Disorder 36. 4% 25. 4% 1. 4 PTSD 9. 7% 3. 6% 2. 7

Depression and AUD 6 2014 Female Males Female: Male Major Depression 20. 2% 13. 2% 1. 5 Any Affective Disorder 24. 4% 17. 5% 1. 4 Alcohol Abuse 7. 5% 19. 6% 0. 4

Jellinek Typology 19607 Alpha-psychological in nature, may not lead to Dependence. Beta-continual heavy drinking leads to physical problems. Gamma-classic loss of control pattern. Delta-inability to stop and drinks to avoid withdrawal. Epsilon-binging and episodic pattern.

Cloninger et al. Typology 19818 Type I Mild to severe alcohol use. Relatively high socioeconomic status. Maternal alcohol use. No criminality among fathers. More restricted by environmental influence. Relatively mild alcohol problems. Late age of onset (greater than 25 years).

Cloninger et al. Typology Type II Positive family history of alcohol use. Severe alcohol problems. Other drug use. Early onset (less than 25 years).

Babor: Type A 19929 Late age of onset. Fewer behavior problems in childhood. Less Psychopathology.

Babor: Type B Behavior problems in childhood. Greater Psychopathology. Positive history of family alcohol use. Early onset of alcohol problems. Greater life stress.

Lesch’s Typology A strong emphasis is placed on biological factors, such as medical and psychiatric conditions. This includes withdrawal, medication and treatment. Suggestions for treatment and relapse prevention are offered in the model proposed by Lesch. It is also being tested with Cocaine and Opiates. His model meshes well with Cloninger’s model. Widely used in Europe and spreading globally.

Experts Endorse Lesch Typology 10, 11 Their exceptions: he should lump all psychiatric together and substitute a mildly affected long term course, low etiology. Lesch has discussed adding another type due to findings in other countries: early multiple drug dependence 12. His work has yielded a free, computerized diagnostic tool: http: //www. lat-online. at/

Lesch Typology I Alcohol adaptation to avoid withdrawal 14 Severe withdrawals. Seizures during withdrawal. Severe craving. Alcohol is used to avoid detox.

Lesch Type II Psychiatric-self medicating anxiolytic 14 Mild withdraw symptoms. No seizures. No suicidal ideation. Alcohol is used to ameliorate anxiety.

Lesch Typlology III Psychiatric-self medicating depression 14 Major Depression. Preponderant female. Trouble with sleep. Suicidal ideations independent of alcohol use or withdrawal. Individual drink to self regulate depression.

Initiation and continuation of drinking Initiation of Drinking Social Drinking Alcoholic Drinking Extent of Influence Environmental (familial and non familial) Personality/Temperament Pharmacological effects of ethanol

Lesch Typology IV Organic damage and to cope with environment 14 Cerebral compromise before age 14. Mostly male. Behavioral disturbances in childhood: enuresis, nail-biting, fluency disorder. Cognitive Impairment-prior to dependence, conditioning. Drink to cope with environment and impulses.
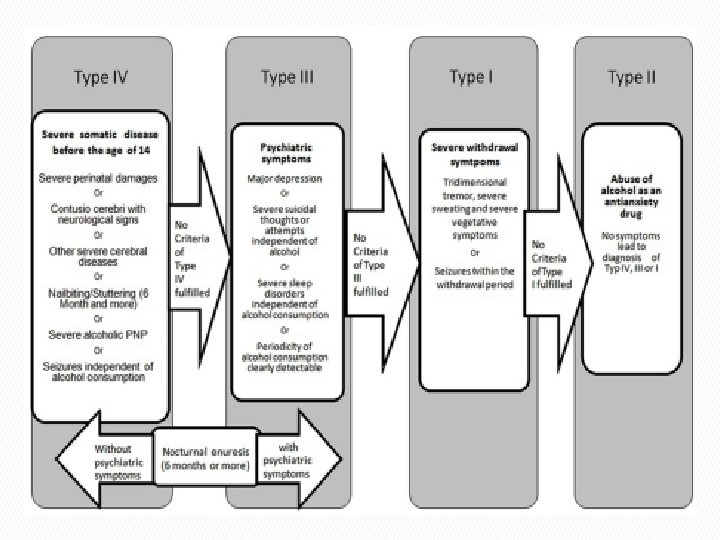

