Late preterm infant Is it a trend or

 increased")





 Percent of live births >70% Late")
")
 # 1 Italy: # 2 Australia: #")
 Median rate 33% (quartile range 24– 43)")






 versus Term (37 -40 wk) Khashu, M.")



 Wang, M. L.")

 38 -40 Oxygen > 1 hour Reference")








: 224")
:")


 % * Cerebral Palsy + Mental Retardation")
- Slides: 41
Late preterm infant: Is it a trend or a catastrophe? Michael E. Speer, MD Professor of Pediatrics & Medical Ethics Baylor College of Medicine
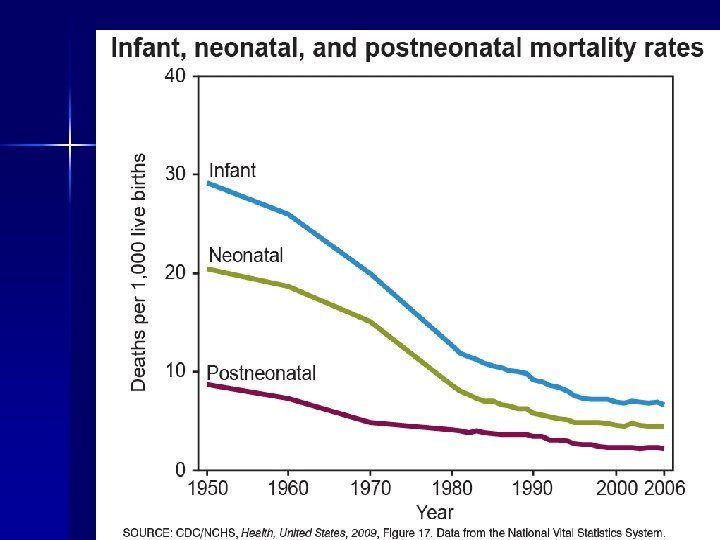
Improved Survival n Survival of extremely low-birth-weight infants (birth weight < 1000 g) increased 35% between the 1980 s and the 1990 s – 85% of infants with very low birth weight (between 500 and 1500 grams) survive Stoelhorst GMSJ, et. al. Pediatrics. 2005 Feb; 115(2): 396 -405.
Improved Survival n Mortality: 1980 s 1990 s – 32 weeks’ gestation: 30% to 11% – <27 weeks’ gestation: 76% to 33% Stoelhorst GMSJ, et. al. Pediatrics. 2005 Feb; 115(2): 396 -405.
Increased Morbidity n Disabilities have also increased between 1980 s & 1990 s – Primarily chronic lung disease and neuro-developmental impairment n n n Sepsis: Periventricular leukomalacia: CLD: (O 2 at 36 wks PMA): Cerebral palsy: Deafness Neurodevelopment impairment* 37% 2% 32% 16% 3% 26% to to to 51% 7% 43% 25% 7% 36% (*major neurosensory abnormality and/or Bayley Mental Developmental Index score of <70) Stoelhorst 2005. Pediatrics. 2005 Feb; 115(2): 396 -405.
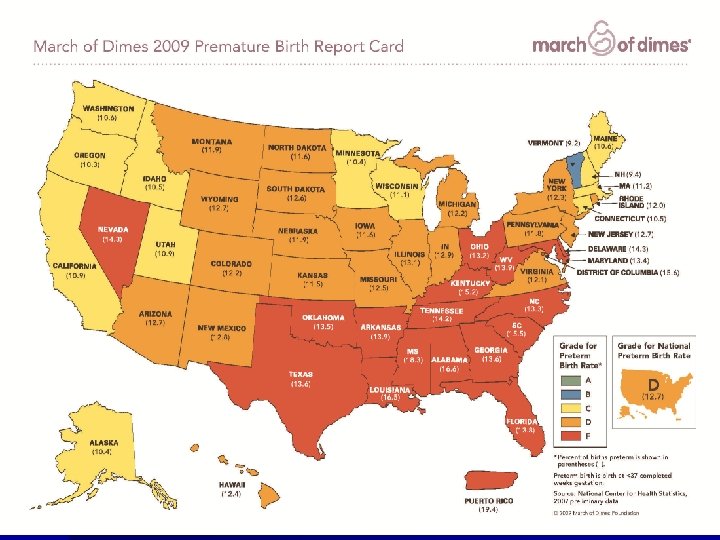
Rising Rate of Prematurity n The preterm birth rate has increased by 36% since the 1980 s* – > 540, 000 each year at present – 21% increase since 1990 (10. 6% to 12. 8%) n Primarily 34 to 36 weeks gestation – Increase of 25% since 1990 *NCHS 2006 final natality data; March of Dimes, 2009
Trends in Late Preterm Birth, Stillbirth, and Infant Mortality: US 1990 -2004 Ananth CV, et al. Am J Obste Gynecol. 2008; 199: 329 -31
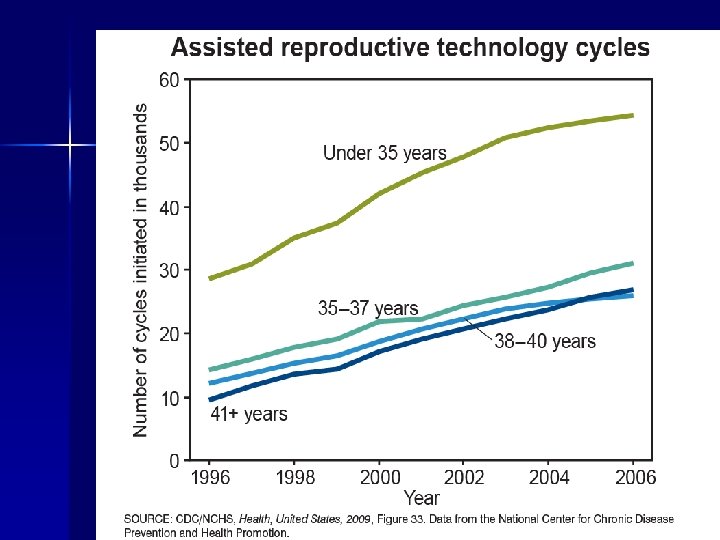
Preterm Birth in the United States: 1996 - 2006
RISE IN LATE PRETERM BIRTHS (34 -36 wks) Percent of live births >70% Late Preterm Source: National Center for Health Statistics Prepared by March of Dimes, Periantal Data Center, 2009 Courtesy of Karla Damus
Percentage of Births by Cesarean: 32% (2007)
