LEAKS IN BARIATRIC SURGERY Paolo Gentileschi Bariatric Surgery

LEAKS IN BARIATRIC SURGERY Paolo Gentileschi Bariatric Surgery Unit University of Rome Tor Vergata

LEAKS IN BARIATRIC SURGERY
:")
Chirurgia gastrica in Italia + 142% Buchwald H, Oien DM. Obes Surg 2013; 23(4): 427 -36 www. salute. gov. it
: 427 -36.")
Chirurgia Bariatrica in Europa Buchwald H, Oien DM. Obes Surg 2013; 23(4): 427 -36.
:")
Chirurgia Bariatrica in Italia - 2011 Buchwald H, Oien DM. Obes Surg 2013; 23(4): 427 -36.

LEAKS
 : 0, 28% ü > 30 giorni (tardiva)")
Mortalità ü < 30 giorni (precoce) : 0, 28% ü > 30 giorni (tardiva) : 0, 35% Pazienti Super. Obesi: ü Mortalità Precoce: 1, 25% ü Mortalità Tardiva: 0, 81% Pazienti con età> 65 anni ü Mortalità Precoce: 0, 34% ü Mortalità Tardiva: 0, 0%

Postoperative Adverse Events by Bariatric Procedure in Controlled Trials. Maggard M A et al. Ann Intern Med 2005; 142: 547 -559

Obesity and Risk of Leaks Local and Systemic Factors that negatively influence suture integrity Local Factors Systemic Factors Tissue Hypoperfusion Malnutrition Suture Tension Hypovolemia/Shock Poor Apposition of Suture Edges Chemotherapy Local Infection Peripheral Vascular Disease Radiation Injury Poor Controlled Diabetes Distal Obstruction Renal Failure Glucocorticoids