“This decision tree assesses multidimensionally four different subgroups. If a symptom of Type IV can be found then the patient has to be defined as Type IV. If there are no symptoms of Type IV but the patient has an affective disorder or suicidal behavior independent from alcohol intake or withdrawal, this leads to the diagnosis of Type III. If there are no symptoms of Types IV and III, but there are severe withdrawal symptoms or withdrawal seizures then Type I has to be diagnosed. Type II patients, consuming alcohol to cope with states of anxiety, do not show any symptoms of Type IV, III or I. ” 21 p. 536

Relapse and Detox Readmissions 12 Over 24 months, 54% of the female patients and 67% of the male patients were re-admitted. The kindling effects were stronger in patients with age at onset of alcohol dependence over 25 years. The Cloninger type 2 profile and the Lesch I typology represented the most significant predictors.

Lesch Relapse Course 13, 17 I-Total abstinence or acute relapse-focus on health and biology-use relapse prevention. Often a good outcome. II-Long periods of abstinence, occasional short lapses without loss of control or harm-motivational interviewing. III-Reduce frequencies of severe use that can lead to changes in personality traits-symptom relief. IV-Severe relapses-intervene by strengthening coping skills, improve environment, need good social support.

Lesch Relapse Prevention 25 Type I: Medication, self help groups, Relapse Prevention. Type II: Medication, Stress reduction, ego strengthening. Type III: Medication, CBT, enhance emotional intelligence. Type IV: Medication, Psycho ed, Relapse Prevention, self help, conditioning, sober living.

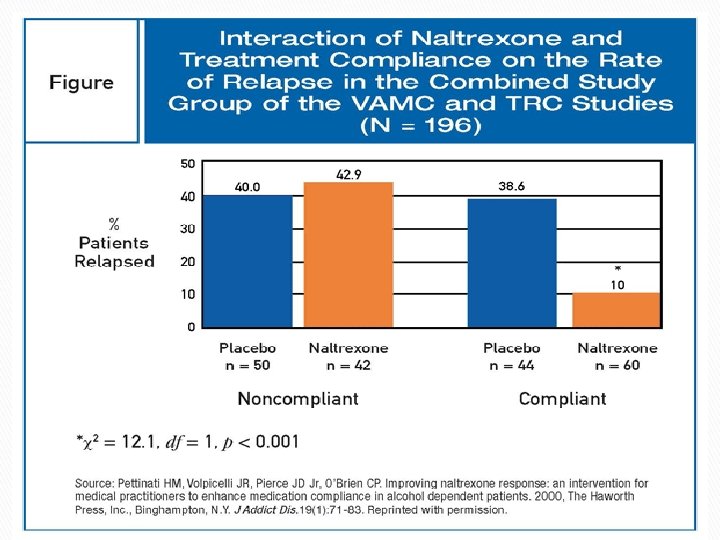
Lesch Relapse Prevention 11, 14, 17 Type I: Campral, Antabuse, self help group. Type II: Campral, focus on coping, not group (Benzo). Type III: Naltrexone, therapy, not group (Topamax, SSRI). Type IV: Naltrexone, self help group (Seroquel). Does not recommend combining Campral and Naltrexone.

Treatment Lesch does not recommend substance abuse counseling other than 12 -step facilitation for type I and IV only 14. He does argue that relapse prevention (CBT)16 psychotherapy and a systems approach be used. Other groups: SMART Recovery, Life. Ring, Women for Sobriety, Celebrate Recovery. Other authors have made recommended specific therapies for treating these types based on research outcomes. We will look first at what Lesch suggests.