Births by caesarean section by country (2000) # 1 Italy: # 2 Australia: # 3 USA: # 4 Germany: # 5 Canada: # 6 Ireland: # 7 New Zealand: # 8 Austria: # 9 France: # 10 United Kingdom: # 11 Belgium: # 12 Finland: # 13 Denmark: # 14 Sweden: # 15 Norway: # 16 Netherlands: 333 live births per 1, 000 217 live births per 1, 000 211 live births per 1, 000 209 live births per 1, 000 205 live births per 1, 000 204 live births per 1, 000 202 live births per 1, 000 171 live births per 1, 000 170 live births per 1, 000 159 live births per 1, 000 157 live births per 1, 000 145 live births per 1, 000 144 live births per 1, 000 137 live births per 1, 000 129 live births per 1, 000 (33. 3%) (21. 7%) (21. 1%) (20. 9%) (20. 5%) (20. 4%) (20. 2%) (17. 1%) (17. 0%) (15. 9%) (15. 7%) (14. 5%) (14. 4%) (13. 7%) (12. 9%) Weighted average: 185. 3 live births per 1, 000 (18. 5%)
Cesarean Section Rates – Latin America (2005) Median rate 33% (quartile range 24– 43) Elective 49% Intrapartum 46% Emerg. s Labour 5% Lancet. 2006; 367: 1819 -29
World Wide Cesarean Section Rates - WHO n Asia – 27. 3% (2007 – 2008)* – – n China Sri Lanka Viet Nam Thailand 46. 2% 30. 6% 35. 6% 34. 1% Latin America – 35% (2005) – Brazil n 36% (2009) Private clinic rate: >90% – Ecuador – Paraguay 40% (2005) 42% (2005) *Lancet. 2010; 375: Pages 490 -499
Rates are not necessarily current http: //blog. fortiusone. com/2009/04/22/birth-in-the-usa/
Risk of Placenta Accreta and Hysterectomy by Number of Cesarean Deliveries Compared with the First Cesarean Delivery Cesarean Section Accreta [n(%)] Odds Ratio Hysterectomy [n(%]) Odds Ratio 40 (0. 7) First 15 (0. 2) Second 49 (0. 3) 1. 3 (. 7– 2. 3) 67 (0. 4) 0. 7 (0. 4– 0. 97) Third 36 (0. 6) 2. 4 (1. 3– 4. 3) 57 (0. 9) 1. 4 (0. 9– 1. 2) Fourth 31 (2. 1) 9. 0 (4. 8– 16. 7) 35 (2. 4) 3. 8 (2. 4– 6. 0) Fifth 6 (2. 3) 9. 8 (3. 8– 25. 5) 9 (3. 5) 5. 6 (2. 7– 11. 6) Six or More 6 (6. 7) 29. 8 (11. 3– 78. 7) 8 (9. 0) 15. 2 (6. 9– 33. 5) Obstet Gynecol 2006; 107: 1226– 32.
Indications for Late Preterm Birth 48. 9 % 23. 2 14. 4 15. 9 1. 3 Reddy U, et al. Pediatrics. 2009; 124: 234 -9
Clinical Issues n Risks of Elective Delivery – 13, 258 Elective Cesarean Sections n Rates of adverse respiratory outcomes, mechanical ventilation, sepsis, hypoglycemia, NICU admission, and hospitalization for 5 days or more. n n Increased by a factor of 1. 8 to 4. 2 for births at 37 weeks Increased by a factor of 1. 3 to 2. 1 for births at 38 weeks. Tita A, et al. NEJM. 2009; 360: 111 -120
