Laryngeal mask airway Dr S Parthasarathy MD DA
, Dip.")


















 is made of polyvinyl")
 LMA • The reinforced (or flexible) LMA (sizes 2 -5)")

 Aspiration is the danger? Can we decrease leak ?")


 The PLMA may not be inserted sufficiently far, with")




- Slides: 34
Laryngeal mask airway Dr. S. Parthasarathy MD. , DA. , DNB, MD (Acu), Dip. Diab. DCA, Dip. Software statistics. Ph. D ( physiology), ( IDRA )
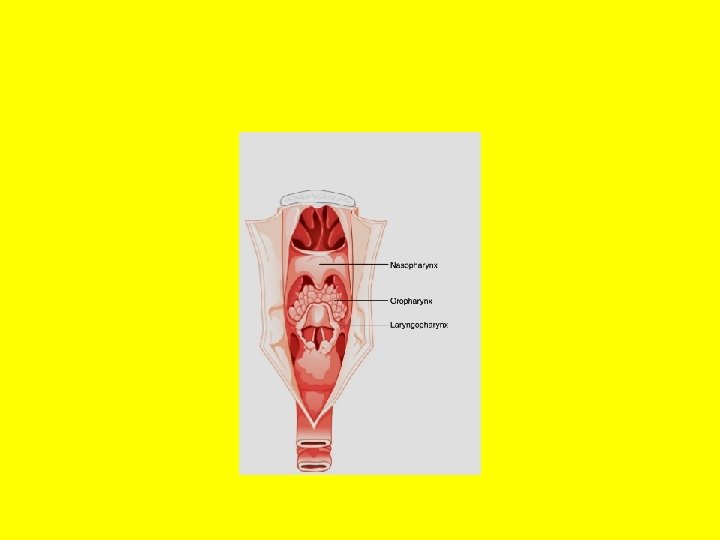
Supraglottic device – the first • standard fixtures in airway management, filling a niche between the face mask and the tracheal tube in terms of both anatomical position and degree of invasiveness. • These devices sit outside the trachea but provide a hands-free means of achieving a gas-tight airway.
History Archie Brain – Supraglottic approach was less traumatic Gold man mask in his dental anesthesia clinic Nasal mask was possibly similar to laryngeal inlet • Connected the tube with the rim • Prototype LMA in 1981 • •
From the internet for closed academic purpose only
1983 – first published article in BJA 1985 Katz MD popularized the use in US Slowly commercial devices Replaced ETT in the use as such in number of cases • Various modifications !! • •
LMA – classic • It consists of an oval soft silicone mask that sits over the larynx with an integrated stem that extends through the oral cavity to allow attachment to the anaesthetic circuit or other appropriate equipment. • Mask when inflated, fits around the laryngeal inlet and supports it in a position away from the posterior pharyngeal wall
• Mask like a bowl continues as a stem to end in a 15 mm male connector for a breathing circuit • Mask and stem – 30 degrees • Inflatable mask – tube, pilot balloon , valve • Grilles across the mask for preventing down folding of epiglottis. • Silicone rubber – 40 times autoclavable
Taken from internet for closed academic purpose only
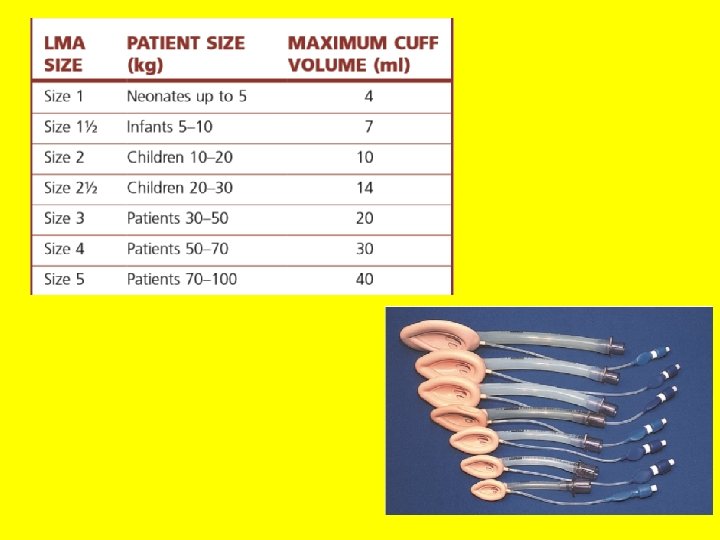
INSERTION TECHNIQUE Something like swallowing Deflate smooth, Fbs, pilot balloon Sniffing position Jaw assistant pen hold – index at junction Black line centre of upper lip push for hard palate Release pull assistant cuff tip flat against palate --See folding of tip. • •
• Continue pushing with left hand • Resistance • Anterior laryngeal displacement • Inflate to desired ml to see LMA slightly coming out
• When properly placed, the mask rests on the hypopharyngeal floor. The sides face the pyriform fossae, and the upper border of the cuff is behind the tongue base • Other techniques • Partially inflated • Retromolar and turn • Lateral in high arched palate • Release cricoid pressure if not
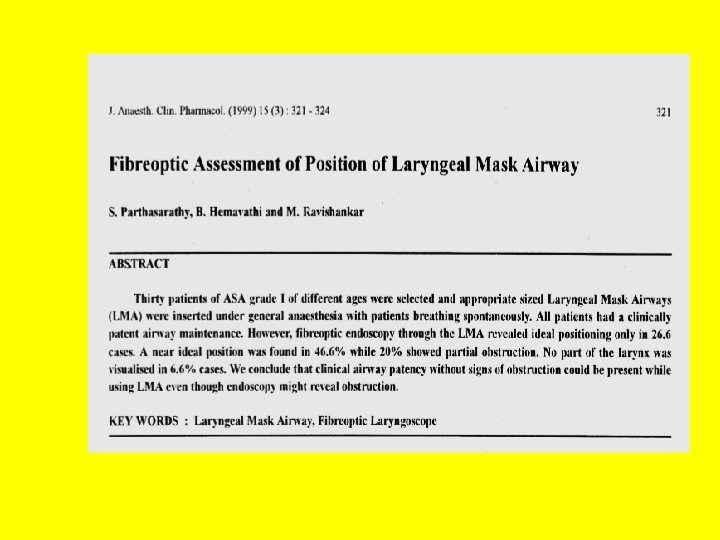
