Lecture Notes By Dr Syed Mohammad Zubair MBBSKE
 BS (PU) DHA (CCM) FWHO(UK)")
Lecture Notes By • Dr. Syed Mohammad Zubair MBBS(KE) BS (PU) DHA (CCM) FWHO(UK) MBA; FACHE (US) M. PHIL (UOL) Assist. Prof Physiology KEMU, Lahore

MICTURITION • Urination is the release of urine from the urinary bladder through the urethra to the urinary meatus outside of the body. It is also known medically as • MICTURITION Ø voiding Ø uresis Ø emiction. • COLLOQUIALLY Ø tinkling, Ø peeing, Ø Weeing Ø pissing.
 the process of urination is")
• In healthy humans (and many other animals) the process of urination is under voluntary control. • In infants, some elderly individuals, and those with neurological injury, urination may occur as an involuntary reflex. • In some animals, in addition to expelling waste material, urination can mark territory or express submissiveness.

• Physiologically, urination involves coordination between the central, autonomic, and somatic nervous systems. • Brain centres that regulate urination include the pontine micturition centre, periaqueductal gray, and the cerebral cortex. • In male placental mammals, urine is ejected through the penis. • In female placental mammals, urine is ejected through the vulva or pseudo-penis

MICTURITION
 • Ureters")
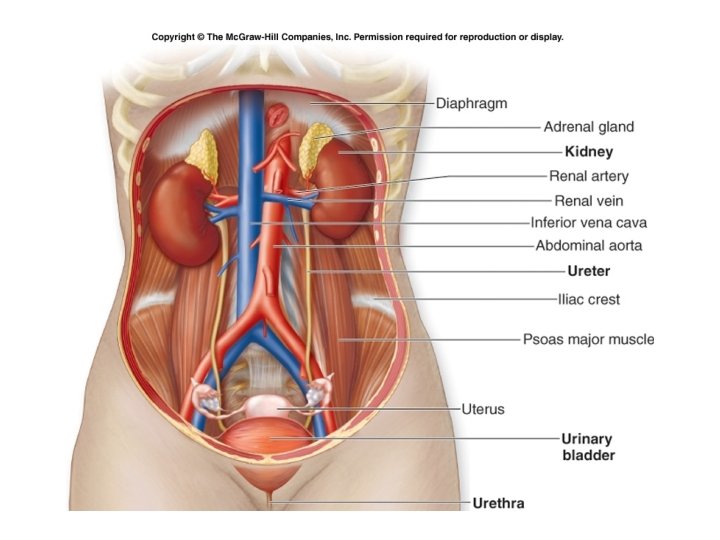
Physiological Anatomy of Urinary System • Kidneys (cortex, medulla, nephron, pelvis ) • Ureters (mucosa, muscle, fibrous) • Urinary Bladder (body, neck), (mucosa, muscle, fibrous) (detrusor, trigone) • Urethra • Internal and External sphincters
 – Stores urine")
Anatomy & Neurophysiology of the Lower Urinary Tract • Bladder (detrusor) – Stores urine at low pressure – Compresses urine for voiding • Urethra – Conveys urine from bladder to outside world • Sphincter(s) internal & external – Controls urine flow & maintain continence between voidings

Transport of Urine from the Kidney through Ureters into Bladder • Kidneys – Calyces • • Ureters Bladder Vesicoureteral Reflux Pain and uerterorenal reflex

Urinary Bladder

Filling of the bladder The walls of ureters contain smooth muscle arranged in spiral, longitudina l and circular bundles. When urine collects in the renal pelvis, the pressure in the pelvis increases. This increase in the pressure initiates a peristaltic contraction beginning in the pelvis and spreading downward along the ureter to force urine toward the bladder. Peristaltic waves occur 1 -5 times/minute

In some people, the distance that the ureter courses through the bladder mucosa is less than normal, so that contraction of the bladder during micturition does not always lead to complete occlusion of the ureter. As a result some of the urine in the bladder is propelled backward into the ureter. This is called ‘Vesicoureteral reflux’. Uerterorenal reflex The ureters are well supplied with pain nerve fibers. When a ureter is blocked e. g. . by a ureteral stone, there will be intense reflex constriction which is associated with very severe pain. These pain impulses cause a sympathetic reflex back to the kidney to constrict the renal arterioles, thereby decreasing urinary output from that kidney. This effect is known as ‘Uerterorenal reflex’.
 1. PARASYMPATHETIC NERVES (PELVIC NERVE) (S 2 -3) a) Sensory")
INNERVATION OF BLADDER (MAIN) 1. PARASYMPATHETIC NERVES (PELVIC NERVE) (S 2 -3) a) Sensory (stretch) b) Motor (detrusor, Internal sphincter) 2. SKELETAL MOTOR FIBER (PUDENDAL NERVES) (S 2 -3) a) Sensory (stretch) b) Motor (external sphincter) 3. SYMPATHETIC NERVES (HYOGASTRIC NERVES) (L 2) a) Sensory (fullness, pain) b) Motor (stimulate blood Vs) They prevent reflux of semen into the bladder during ejaculation.