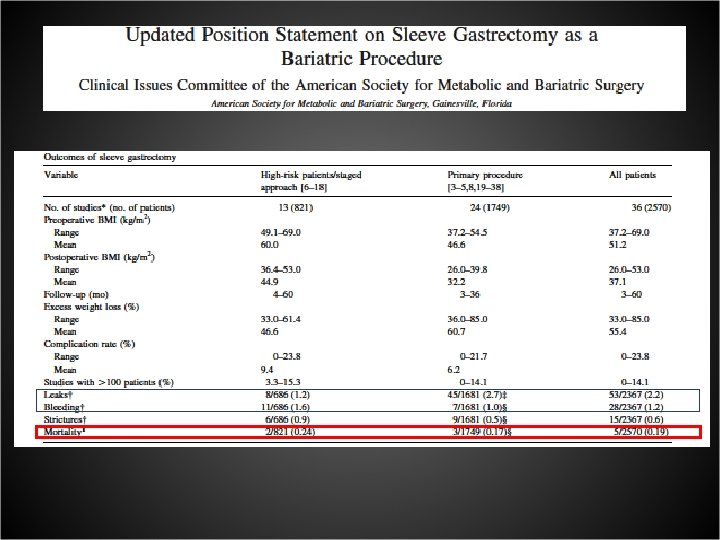
Sleeve Gastrectomy Leaks 0 -6 %

LEAK RATE BY PROCEDURE LAGB 0% LSG 0 -7% LRYGB 0 -7% LBPD 0 -6%

RCTs
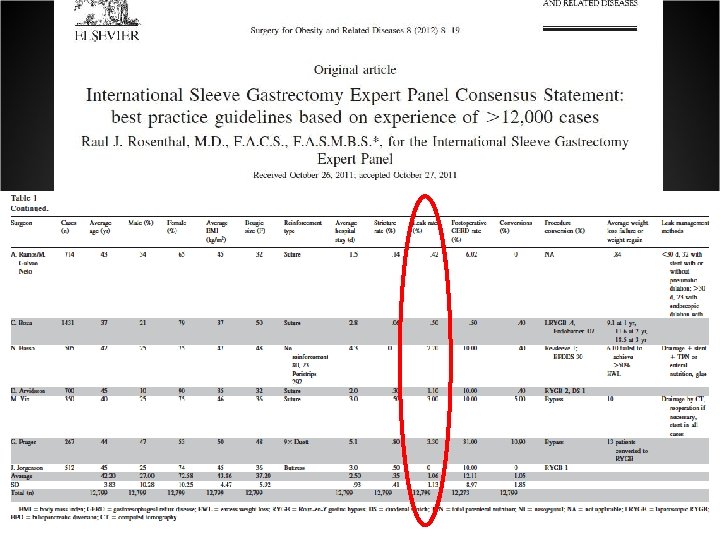

Int’l Consensus Summits on Sleeve Gastrectomy Quest. N. SG/surgeon Sole op. Leak rate Bleeding rate ICSSG-1 Oct 2007 New York 87 7. 500 73. 8± 133. 0 93. 8% 2. 4± 5. 3 1. 4± 2. 6 ICSSG-2 Mar 2009 Miami 106 14. 476 139. 4± 214. 7 86. 3% 2. 0± 3. 3 1. 1± 1. 6 ICSSG-3 Dec 2010 New York 88 19. 605 228. 8± 275. 0 86. 4% 1. 8± 3. 8 2. 0± 5. 0

Comparative Use of Different Techniques for Leaks and Bleeding prevention during Laparoscopic Sleeve Gastrectomy M. Anselmino, N. Basso*, P. Gentileschi°, L. Angrisani§, G. Casella°, D. Benavoli°, S. D’Ugo°, P. Cutolo§, C. Moretto, R. Bellini, R. D. Berta, S. Franceschi Bariatric & Metabolic Surgery Unit, Pisa *VII Dept. of Surgery, Rome La Sapienza §Dept. Of General Surgery, S. G. Bosco Hospital, Naples °Bariatric Surgery Unit, Rome Tor Vergata

Reinforced Sleeve Gastrectomy: Retrospective Multicenter Study All cases of primary SG in 4 Italian Bariatric Centers Center City Investigator A. O. U. P. Pisa Anselmino S. Giovanni Bosco Naples Angrisani Tor Vergata University Rome Gentileschi La Sapienza University Rome Basso
 44,")
Primary Sleeve Gastrectomy 1162 Obese Patients M/F sex ratio 305: 857 Age (years) 44, 1 (15 -72) BMI 47, 0 (27 -84) Gastric Tubule Volume (ml) 80 -110 60 mm firings number 5. 8 (5 -9)

COMPETITIVE LANDSCAPE Company Synovis SI Covidien Gore Baxter Product Brand Name Peri-Strips Dry with Veritas Duet TRS SEAMGUARD Bioabsorbable FLOSEAL TISSEEL Material Bovine Pericardium Synthetic polyester (Biosyn material) Glycolide and Trimethylene Carbonate Copolymer Thrombine Haemostatic matrix + Fibrin Glue Host Tissue Response Remodels Reabsorbs - Tissue thickness Avg = 0. 35 mm 0. 20 – 0. 60 mm Avg = 0. 07 mm 0. 04 – 0. 10 mm 0. 25 mm - Tensile strength (Peak load) 4. 0 kg TBD 1. 2 kg - Storage Controlled room temp Ambient room temp Preparation One piece; requires gel application Pre-loaded on stapler loads; attached with Biosyn sutures Two pieces; sleeves fit on stapler arms

Reinforcement Type Total Type of Reinforcement N. Pts No Reinforcement 189 Oversewing 476 Peri-Strip Dry 312 Duet TRS 76 Seamguard Bioabsorbable 63 Floseal+Tisseel 46 1162

Results Type of Reinforcement N. Pts Leaks % Bleeding % No Reinforcement 189 9 4. 76 26 13. 7 Oversewing 476 14 2. 94 7 1. 47 Peri-Strip Dry 312 1 0. 32 0 0 Duet TRS 76 6 7. 80 1 1. 31 Seamguard Bioabsorbable 63 2 3. 17 1 1. 58 Floseal+Tisseel 46 1 2. 17 0 0 1162 33 2. 83 35 3. 01 Total