Seals !! • pharyngeal seal. • During controlled ventilation efficacy is dependent on factors such as whether the device orifice sits over the larynx and the quality of the device seal with the laryngopharynx • esophageal seal • Reducing aspiration risk requires a good-quality seal with the hypopharynx and/or oesophagus
• If the epiglottis has downfolded, moving the LMA up and down without deflating the cuff may help to reposition the epiglottis. Another maneuver is to withdraw for 5 cm and reinsert • My fixing – gauze piece and a plaster as bite block • Intubate through LMA if needed • Maintain anesthesia
Extubate LMA – my option • Supraglottic device – hence patient acceptance is better • Small dose fentanyl , cut off agents , awake • Reverse and totally awake • Deflate – remove the LMA – ask the patient to swallow • No suction in LMA removal
• Although careful placement, cuff inflation, and adaptation time improve the seal, leakage often occurs at 20 cm H 2 O airway pressure with the classic LMA. • Obesity, a head-down tilt, abdominal insufflation, airway obstruction, or any other conditions necessitating ventilation with high airway pressures increase the risk of hypoventilation, gastric insufflation, and regurgitation
Taken from internet for closed academic purpose only
Advantage LMA !! • • • Professional singers Remote locations Resuscitation Endoscopies ESWL
Complications • injuries have been reported with LMA use, including injuries to the epiglottis, posterior pharyngeal wall, uvula, soft palate, tongue, and tonsils • Sore throat • Ventilate ? Change of head position ? • rare complications include 12 th cranial nerve paralysis, unilateral hypoglossal nerve paralysis and transient bilateral vocal cord paralysis
• If gastric contents are seen in the laryngeal mask, the patient should be placed in the 30° head-down position, the LMA left in situ, anesthesia deepened, • and the breathing system disconnected temporarily to allow drainage and suctioning of the airway tube. • Intubate if aspirated
LMA-Unique • The single-use LMA-Unique (disposable laryngeal mask airway, DLMA) is made of polyvinyl chloride and costs less than a reusable LMA • tube is stiffer and the cuff is less compliant. • It may be helpful to warm the tube before insertion
The reinforced (or flexible) LMA • The reinforced (or flexible) LMA (sizes 2 -5) is an alternative version of the LMA in which the tube is thinner, narrower and longer and is reinforced with a spiral of steel wire to add flexibility and reduce the risk of kinking; • Difficult to insert. can rotate later • Tongue bite safety , no in MRI • But nasal surgeries , tonsils !!
