Laboratory Methods Dr ali pahlevani PREPARATION OF SPECIMENS

Laboratory Methods Dr ali pahlevani

PREPARATION OF SPECIMENS 1 - Fixation 2 - Grossing 3 - Demonstration of Enzyme Activities 4 - Processing 5 - Staining

Fixation ü It is important to properly fix a skin biopsy to stabilize proteins and prevent tissue decay and then prevent artifacts. ü The fixative of choice is a 10% neutral-buffered formalin solution. ü The volume of formalin should be 10 to 20 times the volume of the specimen. ü During winter, either 95% ethyl alcohol, 10% by volume. ü Fixation time is 1 to 2 hours per millimeter thickness

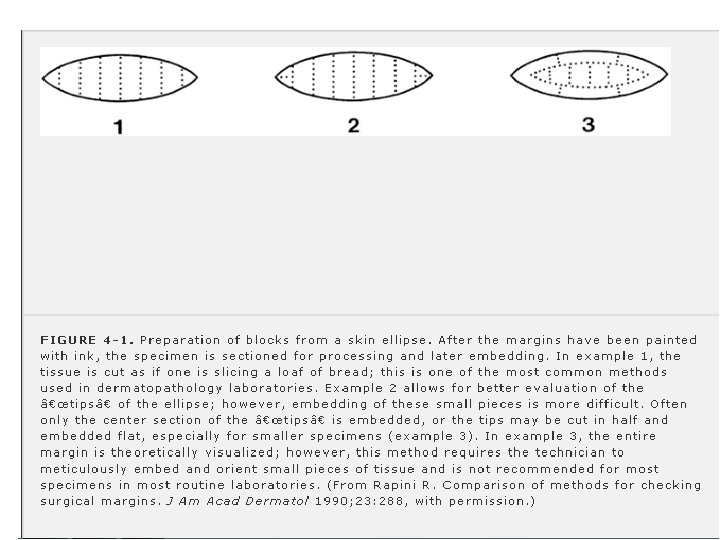
Grossing After fixation due to evaluate cutting margins we should apply ink to specimen. For every size there are techniques for making margin by cutting the specimen.

Demonstration of Enzyme Activities There are few exceptions, specimens should not be placed in formalin such as enzyme activities staining in scleredema of Buschke and amyloidosis. Instead of formalin fixation, specimen delivered to the laboratory wrapped in water-moistened gauze and placed in a clean container, because frozen sections cut on a cryostat are typically used for enzyme staining. For example: 1. demonstration of dopa-oxidase activity in melanocytes could potentially aid in distinguishing a malignant melanoma from tumors not composed of melanocytes

2. In scleredema, demonstration of hyaluronic acid with toluidine blue at p. H 7. 0 may be more intense in unfixed, frozen sections than in formalin-fixed sections. 3. In amyloidosis, the reactions of the amyloid with crystal violet or Congo red may be conclusive only in unfixed, frozen sections.

Processing The purpose of processing is to remove the extractable water from the skin and to provide a supporting matrix (paraffin) so that the tissue can be cut with minimal distortion. After fixation, routine specimens are processed in an automatic processor except lipids because xylene that we used for processing extract lipids.
 passing through high concentration of ethanol for dehydration b) xylene for lipid")
Processing: a) passing through high concentration of ethanol for dehydration b) xylene for lipid extraction and clearing of alcohol c) several changes of hot, melted paraffin for stabilizing of specimen and facilitate cutting

Processing may take long 4 -12 hours. The new method for acceleration of fixation and processing is microwave irradiation to 2 hours. The next morning, specimen are embedded in liquid paraffin with the cut surface for hardening. The cut surface must embedded hardly in the cassette base mold for preserving sections orientation. The specimens are then cut on a rotary microtome into sections 5 to 7µm thick.

