Lecture 18 Foreign bodies Masses Etc Holdorf Foreign

Lecture 18 Foreign bodies, Masses, Etc. Holdorf
 – Iatrogenic (healthcare provider induced –")
Foreign Bodies • Etiology – Foreign bodies (missiles) – Iatrogenic (healthcare provider induced – Bullets – Knives – Nails – Ice picks, etc. • Pathophysiology – Penetrating missiles may cause: – Myocardial rupture – ASD and or VSD – Valvular disruption – Pericardial effusion (25 -50% will not have a effusion – Coronary artery trauma
 – Murmur possible")
• Physical signs – Bleeding (entrance and possible exit wound) – Murmur possible – Tamponade physiology • ECHO – Missiles may occur anywhere in the heart – look for echogenic structures with strong reverberations – Pericardial effusion not always present – Disrupted valve leaflets/support apparatus – ASD/VSDs may be visualized if large enough – Look for wall motion abnormalities – Always perform a micro-cavitation study to rule out an atrial level shunt – NOTE: – Use x-rays for reference. Use off-axis views

DOPPLER • Intracardiac shunt may be present in the case of missile penetration. • Valvular regurgitation may be present • ASD/VSDs may demonstrate abnormal or turbulent flow • Trans-valvular respiratory flow variations when tamponade physiology is present • NOTE: What part of the heart is most likely to be affected by cardiac contusion? – Right ventricle

Bullet in the heart via CT scan

Bullet in the region of the tricuspid valve
 –")
MASSES • Etiology – Thrombus formation – Benign tumors (most common are myxomas) – Malignant tumors – Primary < 20% – Metastatic (more common) What might be the 1 st indication of metastatic cardiac disease? Pericardial effusion Which cardiac chamber is most likely involved with metastatic tumors? Right atrium The most common benign tumor on the aortic valve is papillary fibroelastoma

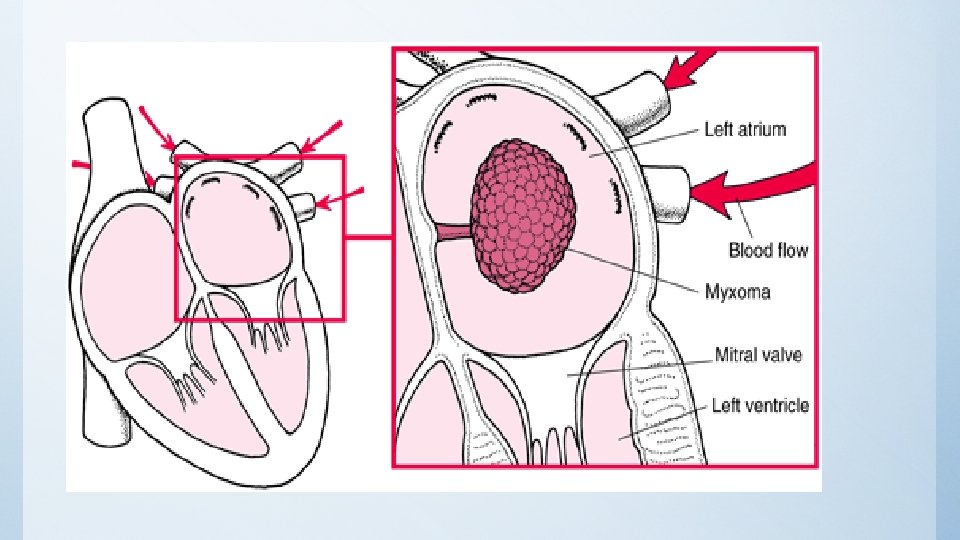
Myxoma

Metastatic tumor

Papillary fibroelastoma

Masses: Pathophysiology • Thrombus may form in areas of Akinesis or dyskinesis • Left atrial thrombi usually associated with MS and left atrial enlargement • Most commonly found at ventricular apex (anterior MI’s) • Papillary fibroelastoma (10% of all primary cardiac tumors – 85% of valve tumors- mostly on Ao. V and MV). • Rhabdomyoma is most common benign tumor in children. • Approximately 20% of primary cardiac tumors are malignant • Metastatic (secondary) are more common than primary • Most metastatic tumors are sarcoma, melanoma or lymphoma from the breast or lung

• Physical Signs: – Valvular stenosis and/or regurgitation may result in murmurs • Echo – Thrombus may be layered, pedunculated, multi-lobulated, or single. – Thrombus will appear as an echogenic mass in areas of Akinesis or dyskinesis – Search ventricular apex closely with a high frequency transducer (5 MHz- short focus) – To rule out artifacts, try to visualize the mass at different depths and from two or more views – Right sided masses can be delineated with micro-cavitation injections. – Angiosarcoma seen most often in the RA: is the most common primary tumor Know how to identify a TEE image of a left atrial appendage clot.

Left atrial appendage

Doppler-Valvular stenosis and or regurgitation may occur with obstructive masses.

Myxomas • Etiology – Benign tumors (comprise 30% of all primary benign cardiac tumors in adults) • Pathophysiology – Over 75% of myxomas are left atrial – Atrial myxomas may mimic mitral stenosis • Physical signs – Malaise/dyspnea – Chest pain (rare) – Dyspnea – Murmur of mitral stenosis with tumor plop is classic (50% of time) – Embolic phenomena(35% of the time) – Know that Myxoma symptoms mimic mitral stenosis

Echo • Atrial myxomas usually attach to the interatrial septum • Intra-cavity tumors will usually move with blood flow • Intra-myocardial tumors usually have borders or texture which is different from myocardium DOPPLER Stenosis and regurgitation may be present with obstructiuve left atrial masses Know that left atrial myxomas are usually attached to the interatrial septum

Left atrial myxoma M-mode
- Slides: 18