Left Ventricular Failure Pathophysiology Results in increased back

�Left Ventricular Failure �Pathophysiology Results in increased back pressure into the pulmonary circulation Causes � MI, valvular disease, chronic hypertension, and dysrhythmias

Right Ventricular Failure Pathophysiology Results in increased back pressure into the systemic venous circulation Causes Left ventricular failure Pulmonary Embolism

�Congestive Heart Failure �Pathophysiology Reduction in the heart’s stroke volume causes fluid overload throughout the body’s other tissues � Starling’s law no longer able to compensate �Manifestation In the acute setting, pulmonary edema, pulmonary hypertension, or myocardial infarction In the chronic setting as cardiomegally, left ventricular failure, or right ventricular failure

�Field Assessment �Check ABC’s and manage life threats �Chief Complaint OPQRST � Paroxysmal Nocturnal Dyspnea (PND) �Medications: Diuretics Medications to increase cardiac contractile force � Lanoxin Home oxygen

�Mental Status �Mental status changes indicate impending respiratory failure �Breathing �Signs of labored breathing �Tripod positioning �“Number of pillows” �Skin �Color changes �Peripheral and/or sacral edema

�Complications �Pulmonary edema may lead to respiratory failure �Pulsus paradoxus Systolic blood pressure drops more than 10 mm. Hg with inspiration �Pulsus alternans Pulse alternates between weak and strong

�Management �General management: Avoid supine positioning Avoid exertion such as standing or walking �Maintain the airway Administer oxygen �Administer �CPAP Nitroglycerine as soon as possible

�Monitor ECG �Establish IV access Limit fluid administration �Consider medication administration: �Nitrates �Angiotensin-converting Catopril Enalopril �Albuterol �Vasopressor Dopamine �Avoid enzyme (ACE) inhibitor patient refusals if at all possible
 Can often prevent the need for endotracheal intubation")
Continuous Positive Airway Pressure (CPAP) Can often prevent the need for endotracheal intubation and mechanical ventilation © Scott Metcalfe
 Positive Airway Pressure �Maintains a constant pressure within the airway throughout the")
�Continuous (CPAP) Positive Airway Pressure �Maintains a constant pressure within the airway throughout the respiratory cycle CPAP will force excess fluid out of the alveoli PEEP is applied only during expiration �Use the lowest effective pressure when applying CPAP A pressure of 2. 5– 5 cm/H 2 O is adequate

Asthma, COPD, pulmonary edema, CHF, or pneumonia Awake and able to follow commands >12 years old and able to fit the CPAP mask Able to maintain an open airway Exhibits two or more of the following A respiratory rate greater than 25 breaths per minute Sp. O 2 of less than 94% at any time Use of accessory muscles during respirations

�Any patient who is in respiratory arrest or apnea �Pneumothorax or has suffered trauma to the chest �Tracheotomy �Patient who is actively vomiting or has upper GI bleeding

�Epidemiology and Pathophysiology �Pathophysiology Result of fluid accumulation between visceral pericardium and parietal pericardium Increased intrapericardial pressure impairs diastolic filling Typically worsens progressively until corrected �Epidemiology Acute onset typically the result of trauma or MI Benign presentations may be caused by cancer, pericarditis, renal disease, and hypothyroidism

�Field Assessment �Patient History Determine precipitating causes Patient relates a history of dyspnea and orthopnea �Exam Rapid, weak pulse Decreasing systolic pressure Narrowing pulse pressures Pulsus paradoxus Faint, muffled heart sounds Electrical alternans � Less than normal voltage in waveforms

�Management �Maintain airway �Administer oxygen �Establish IV access �Consider medication administration: Morphine sulfate Nitrous oxide Furosemide Dopamine/dobutamine

�Rapid Transport �Pericardiocentesis is the definitive treatment Insertion of a cardiac needle and aspiration of fluid from the pericardium �Procedure should be performed only if allowed by local protocol �Procedure should be performed only by personnel adequately trained in the procedure

�Hypertensive Emergency �Causes Typically occurs only in patients with a history of hypertension Primary cause is noncompliance with prescribed antihypertensive medications Also occurs with toxemia of pregnancy �Incidence Risk Factors � Age-related factors � Race-related factors