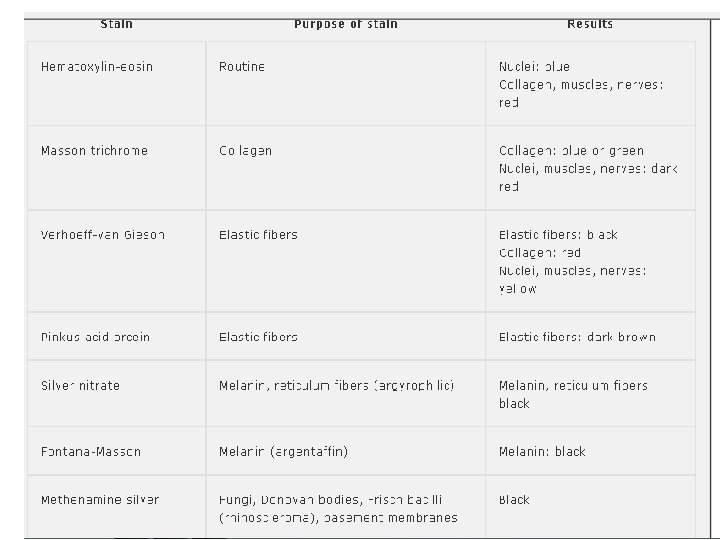
Staining Routine sections are usually stained with hematoxylin-eosin, the most widely used routine stain. With this staining method, nuclei stain blue or basophilic , and collagen, muscles, and nerves stain red or eosinophilic. Special stains are employed when particular structures need to be demonstrated

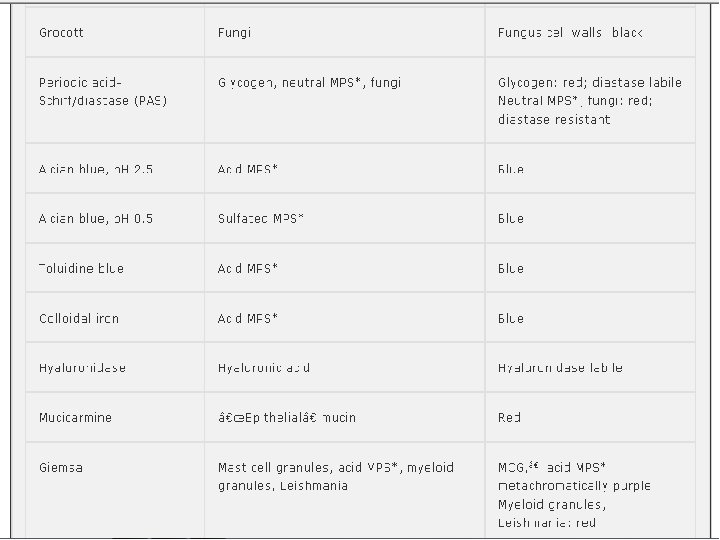
HISTOCHEMICAL STAINING Most histochemical stains can be carried out on formalin-fixed, paraffin-embedded material. PAS: 1. The periodic acid-Schiff (PAS) stain demonstrates the presence of certain polysaccharides, particularly glycogen and mucoproteins containing neutral mucopolysaccharides, by staining them red. 2. The PAS reaction valueable also in the study of basement membrane thickening, such as in lupus erythematosus or porphyria cutanea tarda

3. the cell walls of fungi are composed of a mixture of cellulose and chitin and thus contain polysaccharides, fungi stain bright pink-red with the PAS reaction. For distinction of fungi and glycogen deposits , specimens are exposed to diastase before staining then because glycogen is digested by the diastase, and thus no longer colored by the PAS reaction.

Because glycogen is present in outer root sheath cells and eccrine gland cells, demonstration of glycogen may be of diagnostic value in adnexal tumors with outer root sheath or eccrine differentiation. 4. Demonstration of neutral mucopolysaccharides is of value in Paget's disease of the breast and in extramammary Paget's disease

ALCIANE BLUE: The Alcian blue reaction demonstrates the presence of acid mucopolysaccharides by staining them blue. a) acid mucopolysaccharides: in small amounts in normal skin dermal ground substance. However in dermal mucinoses there are nonsulfated acid mucopolysaccharides, mainly hyaluronic acid, so that the mucin stains with Alcian blue.
 Sialomucin: Sialomucin contains nonsulfated acid mucopolysaccharides staining with Alcian blue at p. H")
b) Sialomucin: Sialomucin contains nonsulfated acid mucopolysaccharides staining with Alcian blue at p. H 2. 5 but not in PH 0. 5; In extramammary Paget's disease of the anus with rectal carcinoma in cutaneous metastases of carcinoma of the gastrointestinal tract containing goblet cells , tumor cells in the skin, like their parent cells, secrete sialomucin.
 strongly acidic sulfated-acid mucopolysaccharides: They stain with alcian blue both at p. H")
c) strongly acidic sulfated-acid mucopolysaccharides: They stain with alcian blue both at p. H 2. 5 and at p. H 0. 5. they are present in: heparin in mast cell granules and chondroitin sulfate in cartilage.

