Laparoscopic Surgical Management of Epithelial Ovarian Cancer Cagatay

































- Slides: 45
Laparoscopic Surgical Management of Epithelial Ovarian Cancer Cagatay Taskiran, MD, Assoc. Prof. VKV American Hospital, Division of Gynecologic Oncology
L/S & EOC q Primary trt for early stage disease q Restaging q Primary cytored’n for advanced disease q Surgical trt for recurrent disease q To assess resectability: Neoadjuvant CT q VATS
Early Stage is Rare
Standard Surgery for Early Stage Ovarian Cancer q Comprehensive surgical staging Exploration - Cytology and biopsies Hyst-BSO- fertility sparing surgery PPLNDTotal Omentectomy Appendectomy
Up-staging Schuler et al, 1999, EJOGRB 401 patients, 24% up-staging q. Diaphragma q. Omentum q. PPALN q. Cytology
Distribution of LN Metastasis
Literature Early stage ovarian cancer & Laparoscopy q. Retrospective series q. Case-control studies q. Meta-analysis q. Cochrane review
Literature Early stage ovarian cancer & Laparoscopy 1994, Querleu-Leblanc 9 patients q. Still small series, number low q 11 studies, 9 -42 pt, 88 multicenter q. Approximately 400 patients
Comparative Studies & Feasibility Chi, AJOG, 2005, 50 pt LN number, omental size: no problem No conversion to L/T Survival rates similar Park, Ann Surg Oncol, 2008, 36 pt LN number, omental size: no problem Upstaging rate is same No recurrence within 20 months
Comparative Studies & Feasibility
Whole Literature
Benefits of Laparoscopy Endometrial cancer – randomized studies EBL lower Shorter hospital stay Fewer postoperative complications Improved QOL Faster return to normal function Similar for ovarian cancer – no RCT, shorter interval to adjuvant chemotherapy
Benefits of Laparoscopy Ghezzi, 2 012, 88 pt Blood tx rate 2. 8% vs 19. 2% Postoperative complications 3. 2% vs 31% Febrile morbidity Ileus Wound dehiscence Wound infection
Potential Benefits & Some Conflicts Cost Complications Hospital stay Performance – return to work – CT ? ? Improved fecundity after fertility sparing surgery - adhesions
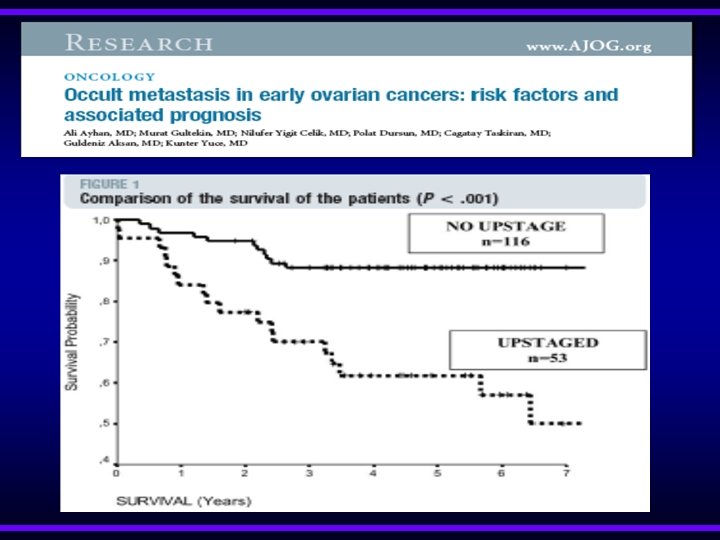
Possible Risks & Rupture – IC – Chemo – survival is worsened v. L/T 10% and L/S 15 -20% v. Size and endobag usage v. Rupture vs puncture ? ?