Treatments 10 Motivational Interviewing first for all. Psychiatric-Pharmacotherapy, II and III. Relapse Prevention Medication all. Type I, IV 12 step Facilitation-no “Near Beer” =Craving 17 Also, Solution Focused, Behavioral Self-Control Training, Relapse Prevention, Support Group

Other Treatment Modalities Goals of treatment: commitment to abstinence, medication management, develop social support (identify threats), symptom relief, drink refusal, and replacement activities 14. There are 99 substance abuse treatments worldwide and most are not evidence-based. 16 Types II and III can benefit from CBT, DBT, Solution Focused, Stress Management, ACT, Motivational Interviewing, and Schema therapy 11, 14
 1951: Adverse reactions with alcohol through aldehyde")
Relapse Prevention Medications FDA Approved Antabuse (Disulfuram) 1951: Adverse reactions with alcohol through aldehyde dehydrogenase, short term use, observed use, may have dopamine effects, liver complications. 22 Revia, Vivitrol (Naltrexone) 1994, 2006: Works in the opiate system as an antagonist, endorphin effects, drinking less pleasurable, warning for use of opiates, nausea. 22 Campral (Acamprosate) 2004: Gaba and Glutamate systems to reduce post acute withdrawal: insomnia, anxiety, restlessness, and dysphoria. 22 Sinclair Method.
: Suspected to work on the dopamine system, in")
Non FDA Approved Medications Topamax (Topirmate): Suspected to work on the dopamine system, in clinical trials for over ten years, is recommended by the National Institute on Drug Abuse. 22 Baclofen: A muscle relaxer, acts in Gaba and Glutamate systems to reduce post acute withdrawal: insomnia, anxiety, restlessness, and dysphoria, side effect of drowsiness. Widely used in Europe and works well. 21, 23 Any meds used for less than 18 months

Application Understand use medications. Learn to see how your clients differ and what treatments can be effective for whom. Use this theory to guide treatment, Cloninger too.

Circuits Involved In Drug Abuse and Addiction All of these must be considered in developing strategies to effectively treat addiction
. Rethinking Drinking. Retrieved from:")
REFERENCES 1. National Institute on Alcohol Abuse and Alcoholism (2009). Rethinking Drinking. Retrieved from: https: //www. niaaa. nih. gov/news-events/news-releases/rethinkingdrinking-offers-tools-assess-and-change-risky-drinking-habits 2. Erickson, C. K. (2007). The science of addiction: From neurobiology to treatment. New York, NY: W. W. Norton & Company. 3. Wilson, K. G. (2017). The other book addiction: A thinking disease. Amazon Books. 4. National Institute of health and human services. Comorbidity: Addiction and other mental illnesses. NIH publication number 10 -5771. 2008 5. Brigs, C. A. (2008). Gender and addictions. In Capuzzi, D. & Stauffer, M. D. (Eds. ), Foundations of addiction counseling (331 -347). New York, NY: Pearson. 6. Bangasser, D. A. , & Valentino, R. J. (2014). Sex differences in stress-related psychiatric disorders: Neurobiological perspectives, Frontiers in Neuroendocrenology, 35(3), 303 -319. 7. Jellinek, E. M. (1960). The disease concept of alcoholism. Brunswick NJ: Hillhouse Press. 8. Cloninger C. R. , Bohman M. , Sigvardsson S. (1981). Inheritance of alcohol abuse: cross-fostering analyses of adopted men. Archives of General Psychiatry. 38: 861– 8.

