LATE PRETERM AND EARLY TERM INFANTS Hugo A



















- Slides: 31
LATE PRETERM AND EARLY TERM INFANTS Hugo A. Navarro, M. D. Medical Director SCN Alamance Regional Medical Center Assistant Professor DUMC
Goals Ø Increase awareness of vulnerability in late preterm and early term infants Ø Definition and incidence Ø Discuss physiologic limitations Ø Morbidity and Mortality Ø Questions
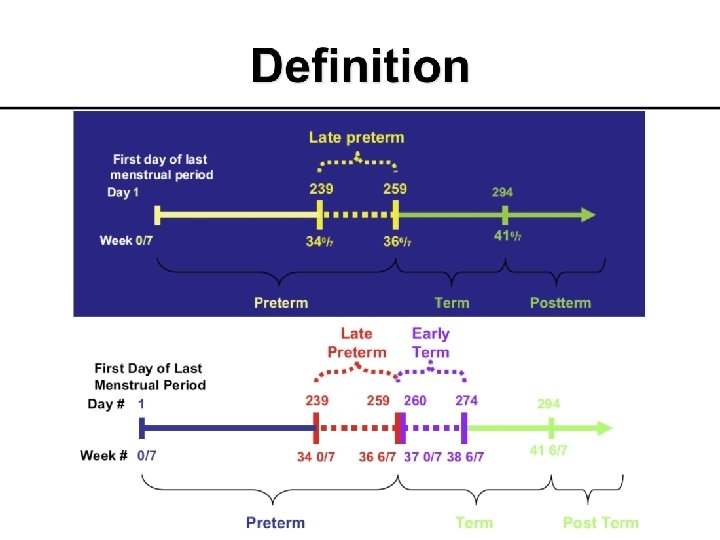
Incidence of early term birth Ø Births of infants > 40 weeks gestation has declined, whereas the early term infants has increased Ø Approximately 700, 000 births/year in USA (17. 5% of live births) occur 37 0/7 -38 6/7 weeks of gestation
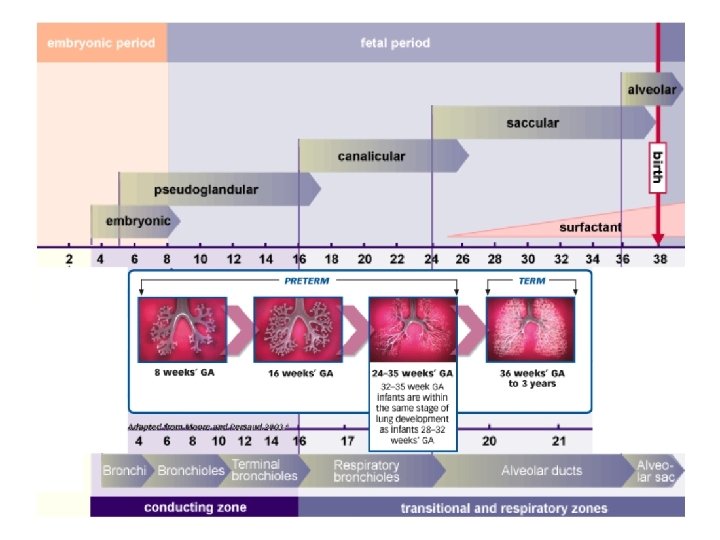
Why? Ø Is multifactorial: Ø Increased surveillance and medical interventions Ø Inaccurate gestational age estimates Ø Presumption of fetal maturity at 34 weeks’ gestation Ø Changes in maternal demographics and health
Why? 1. Increased rates of elective cesarean sections and inductions of labor 2. Maternal and physician concerns about complications of vaginal delivery and subtle changes in medical thresholds for cesarean birth 3. Willingness of mothers to incur risk on behalf of their child
