Laser Therapy of Perforator Veins Michael F Bardwil

Laser Therapy of Perforator Veins Michael F. Bardwil M. D. , F. A. C. S.

Current Treatment of Veins

Saphenous Veins Laser Ablation

Varicose Veins • Phlebectomy • Foam Sclerotherapy

Telangectasia and Reticular Veins Sclerotherapy

Perforator Veins Next area in treatment of veins

Why does Vein Surgery Have Such a Bad Reputation? • Historically the procedures were morbid • High incidence of recurrence perceived as bad results • Severe forms of venous insufficiency including refluxing perforators resulted in recurring stasis ulcers

Perforators Give Veins A Bad Name • Linton procedure had a reported 19% wound complication rate

Perforators Give Veins A Bad Name • Perforators are a more likely source for recurrent varicose veins than neo-vascularsation • Recurrence is perceived as bad results

Perforators Give Veins A Bad Name • Severe forms of venous insufficiency including refluxing perforator veins resulted in recurring stasis ulcers

Significance of Perforator Veins • Source for reflux in the superficial venous system • Reflux from perforator veins has been associated with venous stasis ulcers • Communication between deep and superficial venous Systems • Reflux from perforator veins can result in varicose veins

Communication Between Venous Systems • Not all bad • Allows patients to recover from vein insults such as injuries and DVT • Allows us to perform vein ablative procedures on the saphenous and other superficial veins

Communication Between Venous Systems • • Not all good Source for reflux in the saphenous vein Associated with venous stasis ulcers Reflux from perforators can cause non saphenous varicose veins • Source for new and recurrent varicose veins