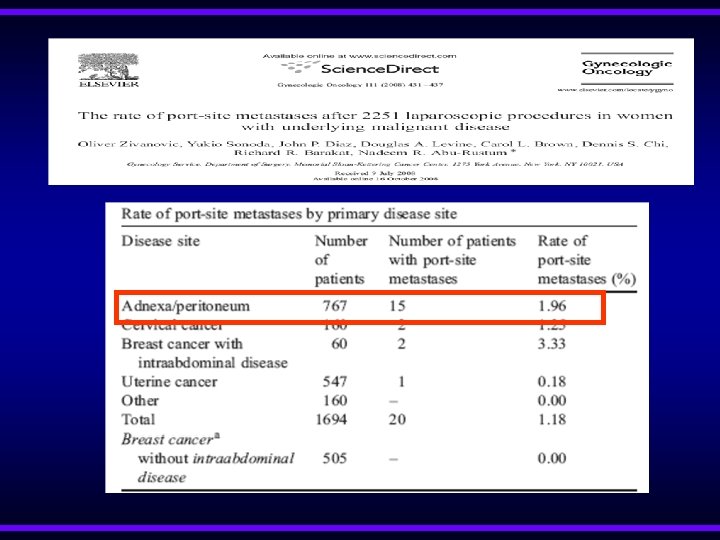
Meta-Analysis & Accepted 4 April AJOG 11 studies EBL lower Upstaging rate Conversion to L/T Recurrence rate Intraop rupture 23% 3. 7% 9. 9% (6. 7 -14) 25% !!!!! Only 1 port site-metastasis
Data Overall 12 hasta Borderline EOC LN number Omentectomy 8 pt 4 pt (all restaging) 31 -84 no problem No conversion No intra-postop comp Median time 5 hr
Trocar Sites
Transperitoneal LA & Learning curve q >20 cases PLN number satisfactory, time shorter, complications decrease; LN number: 17 -22 q Paraaortic LN number increase by years: 6 ----19 Kohler, GO, 2004
Transperitoneal LA & Duration Kohler, GO, 2004
Re-staging & Up-staging 14 studies 1971 -1994
Timing of Restaging Lehner 1998 Kinderman 1996 max. 15 days max. 8 days Adequate staging is very important
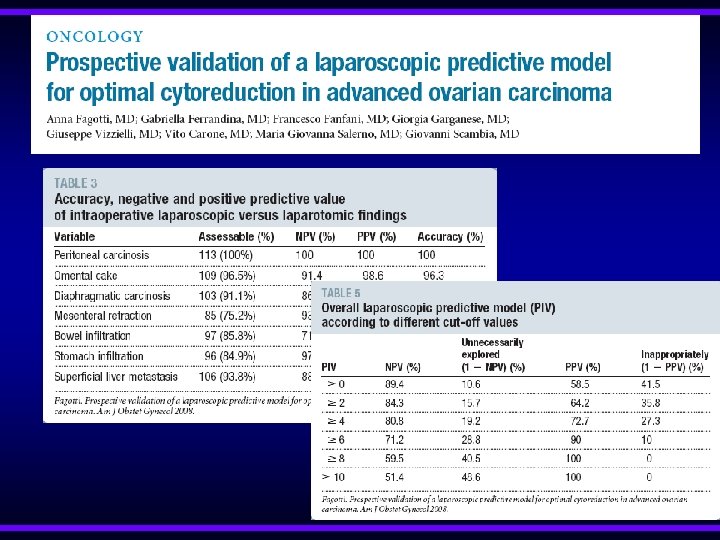
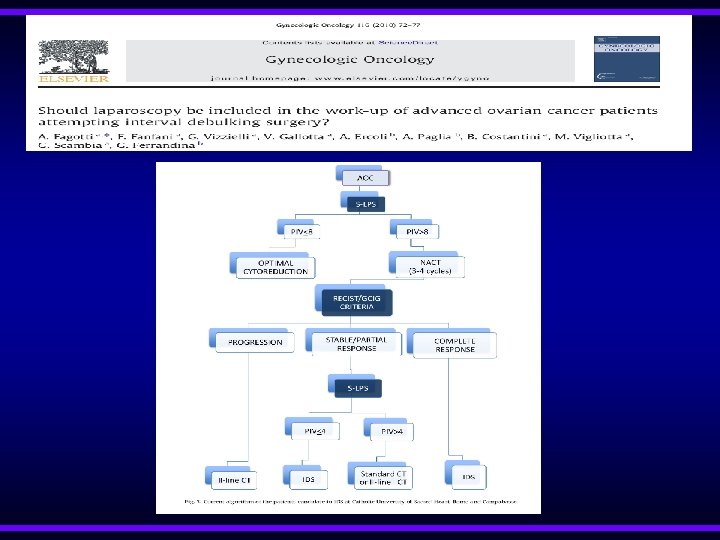
Primary Debulking for Advanced Disease Fanning, 2011, GO q CT: omental metastasis – ascites q 25 cases – 2 conversions: severe omental-RS q 36% no residual q Hospiatal stay median 1 day q Blood loss 340 ml q Median OS: 3. 5 years
Primary Debulking for Advanced Disease Nezhat, JSLS, 2010 q 28 pt, 11 open after diagnostic L/S q %88 optimal q Time and complication rates are same q Blood loss and hospital stay less q 9 NED, 6 AWD, 2 DOD
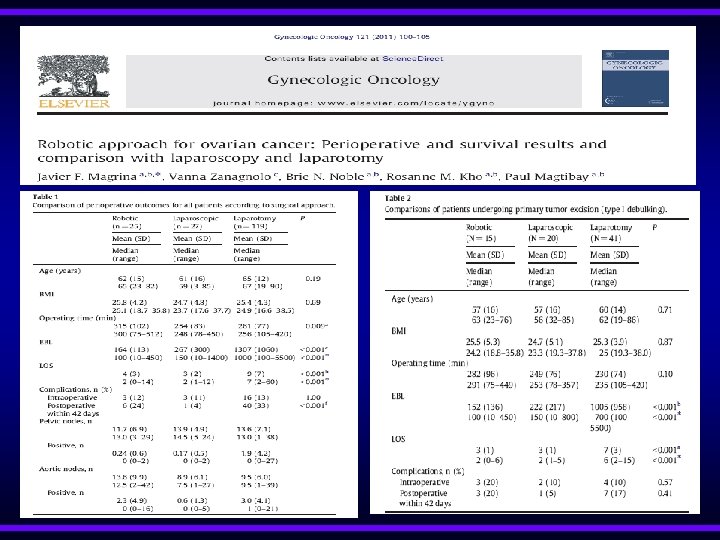
