Laparoscopic Cholecystectomy How to make it safe By

Laparoscopic Cholecystectomy, How to make it safe? By Prof. Dr. Ahmed Lotfy Ain Shams University
")
Liver Common hepatic duct Gallbladder Cystic duct Common bile duct (CBD)

PORTS ARRANGEMENT
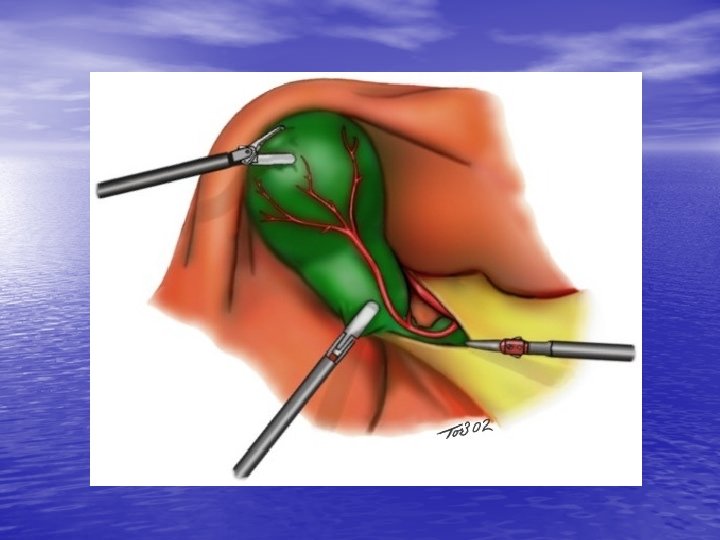

CALLOT’S TRIANGLE
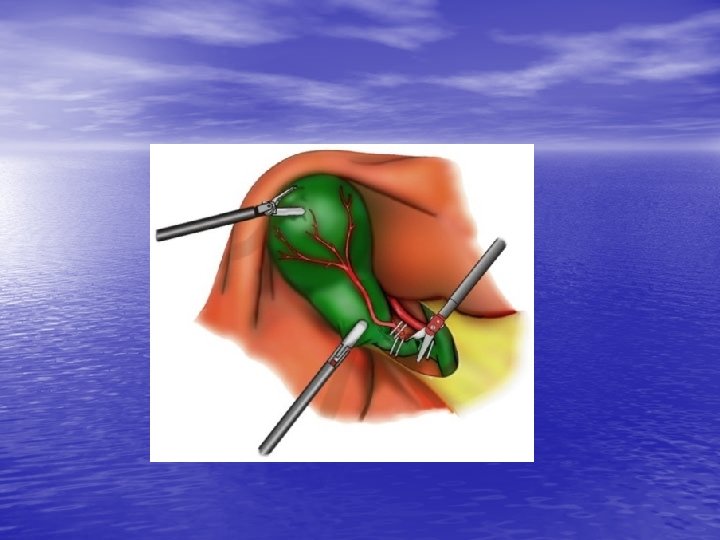

LAP. CHOLECYSTECTOMY TECHNIQUES

Difficult Laparoscopic cholecystectomy

Many difficulties may be encountered: ØPatients with compromised cardiac and § § § respiratory functions: Avoid head down position during surgery; Reduce the pre-selected intra-abdominal pressure to 10 mm. Hg “maximum” Infiltrate the port sites by local anesthesia “marcaine” before puncture.

Many difficulties may be encountered: ØDifficult pneumoperitoneum Ø In very obese patients the umbilical cicatrix may be used for entry (least amount of abd. Fat); Ø In scarred abdomen open or semi open laparoscopy (by using an artery and the finger instead of Veress needle).

Many difficulties may be encountered: ØLaparoscopic cholecystectomy for acute cholecystitis : o. Laparoscopic cholecystectomy in acute cases is not for beginners; o. Aspirate the gall bladder if possible; o. If the fundus is too thick and edematous to be grasped → a toothed gasper is used to support the fundus and retraction of the liver up or just elevaion of gall bladder o. Fundus 1 st. approach

Many difficulties may be encountered: ØLaparoscopic cirrhotic cholecystectomy in o. It is difficult to retract the liver up; o. If the Hartman area could not be seen: You may start some dissection from the fundus or lateral aspect to be able to slide the gall bladder up to visualize the fundus; o. Meticulous haemostasis; o+ drain.

Many difficulties may be encountered: ØDifficult extraction If thick wall “acute cholecystitis” or big stone, it is better to extract the gall bladder from the umbilical port after transferring the scope to the epigastric port, widening the umbilical incision which will be closed later by interrupted sutures.

Many difficulties may be encountered: ØWide cystic duct You may use 11 mm clips if available or use 9 mm at first which will not close the whole lumen followed by applying premade endoloop knot. ØAdhesions o. Stick to the gall bladder; o. Minimize using monopolar diathermy as much as you can or meticulous use of hook

Many difficulties may be encountered: ØBig stone in Hartman’s pouch q. Try to move the stone up and grasp the Hartman below it. q. Lat grasper for retracting the liver without holding the fundus. The other 2 graspers manipulate the stone up. q. If failed, try to support the Hartman by a grasper and dissect the calot triangle.

Many difficulties may be encountered: Ø Left lobe encroaching on the operative field o. Raise the right shoulder of the patient; o. Use a long port or converter from the epigastric incision; o. Use angled scope or change position of camera. o. Finally you may put additional port to retract the left lobe.

Many difficulties may be encountered: ØWhen to stop If after sometime of actual work →no progress → please open. Remember: opening a case is not a failure but indicates maturity in decision making.

COMPLICATIONS ANOMALIES

ACUTE CHOLECYSTITIS

SHORT CYSTIC WIDE CYSTIC

UNCLEAR ANATOMY ADHESIONS SMOKE BLOOD BAD FIELD

INEXPERIENCE, BAD TECHNIQUE

ELECTROCAUTERY

CLIP PROBLEMS • FAILURE • COUPLING • MIGRATION

CBD EXPLORATION

Thank You
- Slides: 26