Elastic tissue: The most commonly used stains are the Verhoeff-van Gieson or Weigert resorcin-fuchsin Additional techniques, such as the Luna stain and Miller stain, may allow better visualization of elastic fibers than traditional methods. These stains are beneficial in the diagnosis of: anetoderma, connective tissue nevi, mid-dermal elastolysis, other alterations of elastic tissue.

Geimsa The Geimsa stain is frequently utilized to highlight mast cells. Geimsa contains methylene blue, a metachromatic stain. The granules of a mast cell will stain metachromatically purple


Polarisocopy Dr Abdulrahman Azizpour Dermatology resident Polariscopic examination is the examination of histologic sections under the microscope with polarized light. ,

• • • Polariscopic examination is useful in evaluating: lipid deposits certain foreign bodies , gout, amyloid.

Certain lipids are doubly refractile. Cholesterol esters are doubly refractile but free cholesterol , phospholipids and natural fat are not. • Only formalin-fixed, frozen • Sections can be used for a polariscopic examination for lipids.

• • • Doubly refractile lipids are present in : Tuberous and plane exanthemas Xanthelasmata of hyperlipidemia, Diffuse normolipidimic plane exanthema Walls of angiokeratoma corporis diffusum Histocytomatosis. X Juvenile xanthogranuloma, Erythema elevatum dutinum Dermatofibroma

Doubly refractile lipids are absent in : Necrobiosis lipoidica, Lipoid proteinosis Multicentric reticulohystosis Solitary rticulohistocytosis granuloma

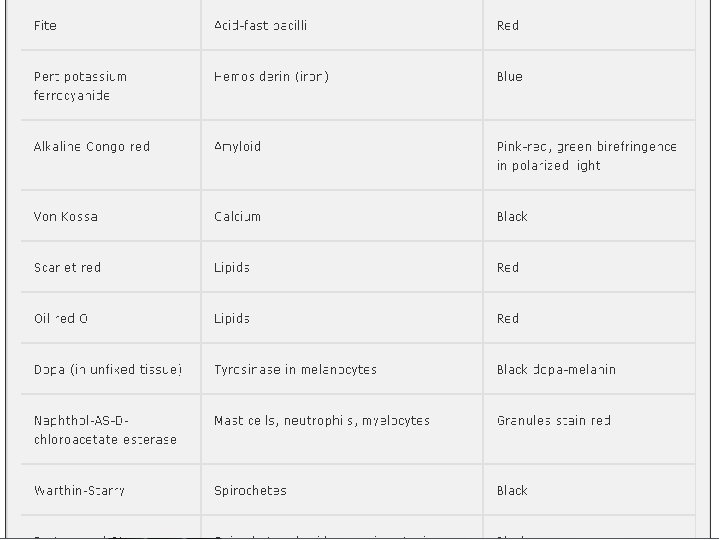
• Among the foreign bodies are : • Silica , Talcum powder , wooden splinters and suture materials • Gout taphi shows double refraction of the. ureate crystal preserved in alcohol • Amyloid shows a characteristic green birefringence in polarized light after Congo red staining.

Direct Immunofluorescence Interpretation

Autoimmune Blistering Diseases • Sensitivity of direct immunofluorescence with active autoimmune blistering disease should be close to 100% • In pemphigus vulgaris and pemphigus foliaceus, the Ig. G immunostaining on the epithelial cell surfaces can be granular and/or linear, resulting in a characteristic chicken wire pattern.

• In paraneoplastic pemphigus, the Ig. G chicken wire immunostaining tends to be linear, thick, and homogenous throughout the epidermis and mucosal specimens including those from bronchi.

• The presence of low titers of circulating autoantibodies may preclude differentiation among the subepithelial autoimmune blistering disorders using indirect immunofluorescence.