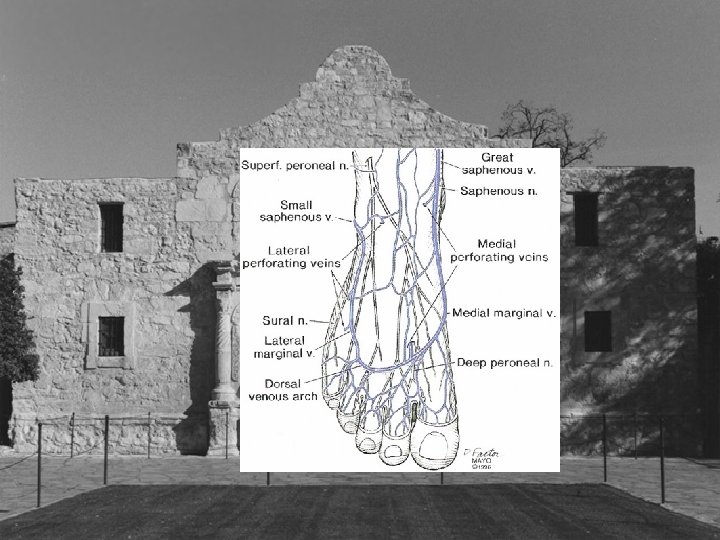
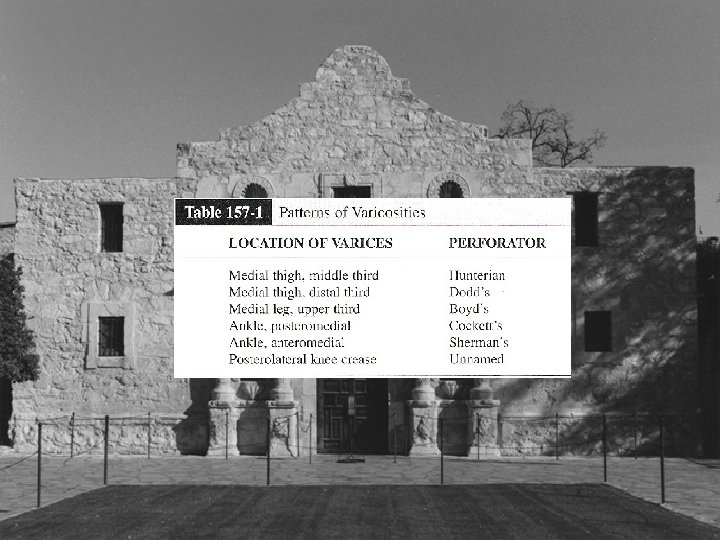
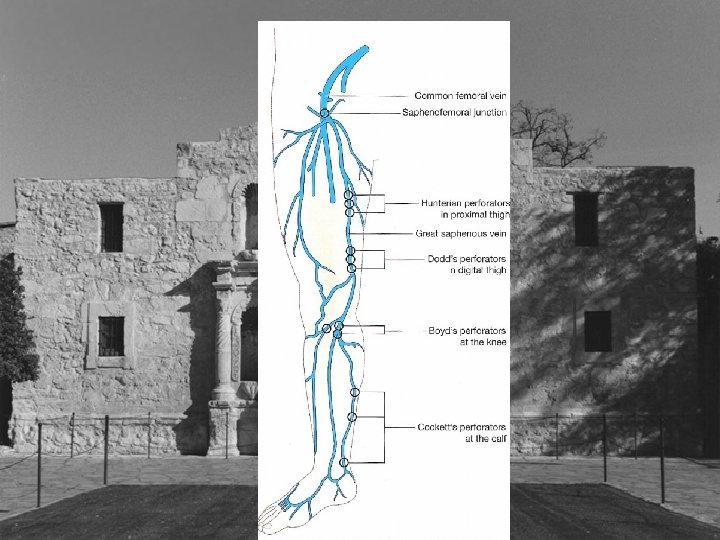
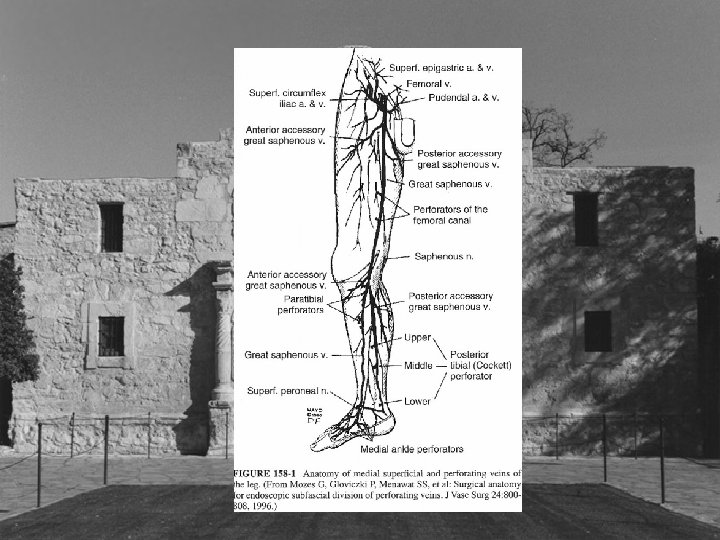
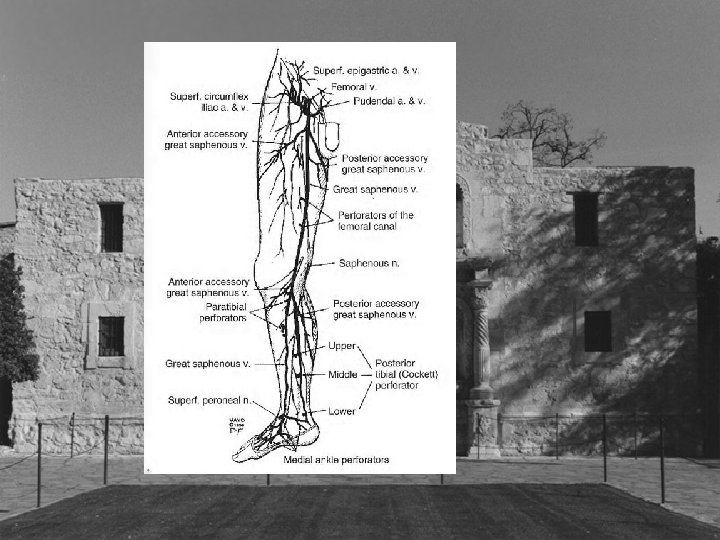
Types of Perforators • • • Hunterian Dodd’s Boyd Cockett’s New Nomenclature
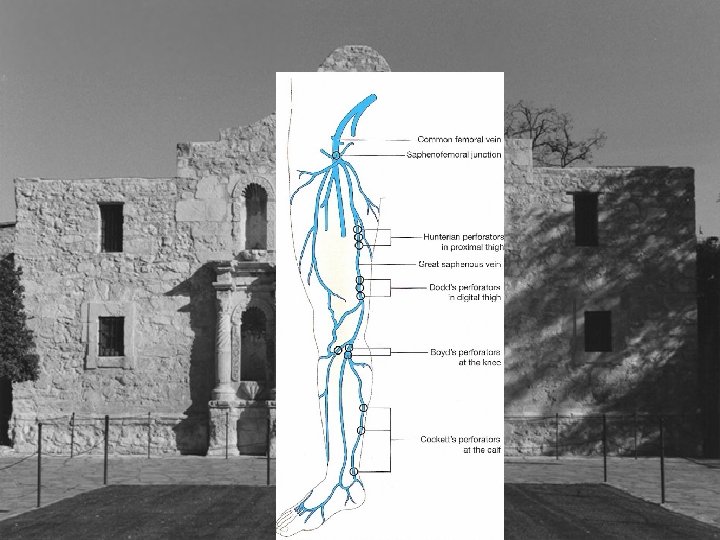