Sympathetic nerve supply L 1 Parasympathetic nerve supply S 2 S 3 L 2 Pelvic nerve L 3 S 4 Sympathetic chain Somatic nerve supply S 2 Hypo gastric ganglion S 3 S 4 Hypo gastric nerve Urethra External sphincter Pudendal nerve

Bladder Innervation

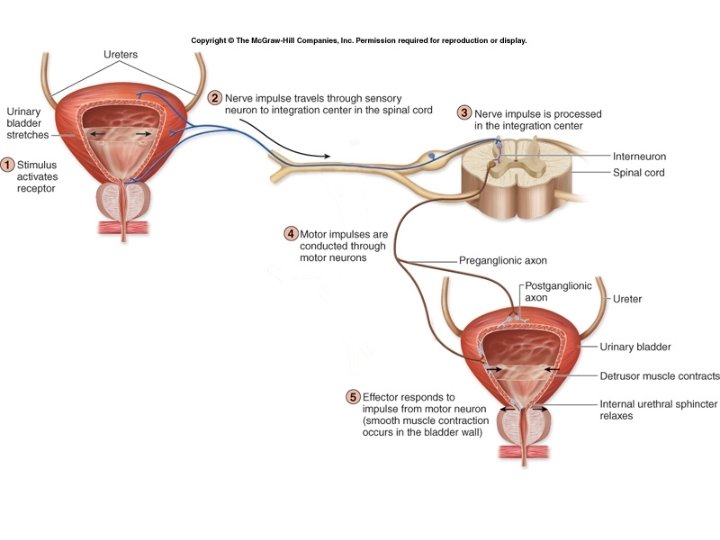
Regulation of the Bladder Main Influence: Parasympathetic Para Pelvic nerve 2. This causes the contraction of the detrusor muscle, via the pelvic nerve. Sym 1. Pressure builds up in the bladder Hypo gastric nerve 3. The internal sphincter relaxes due to decreased sympathetic stimulation. Pudendal nerve Vol Detrusor muscle 4. The external sphincter relaxes due to voluntary decrease in stimulation. Internal sphincter External sphincter

What is micturition reflex? Spinal cord reflex activity. * facilitated or inhibited by higher centers * voluntary facilitation or inhibition

Micturition Reflex • Micturition contractions begin • Role of sensory and motor parasympathetic nerves • Self regenerative once begins • Complete cycle – Rapid increase in pressure – Period of sustained pressure – Return to basal tone

Bladder Filling & Emptying Cycle 1. Bladder fills Detrusor muscle relaxes Urethral sphincter contracts Detrusor muscle contracts Urination The cycle of bladder filling and emptying Urethral sphincter relaxes 3. Urination voluntarily inhibited until time and place are right 2. First desire to urinate (bladder half full)
 300 -400 ml urine in bladder,")
Voiding Urine - Micturition • Micturition reflex 1) 300 -400 ml urine in bladder, stretch receptors send signal to spinal cord (S 2, S 3) 2) parasympathetic reflex arc from spinal cord, stimulates contraction of detrusor muscle 3) relaxation of internal urethral sphincter 4) this reflex predominates in infants

• Infants – Spinal reflex • Adults – Spinal reflex – Higher control • (pelvic muscles and external urethral sphincter)

Normal Control of Urination
 20 0 0 Ib")
Cystometrogram 80 Intravesica l pressure 60 (cm of 40 Water) 20 0 0 Ib Ia 100 200 300 Intravesical volume (m. L) 400

Bladder filling –Cystometrogram • Relation between bladder volume & pressure. • Empty bladder……P zero • 30 -50 ml urine……P 5 -10 cm H 2 O • 50 – 300 ml urine…. P 5 -10 cm H 2 O • More than 400 ml…. . rapid rise in P

LAW of LAPLACE • This is in accordance with law of Laplace. In the bladder tension increases as the urine is filled. At the same time, the radius also increases due to relaxation of the detrusor muscle. Because of this, the pressure rise is almost nil.

• When bladder wall stretches during filling it will initiate a reflex contraction which has lower threshold. That does not trigger micturition reflex. When bladder is filled about 300 – 400 m. L of urine, there will be sharp rise in the intravesical pressure as the micturition reflex is triggered. • At this point also voluntary control is possible. Beyond 600 – 700 m. L of urine voluntary control starts failing.

