Laryngectomy Awareness Session Mairi Mascarenhas Clinical Educator ICU















 through the back wall of the trachea")
 removed – communication methods will vary between each")









- Slides: 27
Laryngectomy Awareness Session Mairi Mascarenhas Clinical Educator ICU Department of Critical Care 2018
Make the safety of the patient everyone’s highest priority As a minimum standard, it is recommended that every member of staff refers to this presentation as a means of improving their awareness of how to safely manage patients with a laryngectomy. It is also recommended that nursing staff should refer to this presentation each time a patient with a laryngectomy is admitted.
Learning objectives: Raise awareness of the anatomical differences in laryngectomy patients. Understand the basic methods of administering oxygen therapy. Understand the appropriate management of the airway during respiratory emergencies. Appreciate the need to adhere to the recommended safety measures. Familiarisation with documentation used when a laryngectomy patient is admitted to your area.
“Laryngectomees”or “Neck Breathers” A person with a laryngectomy has had the voice box or larynx removed. This may be required as part of the treatment of cancer, burns, injury or infection.
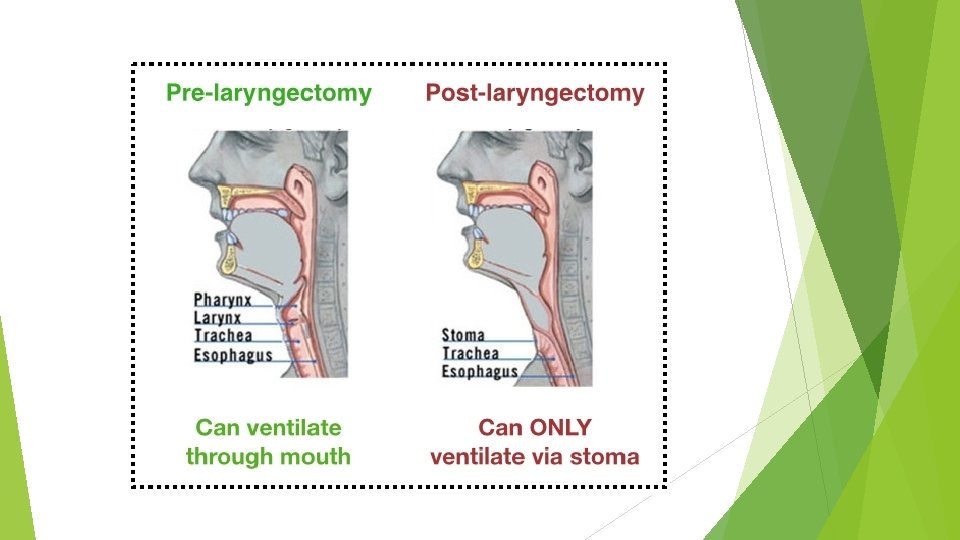
Normal airflow prior to surgery: Normal airflow – air flows between the nose and the mouth and there is a direct passage towards the lungs. Surgery involves removing the larynx and forming a stoma in the patient’s neck.
Airflow following surgery: The upper portion of the trachea is brought to the stoma and secured, making a permanent airway for air to get to the lungs. The nature of the surgery means that there is no longer a direct connection between the oral or nasal passages and the trachea. Following surgery, the patient can no longer breathe via the nose or the mouth. The only way that the patient can now breathe is through the stoma or the hole in their neck.
Laryngectomy stoma: In the event that the patient is admitted to hospital and requires oxygen therapy, nebuliser therapy or artificial ventilation – these treatments MUST only be delivered directly via the stoma.
Simple oxygen therapy using a tracheostomy mask Humidified oxygen is delivered via the tracheostomy mask. Tracheostomy masks are available from the ENT ward. This mask should not be used if the patient has a cuffed tracheostomy tube in situ (rare) and relates to a Safety Action notice from 1998.
Maintain adequate humidification: Press the button immediately next to the tube and mask icons. Confirm that the mask setting has been selected. After sufficient warm-up time, the temperature displayed on the humidifier should approximate 31˚C
Trachi-naze devices: The trachi-naze is a heat moisture exchanger. This helps maintain heat, moisture and filtration. Designed to help clear mucous secretions – and also to reduce coughing, tracheal irritation and crusting around the stoma. Remove the device if the patient needs oxygen therapy via the tracheostomy mask.