• In this cases, a technique called salt-split direct immunofluorescence often circumvents this problem. • This technique consists of thawing the frozen specimen formerly used for routine direct immunofluorescence and incubating it in 1 molar (M) Na. Cl for 48 to 72 hours, allowing for separation of the epidermis from the dermis. • This salt will cleave the basement membrane zone through the lamina lucida, leaving the hemidesmosomes on the epidermal side • and • type VII collagen and epiligrin on the dermal side of the artificially induced blister.

• in all cases of bullous pemphigoid, the linear Ig. G immunostaining will be localized on the epidermal side (occasionally epidermal and dermal) • in epidermolysis bullosa acquisita on the dermal side.

Cutaneous Lupus Erythematosus • The intensity of the deposits of immunoreactants along the basement membrane in these patients correlates with the degree of interface/lichenoid dermatitis/ mucositis.

• In discoid lupus erythematosus, the most common immunoreactant visualized with direct immunofluorescence is Ig. M, • in systemic lupus erythematosus and in subacute cutaneous lupus erythematosus, Ig. G. • most patients with anti-Ro positive, subacute cutaneous-lupus erythematosus may have a characteristic granular Ig. G speckling pattern along the basement membrane and throughout the epidermis.

• The lupus band test, described as positive when granular Ig. G is present along the basement membrane zone in specimens from sun-protected nonlesional areas, has been rapidly abandoned due to its unreliability.

Cutaneous Vasculitides The best immunofluorescence diagnostic yield in Henoch- Schoenlein purpura is obtained from 1 - to 2 -day old lesions. As lesions get older, the Ig. A deposits get degraded and cleared. In Hypocomplementemic urticarial vasculitis , granular Ig. G and C 3 deposits are seen in and around small dermal vessels and along the basement membrane zone.

• Lichen planus lesions, mainly the mucosal variant, are characterized by typical, yet not pathognomonic, linear and shaggy fibrin deposits, and patchy granular Ig. M and C 3 along the basement membrane.

• The direct immunofluorescence findings in cutaneous porphyrias are indistinguishable from those seen in pseudoporphyria. • These findings are characterized by thick and glassy linear Ig. G and Ig. A deposits in superficial dermal vessels in a doughnut pattern and along the basement membrane. • It is thought that immunoglobulins get trapped and bound to glycoproteins in a thickened basement membrane zone and degenerated blood vessels in this disorder.

INDIRECT IMMUNOFLUORESCENCE • Indirect immunofluorescence is a semiquantitative procedure in which a double immunolabeling is carried out to evaluate the presence and titer of circulating antibodies, or to specifically localize antigen in the skin.

• Monkey esophagus is probably the best single substrate for the evaluation of antiepithelial surface antibodies specifically for pemphigus vulgaris and paraneoplastic pemphigus.

• In pemphigus vulgaris and foliaceus, antidesmoglein antibodies give a chicken wire staining, which is more predominant on superficial epithelial cells, • whereas in paraneoplastic pemphigus, the antiplakin antibodies give a pattern that is consistently homogeneous throughout the epithelium and even sometimes associated with immunostaining along the basement membrane zone.

• Transitional epithelium is a plakin-rich substrate, and thus murine bladder is a common substrate for the screening of circulating antiplakin antibodies in paraneoplastic pemphigus

• Monkey esophagus is also a useful substrate in the indirect immunofluorescence screening for subepidermal autoimmune blistering disease. • However, human salt-split skin renders better definition of the subtypes of subepidermal blistering disorders. • Disorders characterized by antibodies to hemidesmosomal proteins BP 180 and BP 230, including those seen in: • bullous and gestational pemphigoid, • some cases of mucous membrane pemphigoid, and linear Ig. A bullous disease, • are associated with a linear immunostaining on the epidermal side (roof) of the salt-split human skin.

• On the other hand, patients with circulating antibodies reacting against type VII collagen and antiepiligrin (laminin 5) as is seen in: • epidermolysis bullosa acquisita • antiepiligrin mucous membrane pemphigoid respectively, have circulating Ig. G autoantibodies that bind the dermal side of the salt-split human skin.

