Leishmaniasis Cutaneous Mucocutaneous And Visceral Genus Leishmania Disease




![Morphology) Amastigotes (donovan bodies): • In vertebrates hosts [Man – Dog]. • Reticulo-Endothelial Cells](https://slidetodoc.com/presentation_image_h2/aa81b331f81fbe4b127831e2278d7dc2/image-5.jpg "Morphology) Amastigotes (donovan bodies): • In vertebrates hosts [Man – Dog]. • Reticulo-Endothelial Cells")




 Sand")


![Cutaneous leishmaniasis [CL] Ø Ø Old World CL: caused by L. tropica complex (L.](https://slidetodoc.com/presentation_image_h2/aa81b331f81fbe4b127831e2278d7dc2/image-15.jpg "Cutaneous leishmaniasis [CL] Ø Ø Old World CL: caused by L. tropica complex (L.")
![A- Old World Cutaneous Leishmaniasis L. tropica complex a. [1] Leishmania tropica Chronic, dry](https://slidetodoc.com/presentation_image_h2/aa81b331f81fbe4b127831e2278d7dc2/image-17.jpg "A- Old World Cutaneous Leishmaniasis L. tropica complex a. [1] Leishmania tropica Chronic, dry")
![[1] a- Chronic, Dry or Urban CL [caused by L. tropica]. Reservoir host: Dogs.](https://slidetodoc.com/presentation_image_h2/aa81b331f81fbe4b127831e2278d7dc2/image-18.jpg "[1] a- Chronic, Dry or Urban CL [caused by L. tropica]. Reservoir host: Dogs.")
 Dry ulcer or Oriental sore Ø Ø The lesion starts as a single")



![[2] a- Acute, Wet or Rural CL [caused by L. major] Reservoir host: Rodents.](https://slidetodoc.com/presentation_image_h2/aa81b331f81fbe4b127831e2278d7dc2/image-23.jpg "[2] a- Acute, Wet or Rural CL [caused by L. major] Reservoir host: Rodents.")
![[2] a- Acute, wet or rural CL [Cont. ] The Lesions are painless, severely](https://slidetodoc.com/presentation_image_h2/aa81b331f81fbe4b127831e2278d7dc2/image-24.jpg "[2] a- Acute, wet or rural CL [Cont. ] The Lesions are painless, severely")

![[3] a- Diffuse; Disseminated; Cutaneous Leishmaniasis [Caused by Leishmania aethiopica] Distribution: L. aethiopica occurs](https://slidetodoc.com/presentation_image_h2/aa81b331f81fbe4b127831e2278d7dc2/image-26.jpg "[3] a- Diffuse; Disseminated; Cutaneous Leishmaniasis [Caused by Leishmania aethiopica] Distribution: L. aethiopica occurs")


![Mucocutaneous Leishmaniasis or Espundia [Cont. ] Disfiguration is often extreme with complete destruction of](https://slidetodoc.com/presentation_image_h2/aa81b331f81fbe4b127831e2278d7dc2/image-29.jpg "Mucocutaneous Leishmaniasis or Espundia [Cont. ] Disfiguration is often extreme with complete destruction of")
![Chiclero’s ulcer L. mexicana Occurs in forest workers [Chicle collectors]. It is a single](https://slidetodoc.com/presentation_image_h2/aa81b331f81fbe4b127831e2278d7dc2/image-30.jpg "Chiclero’s ulcer L. mexicana Occurs in forest workers [Chicle collectors]. It is a single")


 Scrape or take")

 Local measures: � � Surgical excision especially in single lesions. Scraping (curettage).")
 Systemic treatment: Pentostam is the drug of choice. - Metronidazol against Mexican")



 Causes: A- In")


 all over the human body & reservoir")



, ↓ platelets (thrombocytopenia), also")



 Clinical diagnosis: kala azar may be suspected in a patient with irregular")

 test - - A delayed reaction develops")
: - formalin is added")


