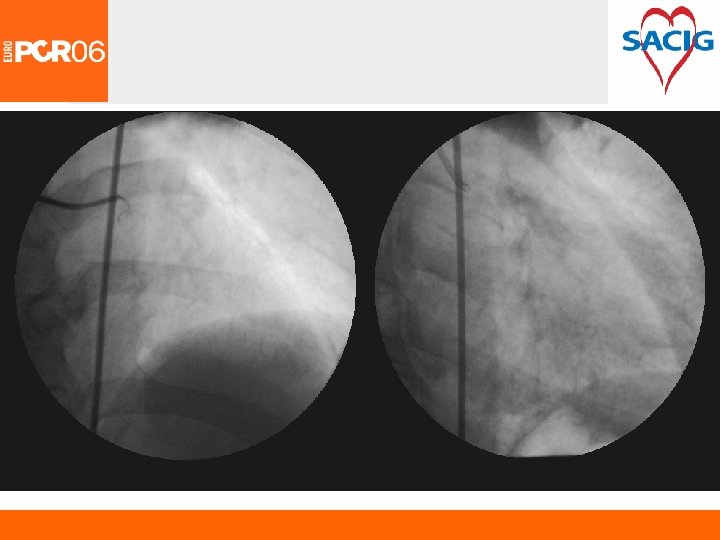
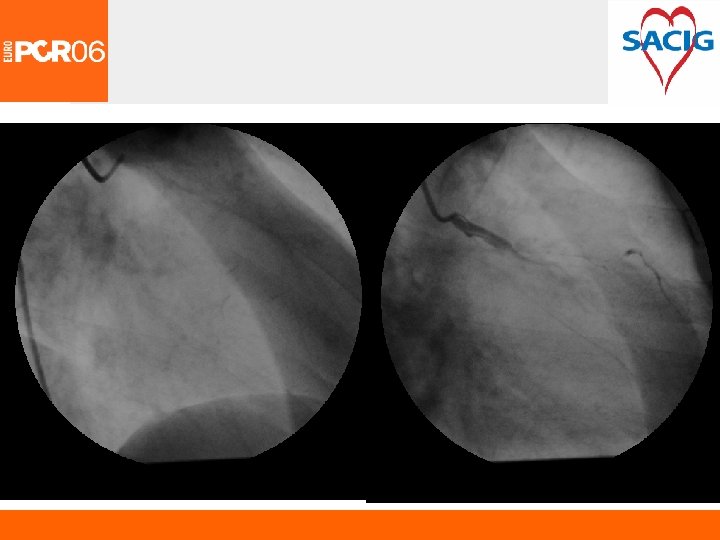
Left Main Coronary Artery Dissection Complicating Diagnostic Coronary














")














- Slides: 31
Left Main Coronary Artery Dissection Complicating Diagnostic Coronary Angiography Layth A. Mimish MBCh. B, FRCPC, FACC Medical Director The Cardiovascular Consultant Clinic Jeddah, KSA
I have no conflict of interest pertaining to this presentation
Left Main Coronary Dissection • Definition and Classification • Incidence • Etiology • Management Conservative CABGS Stenting
NHLBI Classification
Left Main Coronary Dissection • Spontaneous • Extension from Aortic Dissection • Complication of Diagnostic Coronary Angiography or Coronary Interventional procedure
Iatrogenic Left Main Coronary Dissection • Calcification of Lt. Main Stem • Anatomical distortion in aortic root or origin of Lt main that makes selective intubation difficult • The angle formed by the tip of the catheter and the intima of the vessel • The depth with which the artery is cannulated • Forceful injection with dampened pressure • Femoral Vs radial approach • Diagnostic Vs PCI
Left Main Coronary Dissection • Sone’s initial series 4200 diagnostic procedures, 1 reported dissection • Massachusetts General Hospital 1970 -1975 2981 Pts, Lt. main dissection in 1 • Dennis, W. , William O’Neil, Cath C V Intervention 2000, data review 43, 143 diagnostic procedures and PCI (0. 02%) • Carter AJC 1994 3 cases, incidence 0. 02 for diagnostic angiography, and 0. 07% for PCI • Under-reported, with severity varying from type A to severe aortic root dissection
Conservative Treatment
CABG Vs Medical Therapy
ACC / AHA Guidelines
Clinical Outcomes with CABG in Lt. Main Disease • 18 Centers • Jan 2001 -June 2003 • 5, 494 Consecutive CABG with no exclusion • 1, 394 Lt main (24. 1%) • Operative mortality 4. 1% (All other CABG 2. 3%) • CVA 1. 3% Katz, Mack, Simon
OPCAB in LMCA Disease n Predicted Mortality Observed Mortality Risk Adjusted Mortality Off Pump On Pump 273 1, 163 4. 1% 3. 6% 2. 6% 4. 5% 1. 9% 3. 8% Dewey, et al, Ann Thorac Surg 2001
Motality for CABG in Lt Main NYS Database 1997 -2000
Stent Vs Conventional Rx for Abrupt Closure or Symptomatic Dissection
French Lt Main Registry May 2001 -June 2002 (11 French Centers)
French Lt Main Registry 1 Yr Outcome
French Lt Main Registry 1 Month &1 Yr Outcome
French Lt Main Registry 1 Month &1 Yr Outcome
French Lt Main Registry 1 Month &1 Yr Outcome
IVUS Optimization for Stent Deployment
DES Vs BMS in Milan 6 Month Clinical & Angiographic F/Up
DES in Lt Main Disease RESEARCH & T-SEARCH Registry • April 16, 2002 -Dec 31, 2003 • > 50% Lt min • Consensus agreement with CV surgeon with patient and referring MD • 95 Consecutive Pts, with 1 DES (SES 52, PES 43) • Comparison group 86 Consecutive pts who got BMS for Lt main immediately before DES availability • Median F/UP 503 days (331 -873)
DES in Lt Main Disease RESEARCH & T-SEARCH Registry
LMCA Intervention in AMC
In Hospital Outcome
Overall Restenosis rate 7. 9%
6 Months Clinical Outcome
MACE Free Survival at 1 Year
Coclusion • Rapid & thorough assessment • CV Surgeon involved • Haemodynamic support • DES Vs emergency CABGS • IVUS