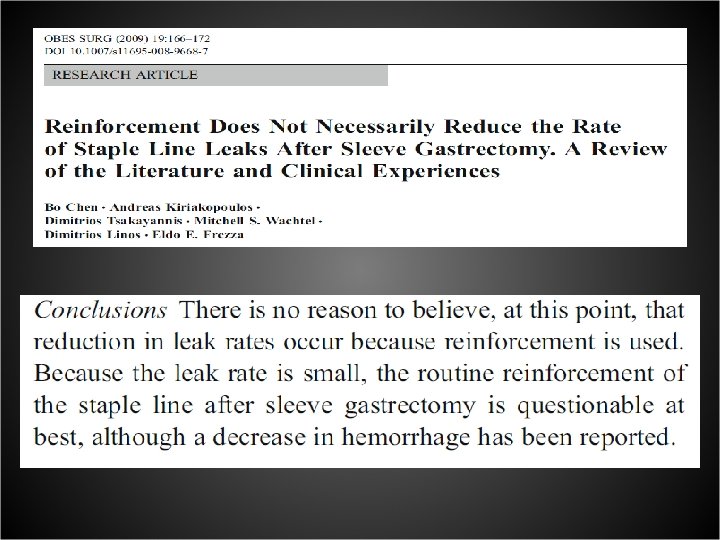
CONCLUSIONS No evidence at this time for minor incidence of leaks with either materials or oversewing - Sufficient evidence of less episodes of bleeding with reinforcement with either strips

LEAKS

Laparoscopic Sleeve Gastrectomy
 March 2013 382 LSG (primary) 6")
Laparoscopic Sleeve Gastrectomy SERIES (Policlinico Tor Vergata Roma) March 2013 382 LSG (primary) 6 LEAKS (1. 5%)

Laparoscopic Sleeve Gastrectomy 5 healed with : 2 with laparoscopic drainage and TPN 3 with endoscopic clipping and stenting 1 Mortality : Pulmonary failure and sepsis

IL BY-PASS GASTRICO
 ü Fistola 2")
Complicanze dopo By Pass gastrico sec. Roux Precoci (entro 30 giorni) ü Fistola 2 -7% ü Embolia polmonare 0, 2 -1% ü Infezione ferita 8% ü Emorragia 0, 8 -4, 4% ü Insufficienza respiratoria 14% Tardive Ernia ferita chirurgica 12 -15% Occlusione intestinale 1 -3% Stenosi delle anastomosi 3 -7% Anemia da carenza di Ferro e/o vitamimina B 12 e/o acido folico 15 -33%* ü Osteoporosi da carenza di calcio 8 -10% * ü Ulcera marginale 1 -16% ü ü
 Marzo 2013 464 pz 1 leak")
LEAKS DOPO BY-PASS GASTRICO Serie (Policlinico Tor Vergata) Marzo 2013 464 pz 1 leak anastomosi gastro-digiunale (0. 2%) Re-intervento, drenaggio, NPT 1 leak anastomosi entero-entero (0. 2%) Re-intervento, riconfezionamento

STENTING

STENTING

Complicanze Precoci: Leak Anastomotici La II causa più comune di morte dopo RYGB ü Leak Anastomosi G-J : Incidenza 2 -5% - LRYGB: 5, 2% - ORYGB: 2, 6% Mortalità 1, 5% Tempo medio per la diagnosi: 2 giorni ü Leak anastomosi J-J Mortalità: 40% Tempo Medio per la diagnosi: 4 giorni Diagnosi Leak anastomotici Segni e/o Sintomi: ü Dolori addominale ü Tachicardia ü Iperpiressia ü Aumentati segni di flogosi: VES, PCR, Pro. Calcitonina ü Leucocitosi Neutrofila ü Distress respiratorio Studio Radiologico: ü Rx digerente con Gastrografin ü Tc con mdc per os