![Prevention & control q Treatment of cases [proper & complete]. q Control of reservoir](https://slidetodoc.com/presentation_image_h2/aa81b331f81fbe4b127831e2278d7dc2/image-57.jpg "Prevention & control q Treatment of cases [proper & complete]. q Control of reservoir")
- Slides: 57
Leishmaniasis Cutaneous, Mucocutaneous And Visceral
Genus: Leishmania Disease: Leishmaniasis I- Cutaneous leishmaniasis II- Mucocutaneous leishmaniasis III- Visceral Leishmaniasis.
Genus: Leishmania Disease: Leishmaniasis is classified according to its clinical picture & geographical distribution: I- Cutaneous leishmaniasis A- Old World Cutaneous leishmaniasis. B- New World Cutaneous leishmaniasis. � II- Mucocutaneous leishmaniasis A- New World Mucocutaneous leishmaniasis. III- Visceral Leishmaniasis.
Epidemiology • Leishmaniasis occurs in tropical and temperate regions, in the living areas of the sand fly vector (Phlebotomus spp. in Old world and Lutzomyia spp. in New world). • It is endemic in areas on four continents including the Middle East region. • ~1. 5 million annual new cases of which 3/4 are cutaneous forms and 1/4 visceral form.
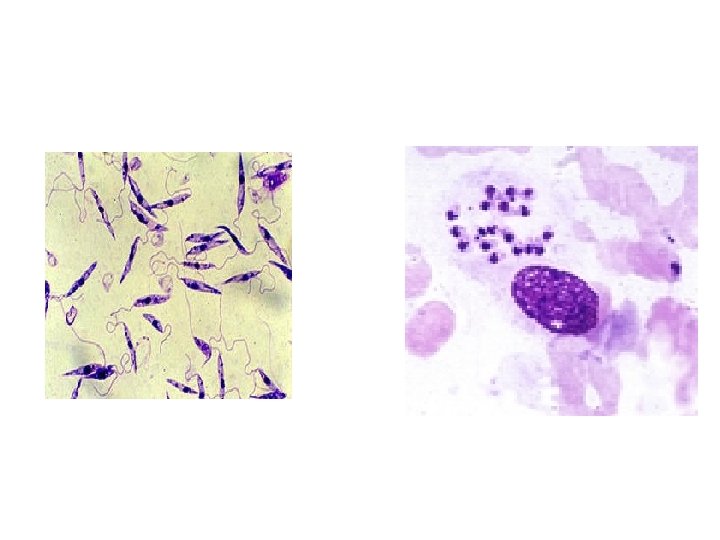
Morphology) Amastigotes (donovan bodies): • In vertebrates hosts [Man – Dog]. • Reticulo-Endothelial Cells (RECs) all body organs in VL and in skin macrophage in CL. • intracellular in macrophages. Promasitogtes (flagellated form): • Motile (with anterior flagellum) • [Vector – culture]
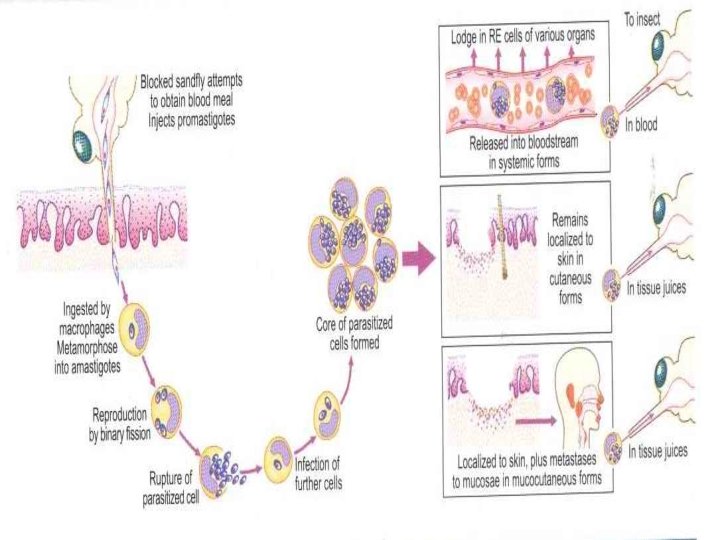
Life cycle of Leishmania species The infective stage is transmitted by the bite of several species of blood-feeding female sand flies (Phlebotomus or Lutzomyia) which carries the promastigote in the anterior gut and pharynx. It gains access to macrophages & other phagocytic cells of the reticuloendothelial system where it transform into amastigotes (Leishmania forms) and divides until the infected cell ruptures. The released organisms infect other cells. The sand fly acquires the organisms during its meal, the amastigotes transform into flagellate promastigotes (Leptomonad forms) and multiply in the gut until the anterior gut and pharynx are packed. Salivary glands are not invaded.
When the sand fly attempts a subsequent blood meal, some of the infective promastigotes are dislodged, regurgitated, and introduced into the skin bite by their motility.
Leishmania spp. life cycle
CUTANEOUS LEISHMANIASIS Cutaneous & Mucocutaneous Leishmaniasis
Cutaneous Leishmaniasis D. H. man R. H. dogs, rodents Vector (I. H. ) Sand fly
Geographical distribution of Cutaneous Leishmaniasis
Cutaneous Leishmaniasis Infective stage Promastigote or Amastigote. Transmission 1 - Biological: Bite of infected female ♀ sand flies. (Infective stage >>> Promastigote form). 2 - Mechanical: Direct contact & autoinfection. (Infective stage >>> Amastigote form).
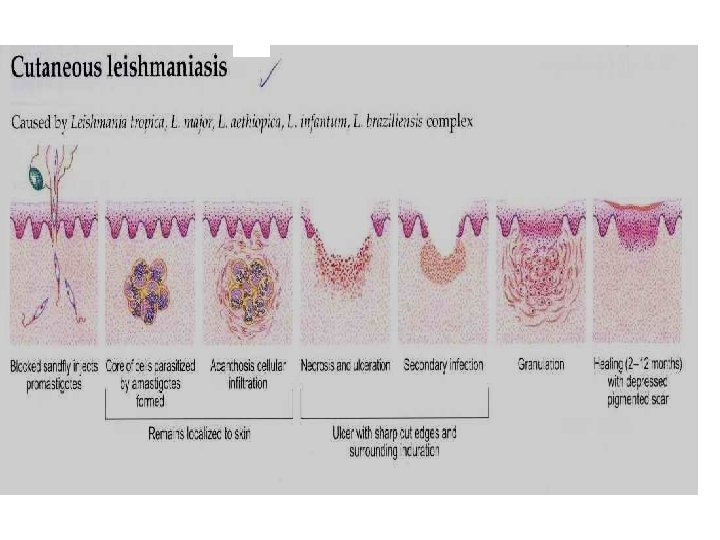
Cutaneous leishmaniasis [CL] Ø Ø Old World CL: caused by L. tropica complex (L. tropica, L. major & L. aethiopica). New World CL: caused by L. mexicana & L. braziliensis complexes. Classical lesion The lesion starts at the site of inoculation (bite) as a Papule >>> Nodule; due to multiplication of Leishmania form in skin macrophages & granulomatous reaction around them; then >>> ulcerates and the ulcer heals leaving a disfiguring scar.