9. Babor T. , De Hoffman M. I. , Boca F. , Hesselbrock V. , Meyer R. , Dolinsky Z. et al. 1992 Types of alcoholics. I. Evidence for an empirically derived typology based on indicators of vulnerability and severity. Archives of General Psychiatry, 49, 599 -608. 10. Kogojo, D. , Addoloratto, G, . Ferrulli, A. , Mouzas, I. , Okruhlica, L. , Poldugro, F. A. , …Walter, H. (2011). Alpe Adria report: Conclusions and recommendations for the treatment of alcohol dependence. Frontiers in Psychiatry, 2(58), 1 -6. 11. Schlaff, G. , Walter, H. , Lesch, O. M. (2011). The Lesch alcoholism typology: Psychiatric and psychosocial treatment approaches. Annals of Gastroenterology, 24(2): 89– 97. 12. Weinland, C. , Braun, B. , Muhle, C. Kornhuber, J. , Lenz, B. (2017). Cloninger type 2 score and Lesch typology predict hospital readmission of female and male alcoholdependent inpatients during a 24 -month follow-up. Alcoholism: Clinical and Experimental Research 41(10): 1760 -1767. 13. Kogoj, D. , Lesch, O. M. , Bluml, V. , Reigler, A. , Vyssoki, B. , Schlaff, G. , Walter, H. (2010). Lesch alcoholism typology medical treatment and research. Archives of Psychiatry and Psychotherapy, 4, 37 -48. 14. Lesch, O. M. , Walter, H. , Wetschka, C. , Hesselbrock, M. , Hesselbrock, V. (2011). Alcohol and tobacco: Medical and sociological aspects of use, abuse and addiction. New York, NY: Springer Wein New York.
. The alcoholic pheno-types among different")
15. Pombo, S. , and Lesch, O. M. (2009). The alcoholic pheno-types among different multidimensional typologies: similarities and their classification procedures. Alcohol and Alcoholism, 44, 46– 54. 16. Hester, R. K. & Miller, W. (Eds. ), In Handbook of alcoholism treatment approaches: Effective alternatives. New York, NY: Allyn and Bacon. 17. Relapse rates Connors, G. J. , Donovan, D. M. , Clemente, C. C. (2001). Substance abuse treatment and the stages of change: selecting and planning interventions. New York, NY: Guilford Press. 18. Pombo, S. , and Lesch, O. M. (2009). The alcoholic pheno-types among different multidimensional typologies: similarities and their classification procedures. Alcohol and Alcoholism, 44, 46– 54. 19. Vlahov, D. , Galea, S. , Resnick, H. , Ahern, J. , Boscarino, J. A. , Bucuvalas, M. . . Kilpatrick, D. (2002). Increased use of cigarettes, alcohol, and marijuana among Manhattan, New York, residents after the September 11 th terrorist attacks, American Journal of Epidemiology, 155: 988 -96. 20. North, C. S. , Nixon, S. J. , Shariat, et al (1999). Psychiatric Disorders Among Survivors of the Oklahoma City Bombing, Journal of the American Medical Association, 282(8): 755 -762.

21. Vyssoki, B. , Steindl-Munda, P. , Ferenci, P. , Walter, H. , Höfer, P. , Blüml, V. , …Lesch, O. M. (2010). Comparison of Alcohol-dependent Patients at a Gastroenterological and a Psychiatric Ward According to the Lesch Alcoholism Typology: Implications for treatment, Alcohol and Alcoholism, 45(6), 534– 540. 22. National Institute on Drug Abuse. Principles of Drug Addiction Treatment: A Research-Based Guide (3 rd Ed. ), Author. 23. Addolorato, G. , Leggio, L. , Ferrulli, A. , Cardone, S. , Vonghia, L. , Mirijello, A. , . . Gasbarrini, G. (2007). Effectiveness and safety of baclofen for maintenance of alcohol abstinence in alcohol-dependent patients with liver cirrhosis: randomised, double-blind controlled study, The Lancet, 370(9603), 8 -14. 24. North, C. S. , Nixon, S. J. , Shariat, et al (1999). Psychiatric Disorders Among Survivors of the Oklahoma City Bombing, Journal of the American Medical Association, 282(8): 755 -762. #IOP Slide Treatment Outcomes among Clients Discharged from Intensive Outpatient Substance Abuse Treatment: 2005 TEDS report 2009 #Slide age first drink and Family History NIAAA 2005 #Alcohol % wheel Substance Abuse and Mental Health Administration (2003). Substance abuse in brief. Author
- Slides: 52