Lactation MCB 135 E Lecture 22 Nutrition of

Lactation MCB 135 E Lecture 22

Nutrition of the Infant Survival & growth depends on: • the mother’s ability to breastfeed • the baby’s ability to suck • good development/function of the gastrointestinal system • good development/function of the central nervous system (which regulates & coordinates GI functions)

Background • Breastfeeding was once a universal requirement for infant survival and still is for many world areas • 1920 s until after WWII: breastfeeding rates declined in industrialized countries • 1970 s: <25% of all infants breastfed at birth; 5% at 6 months

Background • Since 1970 there has been a reversal in this downward trend • Currently breastfeeding rates vary widely with the ethnicity & education level – 60% Caucasian women breastfeed v. 30% African. American women – 70% of women with over 13 years of education breastfeed v. 30% of those who did not complete high school

Growth of Mammary Glands Embryology • 6 th week of gestation: Mammary glands begin to develop as solid growths of epidermis called mammary ridges • Under the influence of estrogen (E) from placenta, mammary ridges canalize to form ducts • At birth, mammary glands of males and females are identical, composed of ~15 -20 rudimentary lactiferous ducts

Development of Breasts: Puberty Female breasts develop further after puberty (under influence of E from developing follicle & corpus luteum each month) • Enlargement occurs due to deposition of fat & connective tissue • Nipple becomes enlarged and pigmented • Further growth & branching of lactiferous ducts

Development of Breasts: Pregnancy • More intense growth and branching of lactiferous ducts (under high levels of E from corpus luteum & placenta) • GH, glucocorticoids, prolactin (PRL), insulin all influence growth • Final development of mammary glands occurs under the influence of progesterone (P), which (in concert with hormones mentioned above) cause alveoli to bud from the ends of the lactiferous ducts • Each alveolus is lined by milk secreting cells
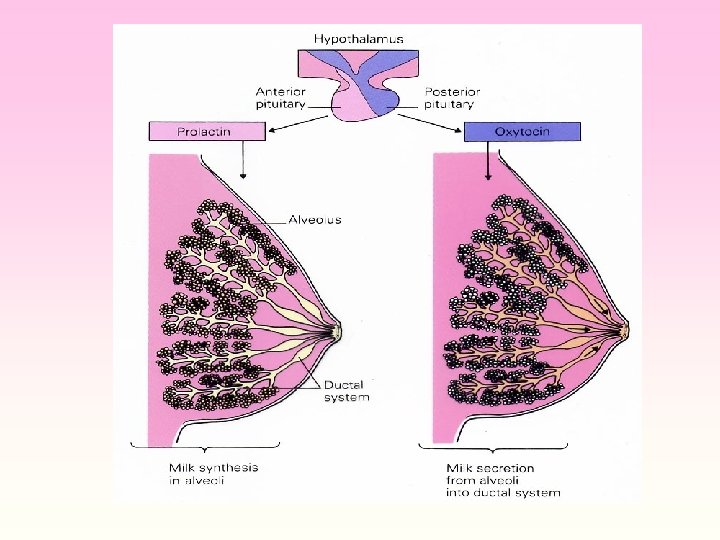
 • PRL, secreted by anterior pituitary gland, stimulates milk production")
Milk Production (during pregnancy) • PRL, secreted by anterior pituitary gland, stimulates milk production • During pregnancy, PRL levels increase 20 fold but action of PRL inhibited by high E & P levels • Human chorionic somatomammotropin ( i. e. placental lactogen) plays role in lactogenesis • Towards end of pregnancy, breasts are fully developed but milk production is suppressed except for small amount of colostrum (same concentration of proteins and lactose as regular milk but hardly any fat)
 • After birth, E and P levels drop and milk")
Milk Production (after birth) • After birth, E and P levels drop and milk is produced in 1 -7 days • Milk production requires: secretion of hormones involved in protein, glucose & calcium regulation (GH, cortisol, insulin, PTH) • PRL levels return to normal within a few weeks. Each time an infant feeds, neurohumoral reflex leads to burst of PRL secretion

Milk Ejection • Alveolar milk accumulate in the lactiferous sinuses (enlargements of ducts near opening of nipple) • Suckling hypothalamus release of oxytocin from post. pituitary. Oxytocin contraction of myoepithelial cells around the ducts. • Negative maternal emotions (frustration, anger, anxiety) can inhibit oxytocin secretion & suppress milk ejection reflex

Cessation of Lactation • After mother stops breastfeeding & PRL levels decline, alveoli degenerate and reabsorb. Duct structure remains until menopause • PRL inhibits pulsatile secretion of Gn. RH by the hypothalamus, resulting in amenorrhea during lactation • This is an unreliable method of contraception used by many women

Benefits of Breastfeeding Compared to Formula-fed Babies Incidence and severity of infections Growth until one year of age Incidence of obesity in adulthood Improves mental development

Benefits of Breastfeeding: Mother Metabolic demands Weight loss after deliver Psychological benefits for mother, child & father Amenorrhea during lactation may act as contraceptive and, possibly, decreased risk of breast cancer

Complications of Breastfeeding • In the past, health professionals recommended breastfeeding only under ideal circumstances. They recommended formula feeding with maternal illness, stress, or inadequate milk production. • Today, mothers receive much greater encouragement to start and continue breastfeeding at least through the first six months, even in the face of complications.

Complications of Breastfeeding HIV: Risk of transmission of infection at birth breastfeeding. Drugs secreted in the milk may impair growth And development Hep B + mothers: Infant must receive globulin Nutritional supplements required for premature infants

Immunology • • Infant immune system is immature at birth. In utero, transfer of antibodies across placenta. This protection tapers off quickly after birth. Breast milk contains a number of different agents to protect the infant: – Secretory Ig. A – WBCs: neutrophils and macrophages – Growth factors: EGF, NFG, IFG
- Slides: 17