Hunterian and Dodd’s Perforator • Connect femoral and proximal popliteal perforators to the saphenous vein • Reflux from these perforator veins results in varicose veins in the middle and distal third of the medial thigh • Stripping reportedly interrupts all but 8%?

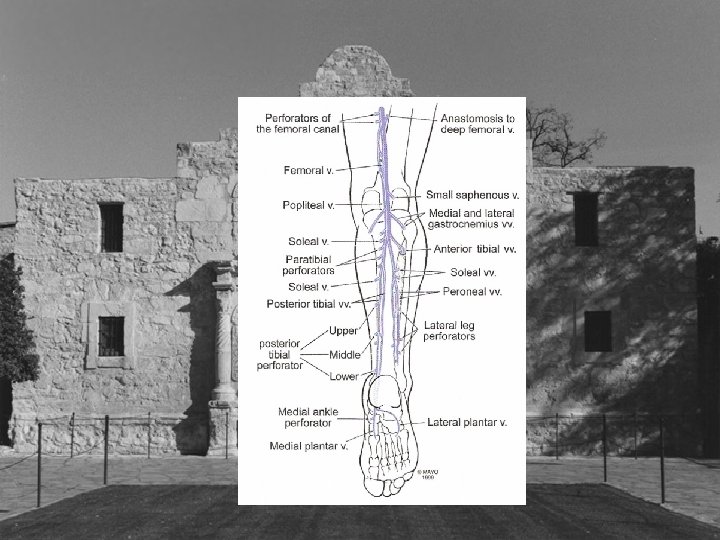
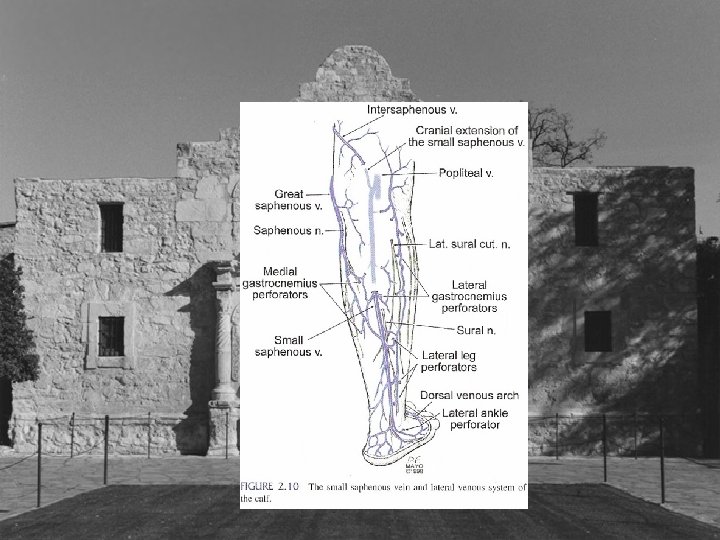
Boyd’s Perforators • Perforator just distal to the knee • Connects saphenous veins to popliteal vein • Varicose veins medial leg upper third • May appear as first place isolated reflux • New nomenclature Paratibial perforators
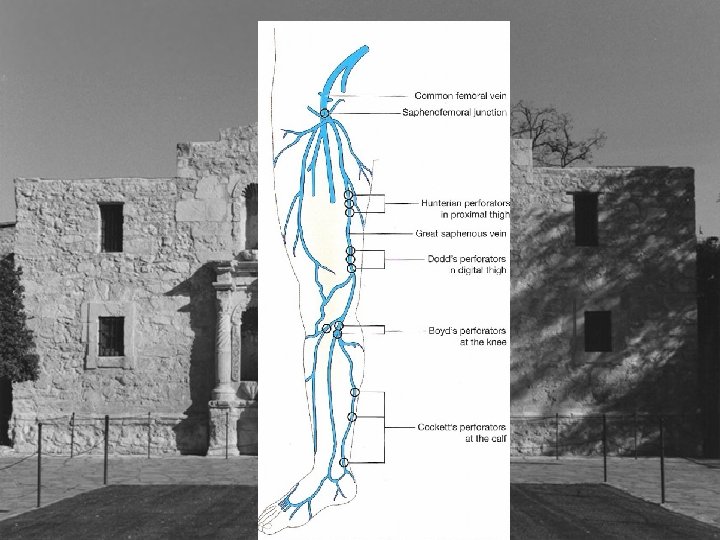
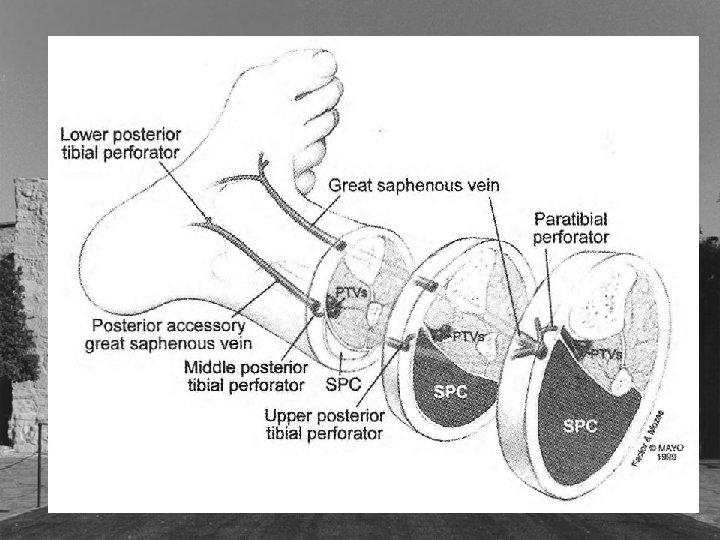

