LEPROSY Leprosy Chronic infectious disease caused by the


LEPROSY

Leprosy � Chronic infectious disease caused by the Mycobacterium leprae bacilli with predilection for peripheral nerves and the skin � The bacillus M. leprae is a very small, slightly curved acid-fast rod. It is an obligate intracellular microorganism, that lives within cells, particularly macrophages and Schwann cells.

The bacillus requires a temperature of ~35°C to grow, and thus has a preference for cooler regions of the body (e. g. the nose, testicles and ear lobes) as well as regions where the peripheral nerves are close to the skin � It cannot grow on artificial media , but it can be cultivated in mice footpads and in armadillo. �

Mode of transmission Droplet infection: nasal secretion � Rare and unlikely route : skin contact �

The clinical-immunologic spectrum of leprosy It depends upon the level of specific cell-mediated immunity : Ø Tuberculoid: in patients with intact cell-mediated immunity Ø Lepromatous: in patients with depressed cellmediated immunity Ø three types of borderline leprosy in between: borderline lepromatous , borderline-borderline and borderline tuberculoid �
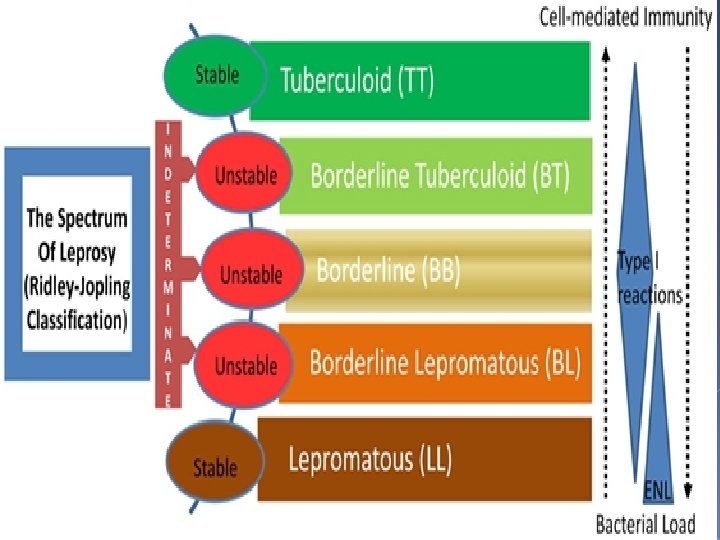

Clinical picture: tuberculoid leprosy: Ø The lesions are limited to nerves and skin Ø cutaneous lesions : single or few well defined erythematous or hypopigmented plaques , The borders of the skin lesions are often slightly elevated Ø The cutaneous lesions have impaired sensation and devoid of hair and do not sweat �

Clinical picture: � tuberculoid leprosy: Ø Peripheral nerve affection: unilateral and/ or asymmetrical occuring early in the disease Ø there is thickening of the peripheral nerves with pain , paresthesia , muscular weakness or paralysis Ø sometimes only neural involvement is present

Clinical picture: � Lepromatous leprosy: Ø It is characterized by multiple, poorly defined, erythematous macules, papules, nodules and plaques. Ø Lesions are widespread, and symmetric in distribution

Clinical picture: Lepromatous leprosy: Infiltration of the skin of the forehead can lead to a leonine face Ø Peripheral nerve affection: bilateral and symmetrical occuring late in the disease , Anesthesia in a stocking or glove distribution may be seen, muscle wasting and atrophy, neurotrophic ulcers, bone resorption and loss of digits � Ø

Clinical picture: � Lepromatous leprosy: madarosis, nasal bleeding , saddle nose, bilateral infiltration of the earlobes and acquired ichthyosis of the lower extremities Ø Corneal ulcers, keratitis, orchitis. Ø

Clinical picture: Borderline leprosy: The features are intermediate between the two ends of the spectrum Ø cutaneous lesions : few or several asymmetrical erythematous partly well defined plaques which usually have annular appearance Ø Peripheral nerve affection: several and asymmetrical � Ø