Filling of the bladder ………. . Filling of the bladder – partially filled Reflex contractions Acute increase in pressure Contractions relax spontaneously Pressure falls back to baseline Bladder continues to fill Reflex contractions – more frequently and powerful

Facilitation or inhibition of micturition by brain • Pons – Facilitatory and inhibitory centers • Cortex – Mainly inhibitory centers Voluntary Urination

• Micturition center is located in the – Frontal lobe • Function of micturition center – Send tonically inhibitory signals to the detrusor muscle to prevent the bladder from emptying (contracting) until a socially acceptable time and place to urinate is available.

Next stop is the…. . Pons • The major relay center between the brain and the bladder • Pontine micturition center – The PMC coordinates the urethral sphincter relaxation and detrusor contraction to facilitate urination

Pontine Micturition Center • Bladder filling detrusor muscle stretch receptors signal to the pons brain – Perception of this signal (bladder fullness) as a sudden desire to go to the bathroom – Normally, the brain sends an inhibitory signal to the pons to inhibit the bladder from contracting until a bathroom is found. • Brain deactivating signal to PMC – Urge to urinate disappears – At appropriate time, brain sends excitatory signals to the pons, allowing voiding

Next Stop After the PMC…. Spinal cord • Function – Long communication pathway between the brainstem and the sacral spinal cord – Sensory information from bladder Sacral cord Pons Brain Pons Spinal cord Sacral cord Bladder – Spinal cord acts as an important intermediary between the pons and the sacral cord – Intact spinal cord is critical for normal micturition

Normal Micturition – Spinal Cord • Sacral spinal cord – what is the significance? – Sacral reflex center • Responsible for bladder contractions • Primitive voiding center – In infants, the brain is not mature enough to command the bladder – SRC controls urination in infants and young children – When urine fills the infant bladder, an excitatory signal sacral cord spinal reflex center detrusor contraction involuntary detrusor contractions with coordinated voiding

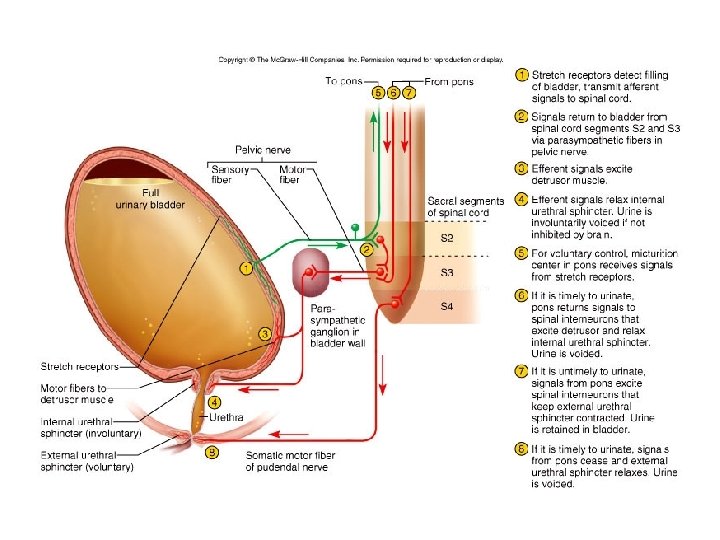
Adult Micturition Reflex Diagram

Cystometrogram

Abnormalities • Atonic bladder Sensory nerve fibers from the bladder to the spinal cord are destroyed Overflow incontinence Crush injury, syphilis,

Automatic bladder • Above the sacral region with intact sacral cord segments • No longer controlled by the brain • Spinal shock • contd.

The urinary bladder looses its tone and becomes flaccid and unresponsive. So, the bladder is completely filled, and later urine overflows by dribbling. After the spinal shock has passed, the voiding reflex returns although there is no voluntary and higher centre control. Whenever, the bladder is filled with some amount of urine, there is automatic evacuation of the bladder. (Spastic neurogenic bladder)

Uninhibited Neurogenic Bladder • Partial damage in the spinal cord or the brain stem • interrupting most of the inhibitory signals • Slight quantity of urine elicits an uncontrollable micturition reflex
 This is normal in infants and children below 3 years.")
Nocturnal micturition (Bed wetting) This is normal in infants and children below 3 years. It occurs due to incomplete myelination of motor nerve fibers of the bladder resulting loss of voluntary control of micturition.

Incontinence from impaired sphincter function • Of lesser degree • In response to sudden rise in intravesical pressure (coughing, sneezing) • After multiple child births in women • After prostatic surgery involving damage to sphincter

- Slides: 46