Indirect Immunofluorescence for Evaluating Cleavage Site in Hereditary Epidermolysis Bullosa • this technique classifies these disorders into epidermolytic, junctional, and dermolytic categories. • this technique is performed as follows: a fresh induced blister is obtained by twisting a rubber-ended pencil, and then this artificially induced blister skin specimen is incubated with anti-type IV collagen and anti-BP 180 antigen

• In some cases of generalized, atrophic, benign epidermolysis bullosa, where the mutated protein is the BP 180 Ag, the immunostaining in the floor of the induced blister given by the anti-BP 180 may be focal or absent.

• • • Specific antibodies to the mutated protein are also used for complementary diagnostic purposes. These antibodies include: “anti-plectin” antibodies for EB simplex with muscular dystrophy, “anti a 6 b 4” in junctional epidermolysis bullosa with pyloric atresia, “anti-laminin 5” antibodies for most cases of junctional epidermolysis bullosa, anti-type VII collagen for most cases of dystrophic form of hereditary epidermolysis bullosa. These specific antibodies are intended to identify a disrupted linear staining due to an even distribution of the probed mutated protein.

In the name of God

IMMUNOHISTOCHEMISTRY

Introduction They are mainly used to diagnose poorly differentiated malignant tumors and lymphoma. The origin of an undifferentiated cell can usually be determined with the application of monoclonal or polyclonal antibodies. A panel approach using multiple markers is the best method for evaluating problem neoplasms. Most monoclonal antibodies, especially those necessary for the diagnosis of lymphoma, have required frozen section studies, but monoclonal antibodies are presently being produced that can be applied to formalin-fixed, paraffin-embedded tissue, tissue such as antibodies for the identification of B cells, T cells, and macrophages.

Introduction Sections that will be incubated with polyclonal or monoclonal antibodies should be mounted on glass slides specially coated or charged to ensure better adherence. Many laboratories currently employ the Microprobe Slide Staining System, using slides with a positively charged surface. Certain antibodies, including antibodies against keratins, lysozyme, or chymotrypsin require protease digestion if formalin-fixed, paraffin-embedded sections are used. Other antigen retrieval methods include the use of heat, either by microwaving or steaming the sections, and pretreatment of the sections with acid (HCl).
 technique has")
Immunohistologic Techniques Historically, several techniques have been used; the peroxidase -antiperoxidase (PAP) technique has been replaced by more sensitive techniques, namely, the avidin-biotin-peroxidase complex (ABC), the alkaline phosphatase-anti-alkaline phosphatase (APAAP), and the streptavidin peroxidase or alkaline phosphatase techniques. In all of these methods, the antibody is used to localize an enzyme (peroxidase or phosphatase) to sites of antigen expression in tissue sections. An appropriate chromogen is then added. A chromogen is a reagent that has the property of developing a color that can be visualized at sites of localization of the enzyme-antibody-antigen complex.

Alkaline Phosphatase-Anti-Alkaline Phosphatase Technique This is an unlabeled antibody bridge technique that utilizes three antibodies; the first and third antibodies are from the same species and are monoclonal. The second antibody is polyclonal from the rabbit, and forms a bridge between the first and third antibody. The third antibody is linked to the enzyme alkaline phosphatase. After applying these antibodies with the linked enzyme, an alkaline phosphatase substrate is added containing a compatible indole chromogen such as INT/BCIP (which yields a red color after the phosphatase-catalyzed reaction), naphthol fast red (red color), or NBT/BCIP (blue). This method may be useful for pigmented tumors since the blue or red reagents can be distinguished easily from melanin.


Avidin-Biotin-Peroxidase Complex and Streptavidin Peroxidase or Alkaline Phosphatase Techniques Avidin is a glycoprotein found in egg white that has a strong affinity to biotin, a vitamin of low molecular weight. The streptavidin technique is exactly analogous, but achieves one to two orders of magnitude greater sensitivity by using streptavidin in place of avidin. In these techniques, the primary antibody (which may be monoclonal or polyclonal) binds directly with the specific antigen in or on the cells to form a stable antigen-antibody complex within the tissue section. A secondary antibody that has been labeled with biotin (biotinylated) binds to the primary antibody, leaving the biotinylated end available. A peroxidase or alkaline phosphatase detection system can be used. In a peroxidase method, the biotinylated complex is detected by avidin or streptavidin that has been conjugated to the peroxidase enzyme. A peroxidase-oriented chromogen is then added, such as diaminobenzidine (yielding a brown color) or aminoethylcarbazole (red color, and therefore useful for pigmented lesions).