�Field Assessment �Initial Assessment Alterations in mental state �Signs and Symptoms Headache accompanied by nausea and/or vomiting Blurred vision Shortness of breath Epistaxis Vertigo Tinnitus

�History �Known history of hypertension �Compliance with medications �Exam �BP >160/90 �Signs of left ventricular failure �Strong, bounding pulse �Abnormal skin color, temperature, and condition �Presence of edema

�Management �Maintain airway �Administer oxygen �Establish IV access �Consider medication administration: Nitroglycerin Sodium nitroprusside (Nipride) Labetalol (Trandate, Normodyne)

�Pathophysiology �General Inability of the heart to meet the body’s metabolic needs Often remains after correction of other problems Severe form of pump failure High mortality rate �Causes Tension pneumothorax and cardiac tamponade Impaired ventricular emptying Impaired myocardial contractility Trauma

�Field Assessment �Initial Assessment �Chief Complaint Chief complaint is typically chest pain, shortness of breath, unconsciousness, or altered mental state Onset may be acute or progressive �History of recent MI or chest pain episode Presence of shock in the absence of trauma

�Mental Status �Restlessness �Airway progressing to confusion and Breathing �Dyspnea, labored breathing, and cough �PND, tripod position, accessory muscle retraction, and adventitious lung sounds �ECG �Tachycardia and atrial dysrhythmias �Circulation �Hypotension �Cool, clammy skin

�Management �Maintain CPAP airway �Administer oxygen �Identify and treat underlying problem �Establish IV access Consider aggressive fluid therapy �Consider medication administration: Dopamine, dobutamine, norepinephrine

Click here to view the Cardiogenic Shock diagram.

�The absence of ventricular contraction �Immediately results in systemic circulatory failure �Sudden death is any death that occurs within 1 hour of symptom onset �Severe atherosclerotic disease is common �Risk factors

Acid-base imbalance Drowning Drug intoxication Electrocution Electrolyte imbalance End-stage renal disease Hyperkalemia (high levels of potassium) Hypothermia Hypoxia Pulmonary embolism Stroke Trauma

�Patients who suffer a cardiac arrest resulting from ventricular fibrillation go through several phases leading up to biological death �Electrical �Circulatory �Metabolic �Prehospital intervention required depends on the phase the patient is in
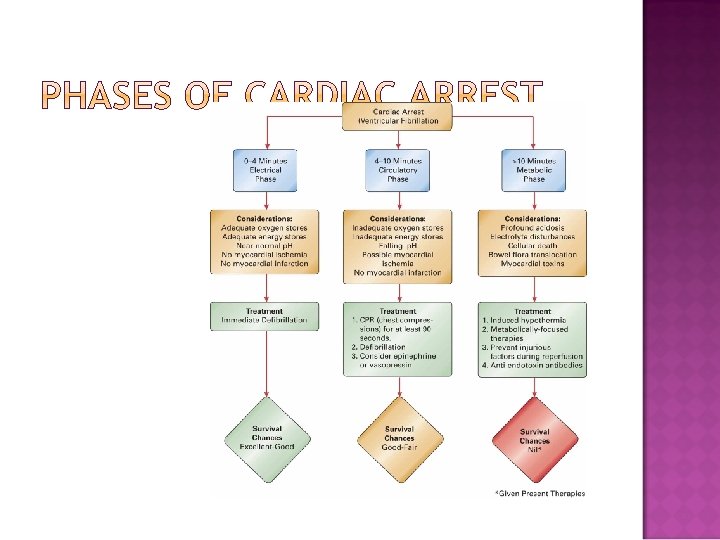

�Electrical Phase �Begins at the time of the cardiac arrest and ends at approximately 3 to 4 minutes postarrest �Adequate oxygen at the level of the myocardial cells Cells are able to maintain energy production through aerobic metabolism �The only beneficial treatment is immediate defibrillation

�Circulatory Phase � 4– 10 minutes post-arrest �Oxygen levels in the myocardial cells are inadequate Shift to anaerobic metabolism �Survival from cardiac arrest during this phase is better if at least 90 seconds of CPR is provided before the application of defibrillation Epinephrine beneficial

�Metabolic Phase �Begins approximately 10 minutes after the onset of cardiac arrest �Failure of the sodium-potassium pump Sodium begins to diffuse into the cell Water follows sodium Cellular swelling and eventually lysis �Current resuscitative measures do not improve survival during the metabolic phase