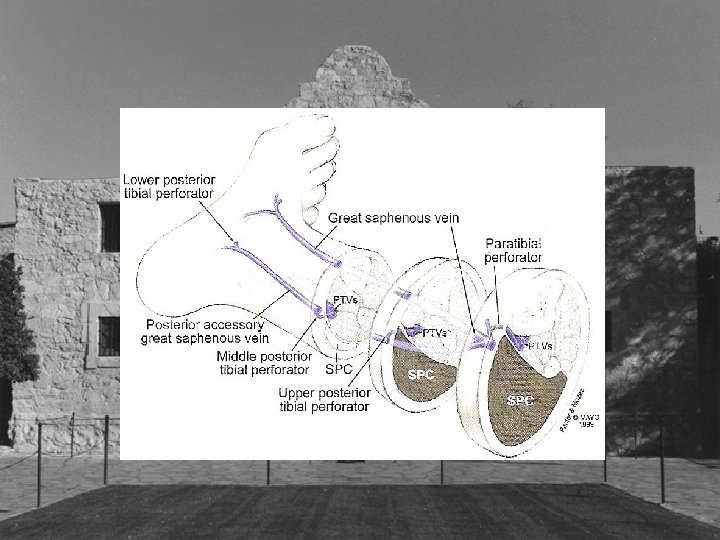
Cockett’s Perforators • Cockett’s I perforator posterior to medial malleolus • Cockett’s II perforator 7 -9 cm proximal • Cockett’s III perforator 10 -12 cm proximal • New nomenclature posterior tibial
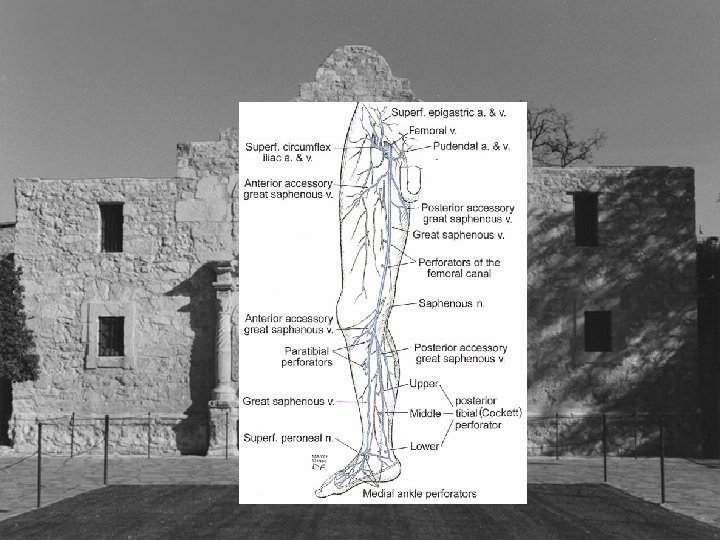