Secondary Cytoreduction Magrina, 2013, GO, 2006 -2010 q L/S: 9, Robot: 10, L/T: 33 patients q 15 types of different procedures q No conversion q No difference: Op. Time, comp’n, complete debulking, survival q Endoscopy: Blood loss and hospital stay q L/T: 3 major procedures, upper and lower quadrants
Secondary Cytoreduction Nezhat, JSLS, 2012, only L/S q 1999 -2009, secondary 20, tertiary 3 cases q %82 optimal q 200 min, 75 ml, stay 2 days q 1 conversion q No intraop complication q NED: 12 q AWD: 6 q DOD: 4 q Median DFS: 72 months
Conclusion q There is limited data on the role laprascopic surgery for early stage ovarian cancer q Although it was started at nearly the same time periods with EC and CC it was not populirezed q It seems feasible for surgical procedures, upstaging rates, adequacy of lymphadenectomy and omentectomy q Survival rates are similar with laparotomy q Port site metastasis is rare, Major problem is tumor rupture
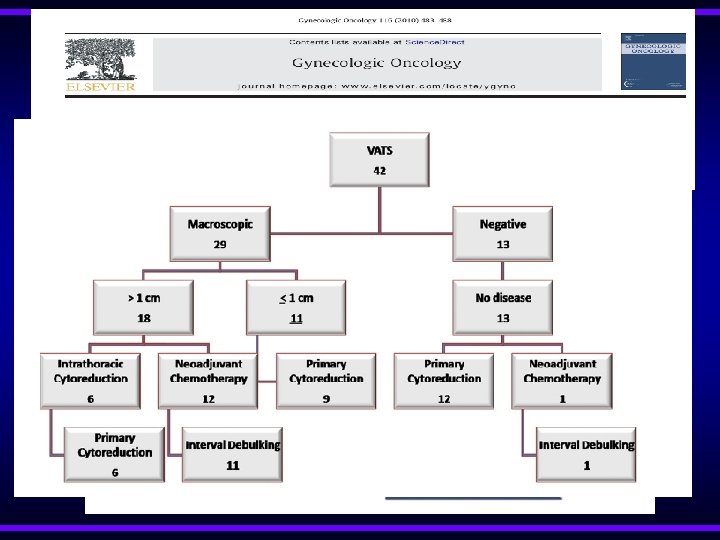
Conclusion q There is limited data on the value of laparoscopic surgery for recurrent disease. It seems feasible for highly selected patients at very experienced centers q It may be good way to assess resectability for advanced cases both before primary surgery and after NACT q VATS should be performed for patients having moderate to severe pleural effusion beforre abdominal cytoreduction
Thanks for your attention ….