�Field Assessment �Initial Assessment Unresponsive, apneic, pulseless patient �ECG Dysrhythmias �History Prearrest events Bystander CPR “Down time”

�Management �Terms Resuscitation Return of Spontaneous Circulation Survival �Role of Basic Life Support �General Guidelines Manage specific dysrhythmias CPR Advanced airway management Establish IV access

�Pharmacological considerations �Amiodarone �Atropine sulfate �Epinephrine �Lidocaine �Magnesium sulfate �Vasopressin �Follow medications in arrest with a bolus of fluid

Click here to view the Cardiac Arrest diagram. Reproduced with permission from “ 2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Care, ” Circulation 2005, Volume 112, IV-59. © 2005 American Heart Association.

�Manage dysrhythmias and problems as presented. �Be alert for PEA �Transport rapidly: Take care to protect intubation and IV access �Withholding �Rigor resuscitation mortis �Dependent lividity �Decapitation, decomposition, incineration �Valid advance directive

�Terminating Resuscitation �Inclusion criteria for termination of resuscitation: Patient over 18 years old Cause is presumed cardiac in origin Successful endotracheal intubation ACLS standards applied throughout the arrest On-scene effort >25 minutes, or four rounds of drug therapy ECG remains asystolic or agonal

�Terminating Resuscitation �Exclusion Criteria: Patient under 18 years old Arrest is of a treatable cause Present or recurring VF/VT Transient return of a pulse Signs of neurological viability Witnessed arrest Family or others opposed to termination of resuscitation �Always follow local protocols related to termination of resuscitation

�Atherosclerosis �Pathophysiology Progressive degenerative disease of the medium-sized and large arteries Results from the buildup of fats on the interior of the artery Fatty buildup results in plaques and eventual stenosis of the artery �Arteriosclerosis �Claudication

�Aneurysm �Pathophysiology Ballooning of an arterial wall, usually the aorta, that results from a weakness or defect in the wall �Types Atherosclerotic Dissecting Infectious Congenital Traumatic

�Abdominal Aortic Aneurysm �Often the result of atherosclerosis �Signs and symptoms: Abdominal pain Back/flank pain Hypotension Urge to defecate

�Dissecting �Caused Aortic Aneurysm by degenerative changes in the smooth muscle and elastic tissue �Blood gets between and separates the wall of the aorta �Can extend throughout the aorta and into associated vessels

�Acute Pulmonary Embolism �Pathophysiology Blockage of a pulmonary artery by a blood clot or other particle The area served by the pulmonary artery fails �Signs and Symptoms Dependent upon size and location of the blockage Onset of severe, unexplained dyspnea History of recent lengthy immobilization

�Acute Arterial Occlusion �Pathophysiology Sudden occlusion of arterial blood flow due to trauma, thrombosis, tumor, embolus, or idiopathic means Frequently involves the abdomen or extremities �Vasculitis �Pathophysiology Inflammation of the blood vessels Commonly stems from rheumatic diseases and syndromes

�Noncritical Peripheral Vascular Conditions �Peripheral Arterial Atherosclerotic Disease Can be acute or chronic Often associated with diabetes Extremities exhibit pain, coldness, numbness, and pallor �Deep Venous Thrombosis Blood clot in a vein Typically occurs in the larger veins of the thigh and calf Swelling, pain, and tenderness, with warm, red skin �Varicose Veins Dilated superficial veins, common with pregnancy and obesity

�General Assessment and Management of Vascular Disorders �Assessment Initial Assessment Circulatory Assessment � Pallor � Pain � Pulselessness � Paralysis � Paresthesia
 �Chief Complaint OPQRST �Physical Exam Prior history of vascular problems Differences")
�Assessment (cont. ) �Chief Complaint OPQRST �Physical Exam Prior history of vascular problems Differences in pulses or blood pressures �Management �Maintain the airway �Administer oxygen if respiratory distress or signs of hypoperfusion present �Consider administration of analgesics �Transport rapidly if signs of hypoperfusion present

�Assessment of the Cardiovascular Patient �Management of Cardiovascular Emergencies �Managing Specific Cardiovascular Emergencies
- Slides: 49