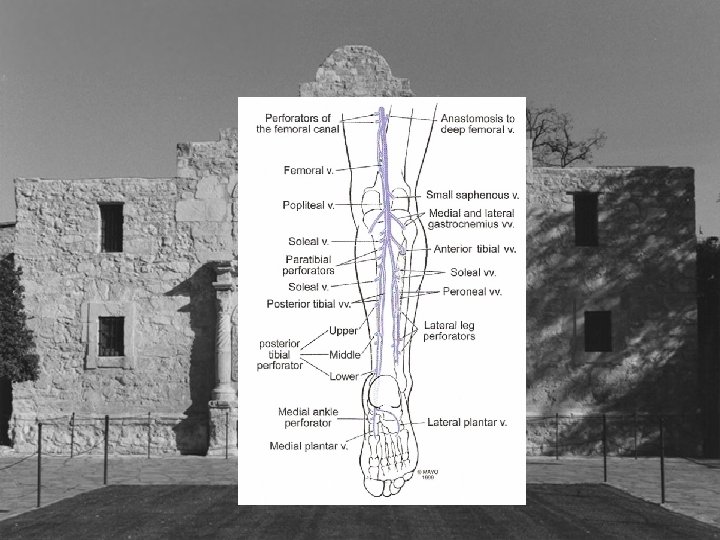
Less Discussed Perforators

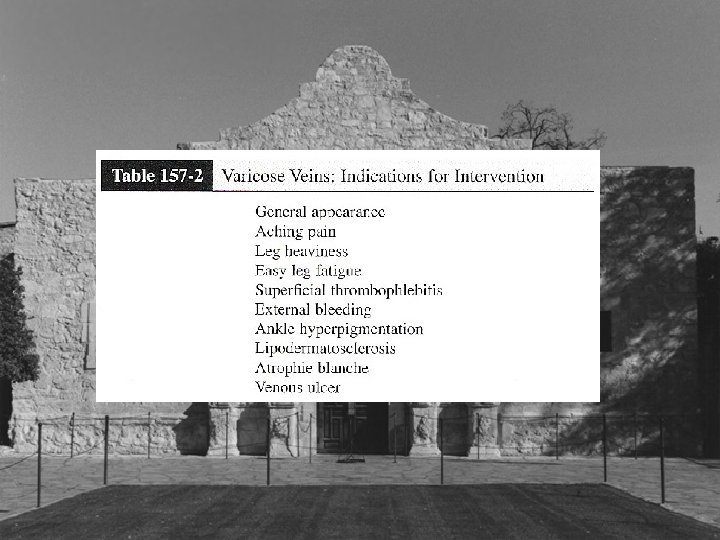
Indications for Treatment • Venous Stasis Ulcer associated with perforator vein 2 -4 mm in size

Indication for Treatment • Large perforator vein 3 -4 mm noted at the time of saphenous ablation • Refluxing perforator 2 -4 mm noted at saphenous ablation

Indications For Treatment • Perforator veins refluxing into varicose veins that are not associated with long or short saphenous reflux

Indications for treatment • Recurrent varicose veins that appear to originating from refluxing perforator

Indication for Treatment • Perforator veins refluxing into varicose veins that are not associated with long or short saphenous vein reflux • Large perforator veins 2 -4 mm noted at time of saphenous ablation • Recurrent varicose veins that appear to be originating from perforator • Stasis ulcers associated with perforator

History • Standard questions regarding symptoms • Previous vein surgery • Stasis Ulcers and previous treatment