Leprosy reactions : � � � As a result of the conflict between M. leprae and immune system. Spontaneous or Precipitated by treatment, pregnancy, other intercurrent infection. Sudden change in the clinical picture of the disease Type 1–Reversal reaction (upgrading): mostly in borderline leprosy , Type IV delayed-type hypersensitivity reaction, acute onset with erythematous and edematous changes in old lesions with tenderness and swelling of the nerves Type 2–Vasculitis : (most commonly erythema nodosum leprosum): mostly in lepromatous leprosy or borderline lepromatous leprosy, Immune complexes small vessel vasculitis , acute onset of fever , malaise and arthralgia with bilateral symmetrical erythematous nodules on the face and extremities

Investigations � Ø Ø Slit skin smear : mainly from the earlobes To avoid bleeding, a fold of skin is firmly squeezed between the finger and thumb of the examiner and a small incision is made with a scalpel blade. The liquid obtained is smeared onto a slide and allowed to dry. The smear is usually stained by the Fite (or Ziehl-Neelsen) method and a search is made for red rods (against a blue background)

Investigations � Ø Ø Skin biopsy : tuberculoid leprosy : dermal epitheliod granulomatous infiltrate is seen that may have a linear pattern as it follows the course of a nerve. Epithelioid histiocytes and Langhans giant cells are surrounded by lymphocytes. The granulomas surrounds the fragmented nerve fibers there is an absence of organisms, even with special stains.
 which are")
Investigations Skin biopsy : Ø Diffuse infiltrate of foamy histiocytes (Virchow cells) which are macrophages with numerous bacilli as well as lipid droplets in their cytoplasm Ø A band of normal-appearing dermis, called Grenz zone, separates the epidermis from the infiltrate. Ø The bacilli can be detected by Ziehl-Neelsen, Fite stain, which stain the bacilli a bright red color. . �

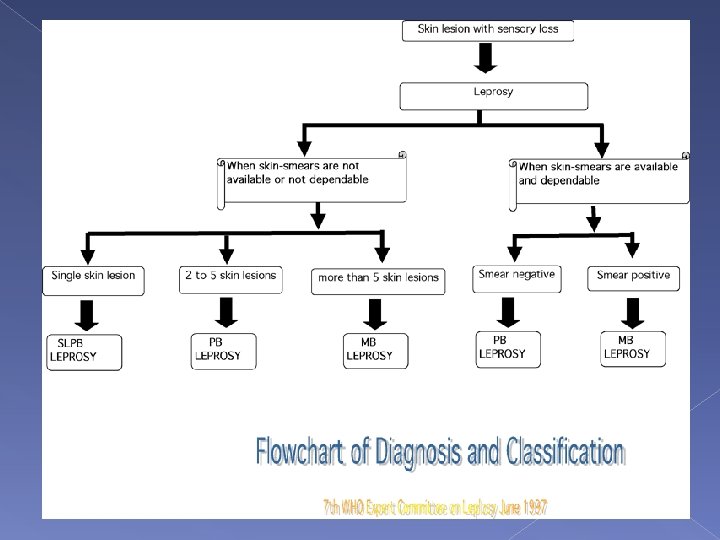
TREATMENT OF LEPROSY MULTIDRUG THERAPY/WHO SCHEME FOR THE TREATMENT OF LEPROSY Rifampin Clofazimine Dapsone Ofloxacin Minocycline. Therapy duration MB (>5 lesions 600 mg once monthly 300 mg once 100 mg monthly and daily 50 mg daily − − 12 to 18 months PB (2– 5 lesions) 600 mg once monthly − 100 mg daily − − 6 to 9 months PB (single lesion) 600 mg × 1 − − 400 mg × 1 100 mg × 1 Single dose

TREATMENT OF LEPROSY q Ø Ø Ø q Treatment of leprosy reactions: Never to stop the antilepromatous treatment Corticosteroids are important and it is used for short periods Immunomodulators Follow up of the patients: close follow up clinically and bacteriologically are needed for a minimum of 2 years in paucibacillary leprosy and 5 years in multibacillary leprosy
- Slides: 21