Buchanan Bib: This is an airway device designed to provide filtration and allows adequate heat and moisture to the airway. Naturally, the ‘Bib’ needs to be removed when oxygen therapy using the tracheostomy mask is required.
Reduce risk of mucous plugging by: Use humidified oxygen or air Ensure temperature on humidifier chamber approximates 31˚C. Good positioning – sit patient upright ≥ 45˚C. Encourage deep breathing and coughing exercises. Chest physiotherapy as required. Suctioning down the stoma may be needed – exercise with caution in patients that have a speaking valve (inside airway) as suctioning could potentially dislodge the speaking valve. Some patients may not have a speaking valve in situ.
What not to do when administering oxygen: NEVER use face masks, nasal prongs, nasal oxygen catheters. NEVER administer nebuliser NO!! treatments via facemask or mouthpiece.
What to do when administering oxygen: This is the correct way to administer oxygen therapy using a tracheostomy mask – connect the heated tubing from the humidifier to the white connection at the front. Apply the tracheostomy mask directly over the stoma. YES!
Reduce risk of mucous plugging by: Use humidified oxygen or air Ensure temperature on humidifier chamber approximates 31˚C. Good positioning – sit patient upright ≥ 45˚C. Encourage deep breathing and coughing exercises. Chest physiotherapy as required. Suctioning down the stoma may be needed – exercise with caution in patients that have a speaking valve (inside airway) as suctioning could potentially dislodge the speaking valve. Some patients may not have a speaking valve in situ.
Stoma-gastric tube: A puncture is made (intra-operatively) through the back wall of the trachea and into the oesophagus. A feeding tube is then directed through this puncture. This is done in preparation for the fitting of a speaking valve. A patient would be discharged into the community with a stomagastric tube for 2 reasons: The patient has developed a fistula post-op requiring a lengthened period of nil by mouth and needs to continue with enteral feeds. 2. The patient is eating and drinking orally, but the stomagastric tube is maturing for fitting of their speaking valve. 1.
Communication: Patients have the larynx (voicebox) removed – communication methods will vary between each patient but the following should be noted: All patients must have access to a call bell. It may be necessary to communicate using pen and paper. Some patients may have speaking valves – requires surgery – but speaking valves may not be suitable for every patient. Other patients may use an electronic device that is held against the neck and this helps transmit sound through the tissues.
Medical alerts Patients may have difficulty communicating during a ‘minor emergency’. Some patients may wear medical identification bracelets similar to those shown below. Specially designed necklaces, medallions – or an alert card in the patient’s wallet – may also contain important information on medical conditions, allergies, medication and emergency contacts.
Emergency airway support: Never apply the mask to the patient’s face
Emergency airway support: In the event of a respiratory or cardiac arrest, artificial respiration can only be carried out via the stoma. YES! Preferably a small round size 1 mask should be used as it offers a better seal around the stoma
Emergency airway support:
Emergency events: intubation Intubation may be required an endotracheal tube may need to be inserted directly via the stoma. T The patient must NOT be intubated via the mouth or the nose.
Nursing and medical alerts: 1. Head of Bed Signs 2. Highlight in Safety Brief 3. Inform ICU of admission 4. Use laryngectomy checklist 5. Use obs chart stickers 6. Documentation inside the Tracheostomy Care Manual
Observation Chart Sticker: LARYNGECTOMY: not for oral or nasal intubation Follow the laryngectomy guidelines when breathing difficulties develop. Bag-valve-mask to stoma (or tracheostomy tube
Laryngectomy checklist: • • Use the checklist and observe the patient at least every 4 hours. Hourly observation is required whilst the patient is sleeping or in the patient with reduced level of consciousness. Never allow water/humidifier tubing condensate to enter the stoma. Regularly empty condensate from the hose tubing. Check that the weight of water in the tubing doesn’t pull on the tracheostomy mask. The humidifier chamber needs to be securely mounted on a drip-stand. Don’t allow the water chamber to run dry – check the water bag level every 4 hours. Precautions must be taken in the shower to prevent water from entering the stoma.
Patient’s requiring advanced respiratory support: e. g. non-invasive ventilation - will require management in ICU.