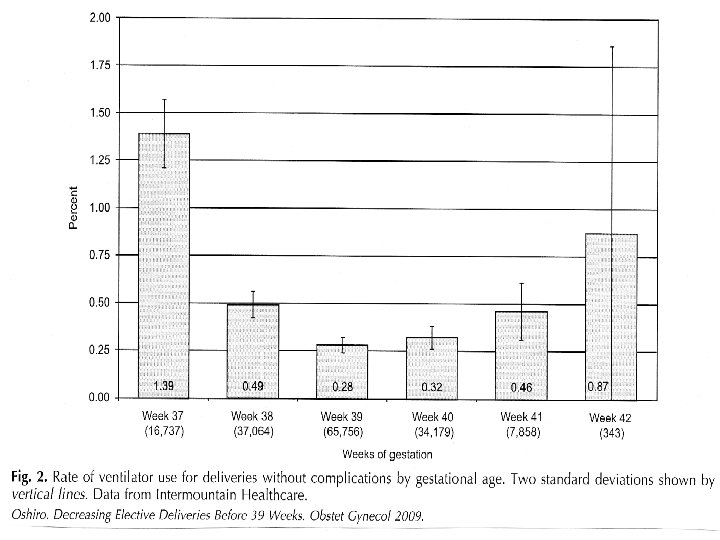
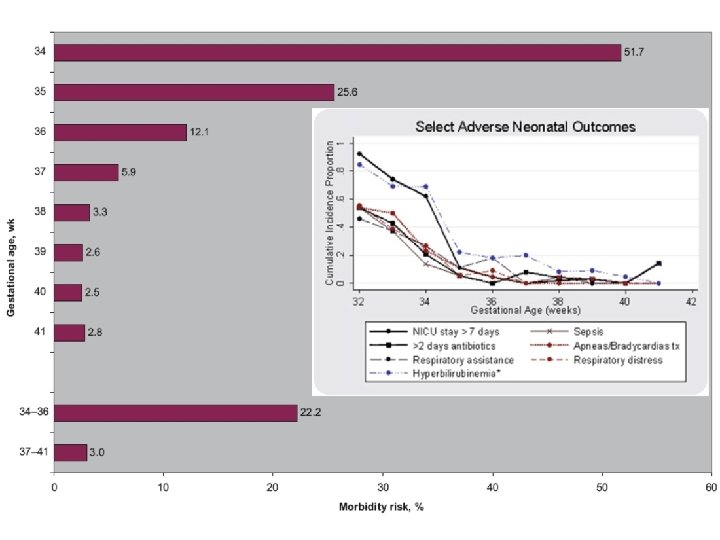
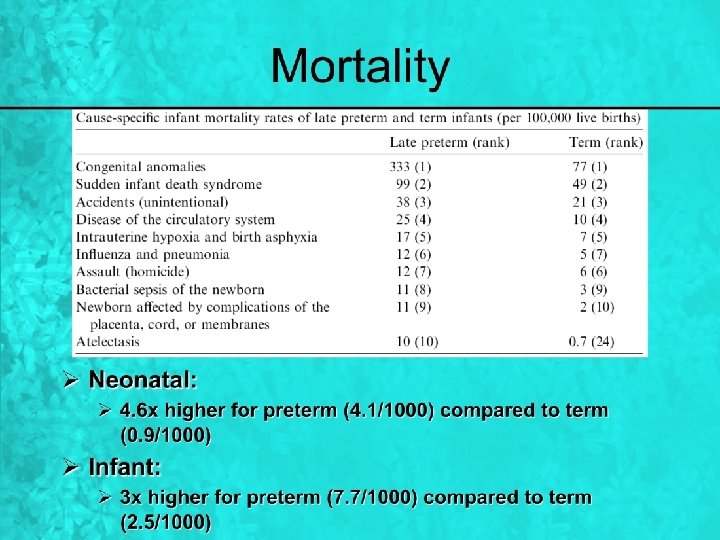
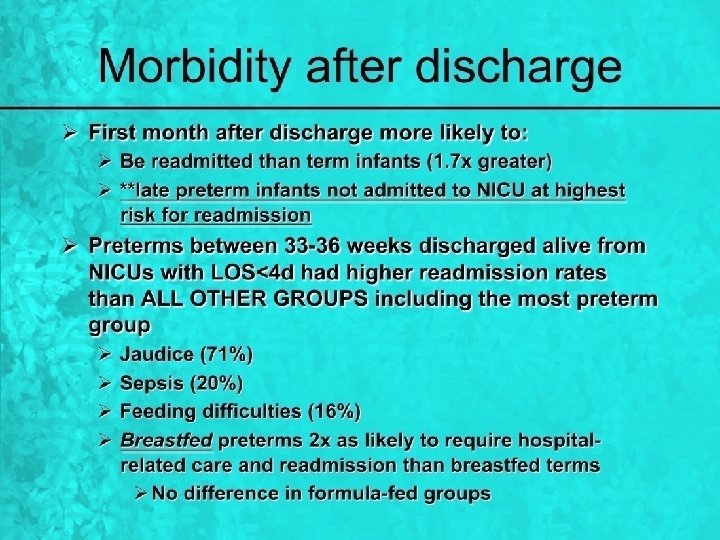
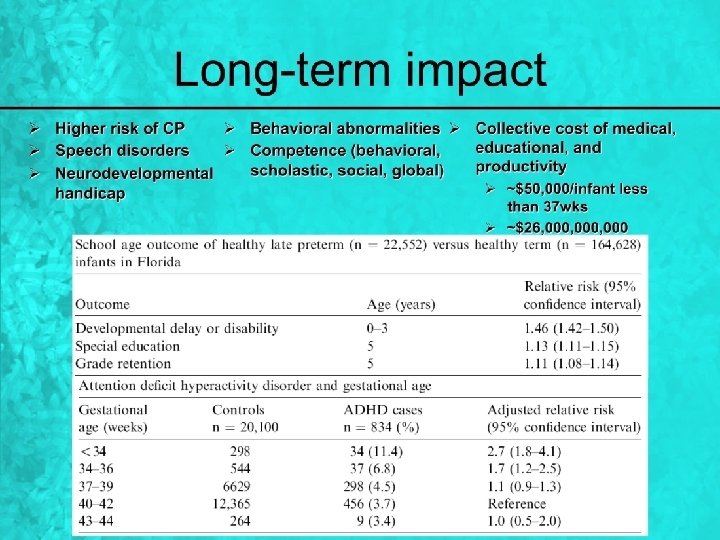
Preterm ≠ LPT ≠ ET ≠ Term ↑risk for medical complications that result in higher morbidity and mortality during birth hospitalization The ↑ in LPT and ET, raises the risk for physiologically immature infants ↑admissions to NICU and duration of hospital stay, disrupting the infant-family bonding ↑ rates of readmission during the neonatal period ↑long-term complications
Most common problems/treatments in descending order Feeding problems Respiratory distress Evaluation for sepsis Intravenous fluids Jaundice Hypoglycemia Temperature instability Apnea Mechanical ventilation
POOR FEEDER Lower the GA worst the feeding skills Dehydration Hyperthermia Hypoglycemia Hyperbilirubinemia IV fluids Antibiotics Phototherapy ADMISSION
Summary 1. LPT and ET infants are at greater risk than term infants for acute and long-term complications of premature birth 2. The rates of LPT and ET births are increasing 3. Causes for the increase in rates of LPT and ET infants are unclear 4. The route and timing of delivery of LPT and ET NB infants have important implications for short-term and long-term neonatal outcomes
Summary Ø The risks and benefits for planned induction of labor, or elective cesarean section for mother and infant should be carefully considered by mothers, families, and physicians when determining the optimal timing and route of delivery Ø Our understanding of the maternal, fetal, neonatal, and long-term outcomes and causes of LPT and ET births is incomplete
Summary Ø Research is needed to increase our understanding of maternal and infant outcomes of infants born at 34 to 38 weeks’ gestation, to determine the efficacy and safety of strategies to optimize these outcomes, and to develop interventions that effect physiologic maturation of the fetus when premature delivery is necessary or elective