Insertion of an LMA is frequently difficult in patients in whom tracheal intubation is difficult.
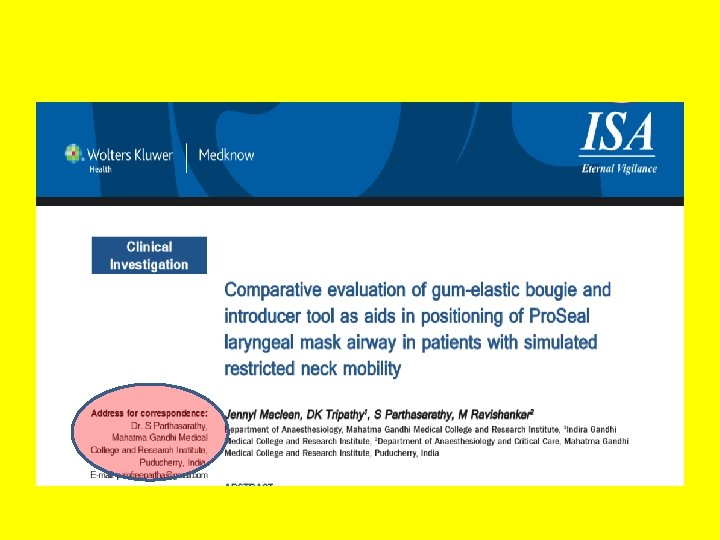
Proseal LMA ( p. LMA) Aspiration is the danger? Can we decrease leak ?
• Drainage tube with a ring • No grille • Cuff s- 2 • Anterior and posterior • Reinforced tube • - Hence narrower • Bite block
p. LMA • Greater depth • Technically more demanding insertion • The device may be introduced digitally or with a special introducer. • Bougie to drainage tube and esophagus • Bougie to larynx – straight to main tube • Laryngoscope or a tongue depressor
Position ? ? • (1) The PLMA may not be inserted sufficiently far, with the consequence that the tip of the drainage tube lies in the pharynx. Positive-pressure ventilation is ineffective because delivered gas passes out the drainage tube. • (2) The tip of the PLMA may lie within the glottis, thereby obstructing ventilation and impairing function of the drainage tube. • (3) The tip may be folded over and obstruct ventilation and the drainage tube.
Gel to proximal portion of drainage tube • The drainage tube gel does not move with positive-pressure ventilation or brief firm pressure applied to the sternum. • The drainage tube gel does not move when airway pressure is raised to 20 cm H 2 O. • The drainage tube gel moves slightly when brief “bobbing” pressure is applied to the suprasternal notch (the mechanism is pressure on the esophagus). ( SS notch test ) • Catheter inside drain tube
Clinical pearls Can we nebulize ? ? Pregnancy more than 14 weeks ? ? Prone position ? ? Classic 20 cm Vs 30 cm peak pressure for p. LMA • Cuff pressure is 60 cm for both • Limit of surgical duration – 2 hours but with proseal 12 hours reported • •
Supreme LMA • . Similar to the p. LMA, • s. LMA has an improved cuff design that produces higher airway leak pressures, • drainage tube that allows for gastric access, • integrated bite block • Fixation tab to insert and to find size
Summary • • LMA – history Types Classical insertion tecniques Indications and contraindications Merits and demerits Supreme p. LMA Other SGD in next classes Thank you all