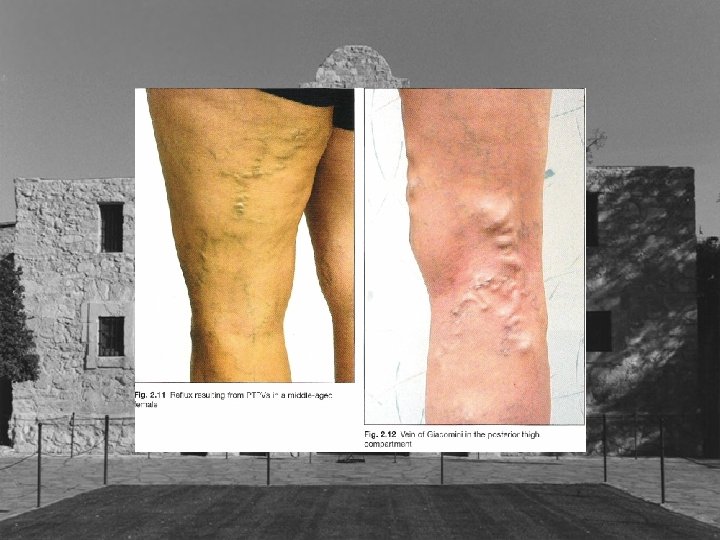
Examination • Physical exam with attention to pattern of varicose veins • Use the ultrasound as an extension of the physical exam • Photograph markings of perforator to be treated • Ulcers • PPG to physiologically document venous insufficiency

Problems with Perforator Rx • Linton procedure problem with wound healing • SEPS general anesthesia required inconsistent results • Ultrasound guided foam multiple sessions inconsistent results, non approved solution no code for reimbursement

Future Meets Past • • • In office procedure to treat perforators Less morbid Addresses non saphenous varicose Veins Addresses sources of recurrence Addresses stasis ulcers

Endoluminal Ablation Perforators

Endoluminal Ablation of Perforators • • • Minimally invasive procedures Office based Local anesthesia VNUS Closure Laser ablation My experience

VNUS Closure • Device FDA approved • Billing Code recommendation • Recommended protocol using ultrasound guidance and impedance to verify position

Disadvantage VNUS Closure • Device awkward and expensive, especially for add on perforator veins • Protocol less effective than thought • Impedance less useful than flash • In general other closure procedures have inferior results to laser

Laser Perforator • Technically simpler • Less expensive to perform; can treat perforator at time of other veins and not incur increase procedural costs • Results should be superior to closure

Technical Issues • • Visualization Broad based neck Multiple perforator necks Long Perforator necks

Technique My Experience • • Micro puncture kit Angio catheter 18 gauge thin wall angiogram needle 25 gauge “finder” needle 20 gauge needle with 400 u fiber 20 gauge needle with 600 u fiber Laser setting Use of foam

Micro-Introducer • Advantage theoretically similar Elas • Disadvantage not enough room to place guide wire in far enough for introducer Dr. Murphy technique use stiff end of guide wire

Angiocath • Advantage: Able to place without guide wire • Disadvantage: Needle may be in, but laser not. Work with VNUS device demonstrated proximity still only applies to horse shoes and hand grenades

18 gauge Angiogram Needle • Advantage: Direct access to vein • Disadvantage: Still bulky, at times difficult getting fiber through needle

20 Gauge Needle 400 u Fiber • Advantage: Easier to use technically to access vessel • Can access vessel at more than one spot • Disadvantage: Inconsistent delivery of Energy if Laser system made for 600 u fiber

How I Do It • Always perform the venous duplex yourself • Mark the vein with patient standing or sitting with feet dangling • Strategically position patient • Put the bed in reverse trendlenberg

How I Do It • Re-map and mark patient in new position • Use 25 gauge “finder” needle • Place previously 2 inch stripped fiber through 20 gauge needle and mark with steri-strip • Access vein with 20 gauge needle, use more than one needle if necessary • Inject local anesthesia after you are in vein

How I Do It • Laser setting 15 watts intermittent 1. 5 sec duration, 1 sec rest • Look for steam in vessel • I usually deliver 200 -300 joules • Steri strip applied. 4 x 4, kerlex, co-ban

Follow Up • 1 -2 days remove wrap and ultrasound • Low threshold to use foam at time of this exam

Results • In progress


- Slides: 60