Clinical Issues http: //www. femalepatient. com/html/arc/sig/Pat. S/articles/034_09_041. asp
Mortality Higher in Preterm (33 -36 wk) versus Term (37 -40 wk) Khashu, M. et al. Pediatrics 2009; 123: 109 -113
Mortality: Late Preterm vs Term Infant: 1995 -2002 Mortality/1000 live births Late PT Term Ratio Overall (0 – 364 days) 7. 9 2. 4 3 x Early neonatal (0 – 6 days) 2. 8 0. 5 6 x Late neonatal (7 – 27 days) 1. 4 0. 4 3 x Post neonatal (28 -364 days) 3. 7 1. 6 2 x Tomashak KM. J Pediatr 2007; 151; 450
RR of morbidity, preterm versus term Khashu, M. et al. Pediatrics 2009; 123: 109 -113
Proportion with newborn morbidity during birth hospitalization according to gestational age Shapiro-Mendoza, C. K. et al. Pediatrics 2008; 121: e 223 -e 232
Clinical outcomes in near-term and full-term infants (% of patients studied) Wang, M. L. et al. Pediatrics 2004; 114: 372 -376
Early Respiratory Morbidity in Late Preterm Infants Weeks of Gestation 34 35 36 37 39 TTN (%) 2. 4 1. 6 1. 1 0. 7 0. 4 Ventilator (%) 3. 3 1. 7 0. 8 0. 5 0. 3 Mc. Intire & Leveno. Obstet. Gynecol. 2008; 111: 35 -41
Early Respiratory Morbidity Odds Ratios GA (wk) 38 -40 Oxygen > 1 hour Reference Assisted Ventilation Reference 37 2. 04 (1. 61 -2. 59) 2. 35 (1. 84 -3. 02) 36 4. 95 (3. 95 -6. 21) 5. 24 (4. 11 -6. 68) 35 8. 76 (6. 77 -11. 4) 0. 04 (6. 88 -11. 9) 34 18. 67 (14 -24. 9) 19. 8 (14. 7 -26. 6) Escobar GJ. Semin Perinatal. 2006; 30: 28 -33
Early & Late Nutritional Morbidity n n n n Inadequate caloric intake: – Poor suck/swallow coordination – Fatigue Feeding intolerance – Delayed stooling – Feeding residuals Exaggerated physiologic jaundice Dehydration Hypernatremia Increased need for parenteral nutrition Failure to thrive
Breastfeeding Issues n n n Decreased milk production Poor latch Poor sucking effort Poor coordination Potential alteration in bonding
Neonatal gestational age versus length of hospital stay Wang, M. L. et al. Pediatrics 2004; 114: 372 -376
Primary Reason Documented for Discharge Delay of Near-Term and Full-Term Neonates Primary Reason for Delay of Discharge Near Term Full Term Jaundice 8/49 (16. 3%) 1/36 (0. 03%) Respiratory distress 8/26 (30. 8%) 2/4 (50%) Poor feeding 22/29 (75. 9%) 2/7 (28. 6%) 50 7 Neonates (total) with discharge delay Comment P =. 072; 95% CI: 0. 083– 311. 1; OR: 6. 71 P =. 58; 95% CI: 0. 03 – 7. 36; OR: 0. 46 P =. 029; 95% CI: 0. 94– 93. 4; OR: 7 Wang, M. L. et al. Pediatrics 2004; 114: 372 -376