Leak Anastomotici Trattamento Pz Stabile Pz Instabile No segni di shock settico, No segni di ampio Leak Segni shock Settico Segni radiologici di ampio Leack Trattamento Conservativo ü Digiuno ü NPT ü Antibtioticoterapia e. v. ü SNG ü STENT Reintervento Presenza di Raccolta Addominale Drenaggio percutaneo TC-guidato Relaparoscopia Laparotomia Lavaggio raccolte intraddominali Posizionamento di Drenaggi Aspirativi Sutura diretta Leak
 -chronic fistulas (n=2) -strictures")
Treated 19 patients with removable covered stents -acute leaks (n=11) -chronic fistulas (n=2) -strictures (n=6) Leaks were identified endoscopically, marked radiographically, and stents deployed under fluoroscopy. Oral feeding could be started in 79% of the patients after stenting. At a follow up of 3. 6 months successful healing was achieved in : • 91% of acute leaks • 100% of gastrocutaneous fistulas • 81% of strictures Mean healing time of 30 days

Treatment of Leaks and Other Bariatric Complications with Endoluminal Stents Treatment of acute fistola Infected fluid collection Percutaneus or laparoscopic dranaige Acute fistola Applications of stents were extended to treat esophageal and gastrointestinal leaks Healed anastomotic leak after stent removal
 suture buttress material sealants")
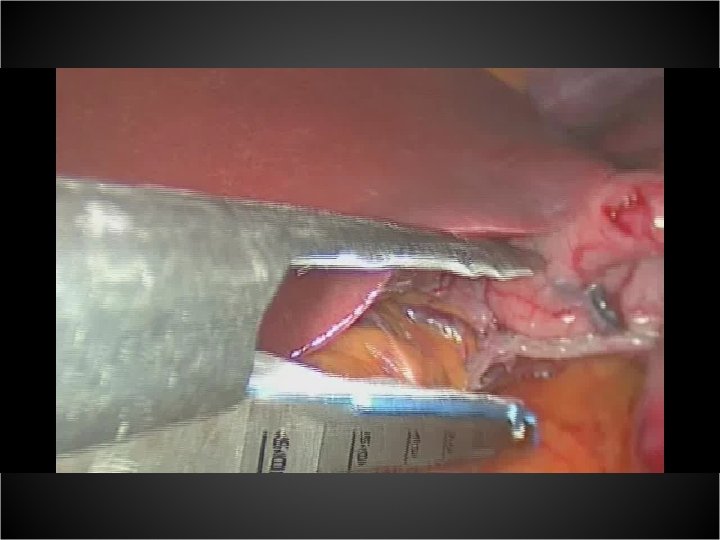
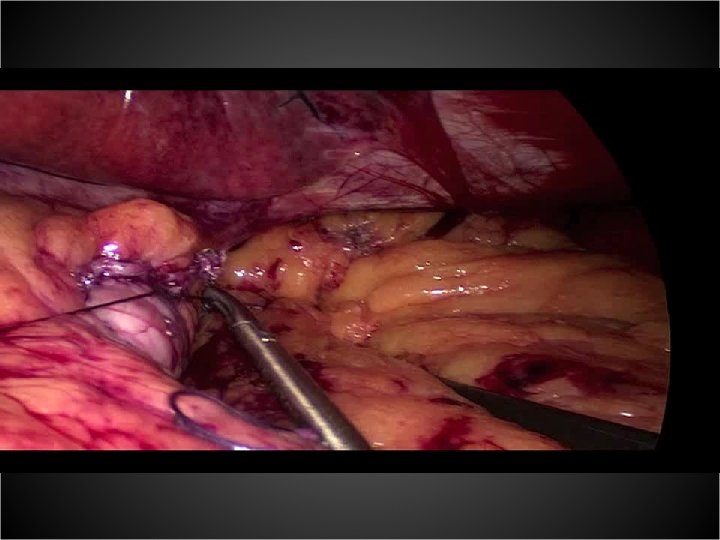
LEAKS PREVENTION APPROPRIATE SURGICAL TECHNIQUE STAPLE LINE REINFORCEMENT (? ) suture buttress material sealants MET BLUE TESTING NG TUBE (? ) DIAGNOSIS ENDOSCOPY WITH FLUOROSCOPY CT SCAN TREATMENT CONSERVATIVE Drainage TPN STENTING Endoscopic clipping or sealants (? )
- Slides: 43