A- Old World Cutaneous Leishmaniasis L. tropica complex a. [1] Leishmania tropica Chronic, dry or urban Cutaneous Leishmaniasis: (1) Painless ulcer or Oriental sore. [2] Leishmania major a. Acute, wet or rural Cutaneous Leishmaniasis. [3] Leishmania aethiopica a. Diffuse (Disseminated) Cutaneous Leishmaniasis.
[1] a- Chronic, Dry or Urban CL [caused by L. tropica]. Reservoir host: Dogs. Incubation period: 2 -8 months. Distribution: Occurs in Mediterranean region, Middle East, parts of Africa & Asia (mainly in urban areas). Insect vector: Female Sand fly - Phlebotomus papatassi
(1) Dry ulcer or Oriental sore Ø Ø The lesion starts as a single red pruritic papule on the exposed parts of the body. It is dry & painless. It increases in size, crusts & ulcerates after several months. The ulcer [Oriental sore] has sharp cut edges, raised indurated margin (volcano like), with scanty exudate Healing in about 1 -2 years leaving depigmented flat, atrophic, disfiguring scar.
Dry Oriental Sore.
[2] a- Acute, Wet or Rural CL [caused by L. major] Reservoir host: Rodents. Incubation period: 2 -6 weeks. Distribution: Occurs in the desert areas of Middle East, Asia, Africa [mainly in rural areas]. Lesions are multiple & more severe than the chronic, dry type of L. tropica
[2] a- Acute, wet or rural CL [Cont. ] The Lesions are painless, severely inflamed, moist with serous exudate and rapidly ulcerating. Healing takes place within 3 -6 months, leaving large disfiguring scars.
[3] a- Diffuse; Disseminated; Cutaneous Leishmaniasis [Caused by Leishmania aethiopica] Distribution: L. aethiopica occurs mainly in Ethiopia, Kenya & south Yemen. The parasite causes chronic disseminated nodules, NOT Ulcerate. [due to deficient cell-mediated immunity & Failure of Immune system] Diffuse Cutaneous Leishmaniasis similar to Lepromatous leprosy
B- New world cutaneous leishmaniasis q Ø Ø Ø Parasite: L. braziliensis complex a. Espundia: b. Uta: Caused by L. peruviana; & L. mexicana complex. a. Chiclero’s ulcer b. Diffuse Cutaneous Leishmaniasis. Distribution: Occurs in Central & South America. Reservoir hosts: Forest rodents & dogs. Vector: ♀ sand fly, genus Lutzomyia.
II- Mucocutaneous Leishmaniasis or Espundia L. braziliensis produces single or multiple lesions; that undergo extensive ulceration. lymphatic spread to mucous membranes of nose, mouth & ear may occur >>> causing hypertrophy, destruction, severe pain & great deformity.
Mucocutaneous Leishmaniasis or Espundia [Cont. ] Disfiguration is often extreme with complete destruction of the nasal septum, perforation of the palate and damage to the tissues of the lips and larynx. Oedema, tissue destruction, (Espundia). Death may develop from aspiration pneumonia, or septicemia.
Chiclero’s ulcer L. mexicana Occurs in forest workers [Chicle collectors]. It is a single painless lesion mainly affects the ear Causing destruction of cartilage & heal spontaneously within 6 months. Chiclero’s ulcer
Diagnosis of Cutaneous Leishmaniasis
1 - Direct Laboratory Methods Ø 1 -a- Aspirated tissue juice, scraping or biopsy material from raised nodule or raised edge of the ulcer & from mucosal scraping in mucocutaneous type to detect the parasite after: preparing smears & staining with Giemsa or Leishman stains >>> Amastigote form. Amastigote b- Inoculation in culture [NNN medium] >>> Promastigote form. c- Animal inoculation 2 - Aspirate or biopsy >>> PCR to diagnose & type the species. Promastigote