GA at Presentation to ED: 2003 Jain S. Clinics in Perinatology. 2006; 33: 935 -945
Lung Maturation n Pulmonary – Persistent airway obstruction demonstrated in healthy premature infants ( 36 wk GA) compared with infants born at term: weeks after birth: FEF in healthy 30– 34 wk GA infants (P<0. 001)1 n 6– 10 age 1: Vmax. FRC in healthy 29– 36 wk GA infants (P<0. 05)2 n At FEF: forced expiratory flow; V max. FRC: maximal expiratory flow at functional residual capacity. 1. Friedrich L, et al. Am J Resp Crit Care Med. 2006; 173: 442 -447. 2 2. Hoo A-F, et al. J Pediatr. 2002; 141: 652 -658.
Risk of Infection: RSV-related Hospitalizations per 100 Children <6 Months of Age Infection 56. 3 *Retrospective study of enrollees in Tennessee Medicaid, July 1989 -June 1993. **Low-risk defined as all other children born at term. 12. 1 BPD CHD 9. 4 £ 28 wks GA 8. 2 8. 0 29 to <33 wks GA 33 to <36 wks GA 4. 4 Low-risk** Boyce TG, et al. J Pediatr. 2000; 137: 865 -870.
Changes in brain volume and maturation with increasing gestational age Kapelloou, O et al. PLOS Med 2006; 3: e 265
Brain Growth During Gestation Hüppi PS, et al. Ann Neurol. 1998 Feb; 43(2): 224 -35.
Neurologic Maturation: Cerebral White Matter Hüppi PS, et al. Ann Neurol. 1998 Feb; 43(2): 224 -35.
Neurologic Maturation From Conel, 1939 -59
Neurodevelopmental Early School-Age Outcome Developmental delay/disability Age % Late Preterm N=7152 % Term N=152, 661 Unadjusted RR [95% CI] Adjusted RR [95% CI] 0– 3 4. 24 2. 96 1. 43 (1. 36– 1. 51) 1. 36 (1. 29– 1. 43) Disability in prekindergarten 3 4. 46 3. 89 1. 15 (1. 09– 1. 20) 1. 13 (1. 08– 1. 19) Disability in prekindergarten 4 7. 40 6. 60 1. 12 (1. 08– 1. 16) 1. 10 (1. 05– 1. 14) Not ready to start school 4 5. 09 4. 40 1. 16 (1. 11– 1. 21) 1. 04 (1. 00– 1. 09) Exceptional student education 5 13. 30 11. 9 1. 13 (1. 09– 1. 16) 1. 10 (1. 07– 1. 13) Retention in kindergarten 5 7. 96 6. 17 1. 29 (1. 24– 1. 34) 1. 11 (1. 07– 1. 15) Suspension in kindergarten 5 1. 80 1. 22 1. 48 (1. 37– 1. 60) 1. 19 (1. 10– 1. 29) Morse SB et al. Pediatrics. 2009; 123: e 622 -e 629
Disabilities Related to GA at Birth (Adults) % * Cerebral Palsy + Mental Retardation ^ Disability Affecting Work # Other Major Disability *RR: 2. 7(2. 2 – 3. 3) +RR: 1. 6(1. 4 – 1. 8) ^RR: 1. 4(1. 3 – 1. 5) #RR: 1. 5(1. 2 – 1. 8) Moster D et al. NEJM. 2008; 359: 262 -273