Aspiration and biopsy from the ulcer Aspiration Leishmania amastigotes (Giemsa stained) Scrape or take biopsy
2 - Indirect Laboratory Methods 2 - Indirect methods: a- Intradermal skin test [Leishmanin or Montenegro's test]: It is a delayed hypersensitivity skin test. Positive test [˃ 95%] >>> induration more than 5 mm at site of injection after 48 hours. It is –ve in D. C. L. (since there is deficiency in cell mediated immunity).
Treatment 1) Local measures: � � Surgical excision especially in single lesions. Scraping (curettage). Intra- lesional injection of pentavalent antimonial or 2% atebrine sulphate I. D. Heating of lesion to 50% with coned infra red rays & freezing therapy, using carbon dioxide snow. - Antibiotics: for 2 nd bacterial infections
Treatment 2) Systemic treatment: Pentostam is the drug of choice. - Metronidazol against Mexican cutaneous leishmaniasis gives impressive results. - Amphotricin B.
Prevention & control q Treatment of cases, control of reservoir hosts. q Proper dressing of the ulcer q Active immunization on concealed parts of body in endemic areas. q Protection: by using wire screens, repellents & mosquito nets fine mesh screening (40 meshes/ inch 2) q Control of sand flies by destruction of their breeding grounds and by the use of residual chlorinated hydrocarbon as DDT.
Leishmania species & Disease SPECIES Leishmania tropica * Leishmania major * Leishmania aethiopica Leishmania mexicana Leishmania braziliensis Leishmania donovani * Leishmania infantum * Leishmania chagasi Disease Cutaneous Leishmaniasis Mucocutaneous Leishmaniasis Visceral Leishmaniasis
VISCERAL LEISHMANIASIS
1 - Visceral Leishmaniasis (Kala azar, black fever or Dum-dum fever) Causes: A- In old world : L. donovani complex that includes, L. donovani and L. infantum. B- In new world: L. chagasi and L. amazonensis.
Geographical distribution of Visceral Leishmaniasis
Geographical distribution L. donovani: the disease is endemic in India, Pakistan, Indonesia Thailand, Central Africa & Sudan. L. infantum: Mediterranean area (North Africa) and southern Europe, as it affects principally infants and young children L. chagasi: in the Americas (central & south America).
Morphology : - In Reticulo-Endothelial Cells (RECs) all over the human body & reservoir hosts, it takes numerous amastigote (Leishmalial) forms, intracellular in macrophages. - In insect vector and culture, it takes the promastigote (Leptomonal) form.
Life Cycle: Habitat: R. E. Cs of the viscera, especially of spleen, liver, bone marrow, intestinal mucosa & mesenteric lymph nodes. � � � Definitive host: Man. Reservoir hosts: domestic dogs, rodents & desert gerbils. Insect vectors: are female Sand flies of the Genus Phlebotomus , which in the Americas has been renamed Lutzomyia. Infective stage: Promastigotes in buccal cavity & proboscis of Sand fly. Mode of infection: 1) Bite of infected sand fly. 2) Blood transfusion. 3) Direct from man to man in epidemics by nasal
Clinical Manifestations The incubation period is long 1 -3 months, but may be as short as 2 weeks. A primary lesion at the site of infection is rarely observed, minute papules (dermal leishmaniomas). The phagocytosed parasites are numerous in the R. E. Cs of the previously mentioned organs with marked hyperplasia.
Clinical Manifestations The most important physical finding is fever with characteristic twice-daily elevation, +malaise, headache, sweating, weakness, hepatomegaly. Splenomegaly. Diarrhea and dysentery,
Clinical Manifestations Bone marrow involvement ↓ production of reticulocytes (aneamia), ↓ platelets (thrombocytopenia), also ↓ WBCs (neutropenia) allows bacteria and other secondary invaders to attack tissues. Oedema of the skin, ematiation, bleeding tendancy Anaemia in Kala-azar may be: 1) Aplasatic anaemia due to extensive multiplication of parasites in bone marrow. 2) Microcytic anaemia in 5% due to lack of iron absorption from intestine. 3) Macrocytic anaemia due to hepatic damage & fatty infiltration deficient storage of vit. B 12.
Clinical Manifestations Hyperpigmentation of the skin may be noticed, the term Kala-azar is for black sickness. A butterfly distribution over the nose.
Clinical Manifestations Post kala- azar dermal leishmanoid: It is an outbreak of chronic, progressive, granulomatous hypopigmented cutaneous nodules (no ulceration). It may appear 6 months to 5 years after spontaneous or drug cure. The parasite will migrate to the skin mostly of the face resemble Lupromatous leprosy or disseminated
Diagnosis of Visceral Leishmaniasis
Diagnosis 1) Clinical diagnosis: kala azar may be suspected in a patient with irregular or remittent fever (often a double daily peak), hepato-splenomegaly, pain from perisplenism, anaemia, leucopenia & ematiation. 2) Laboratory diagnosis: [parasite or antibodies] A- Direct: - Detection of the parasites (amastigote inside & outside macrophages) in blood films after staining with
Diagnosis - - The parasite can be demonstrated in aspirates from LN, liver , bone marrow, or Splenic puncture or blood : examined directly, or inoculated in N. N. N. culture media showing promastigotes in the form of rosette grouping of parasites.
Diagnosis B- Indirect: 1 - Montenegro (leishmanin) test - - A delayed reaction develops in cured individuals. - The test is negative in early cases due to depression of cellular immunity by the parasites, but becomes
Diagnosis 2 - Aldehyde test (Formol gel or Napier's test): - formalin is added to serum of person. The test is positive if the serum solidified. - It depends upon ↑ of serum gamma globulins. 3 - Antimony test (Chopra's or Urea-Stibamine test) : formation of white ring at the interface indicates positive reaction. 4 - Globulin opacity test or (Sia's test) : - distilled water. opaque in positive cases. 5 - Fluorescent antibody test 6 - ELISA, IFA or direct agglutination: (↑ Ig. G).
Diagnosis
Treatment 1 - Supportive treatment includes : - Good nursing care. - Diet rich in vitamins, iron & antibiotics. - Blood transfusion, for patients with severe anaemia or bleeding problems. 2 - Specific treatment : - Pentostame (Antimony sodium gluconates or Sodium stibogluconate). - Amphotricin B.
Prevention & control q Treatment of cases [proper & complete]. q Control of reservoir hosts. q Screening of blood donors q Protection: by using wire screens, repellents & mosquito nets fine mesh screening (40 meshes/ inch 2) q Control of sand flies by destruction of their breeding grounds and by the use of residual chlorinated hydrocarbon as DDT.