Avidin-Biotin-Peroxidase Complex and Streptavidin Peroxidase or Alkaline Phosphatase Techniques The alkaline phosphatase-streptavidin method is analogous to the streptavidin-peroxidase method, but in this case the biotinylated complex is detected with an alkaline phosphataselinked streptavidin, and requires a compatible chromogen such as the indole reagents INT/BCIP (red color), naphthol fast red (red), or NBT/BCIP (blue). Caution should be taken not to make a diagnosis based on immunohistochemistry alone. Unfortunately, there is no antibody that distinguishes between benign and malignant cells.
")
APPLICATIONS OF IMMUNOHISTOPATHOLOGY Diagnosis of Tumors (Excluding Lymphomas)


Antibodies Against Cytoskeletal Antigens The cytoskeleton of a cell consists of intermediate filaments measuring 7 to 11 nm in diameter, actin-containing microfilaments, and tubulincontaining microtubules. Intermediate filaments are smaller than microtubules (25 nm) but larger than microfilaments (6 nm); hence, the designation intermediate. Antibodies against intermediate filaments (IFs) help to identify the origin of an anaplastic cell. Malignant tumors usually retain the intermediate filament-type characteristic of the tissue of origin, and metastases generally continue to express these intermediate filaments. There are six groups of intermediate filaments. Types 1 and 2 IFs include cytokeratins, which are present in epithelia. Type 3 IFs include vimentin, found in mesenchymal cells; melanocytes, desmin found in most muscle cells; and GFAP (glial fibrillary acidic protein) found in glial cells and astrocytes. Type IV IFs include neurofilaments that are components of neurons. Nuclear lamins constitute type V IFs, while nestin comprises the type 6, and is found in some stem cells. In dermatopathology, keratin antibodies are used to differentiate epithelial from nonepithelial (melanocytic, hematopoietic, and mesenchymal) tumors.

Antibodies Against Cytoskeletal Antigens A mixture of antibodies against low and intermediate keratins such as AE 1 and AE 3 (AE 1/3) is commonly used. An additional antibody to low molecular-weight keratins such as CAM 5. 2 may be beneficial in poorly differentiated carcinomas. The keratin marker CK 20 has useful specificity for Merkelcell carcinoma. Atypical spindle cell tumors, for example, are often difficult to diagnose with routine stains. The differential diagnosis for such lesions includes spindle-cell, squamous-cell carcinoma, atypical fibroxanthoma, leiomyosarcoma, and spindle-cell malignant melanoma.


Vimentin is an intermediate filament originally isolated from chick embryo fibroblasts. It is found in fibroblasts, endothelial cells, macrophages, melanocytes, lymphocytes, and smooth muscle cells. Antibodies to vimentin are found in both benign and malignant counterparts of these cells. There have also been reports of positivity in epithelial tumors; however, normal epidermis is negative for this antibody. Because of the nonspecific nature of the antibody, it is useful only as a panel approach to support mesenchymal or melanocytic differentiation.
 has been found in normal")
Carcinoembryonic Antigen and Epithelial Membrane Antigen Carcinoembryonic antigen (CEA) has been found in normal eccrine and apocrine cells, in benign sweat gland tumors, and in mammary and extramammary Paget's disease of the skin Incubation with anti-CEA can be helpful in distinguishing Paget cells from atypical melanocytes in melanoma in situ However, reactivity of melanomas with CEA has been reported. Carcinoembryonic antigen typically stains adenocarcinomas from most organ systems. Most epithelial tumors react with antibodies against epithelial membrane antigen (EMA), including squamous cell carcinoma, breast carcinoma, and large-cell lung carcinoma. EMA will also stain normal sweat and sebaceous glands, although epidermis is unreactive with this antibody. Epithelioid sarcoma is also stained by EMA.
 is an acidic enzyme found in neuroendocrine cells, neurons,")
Neuron-Specific Enolase Neuron-specific enolase (NSE) is an acidic enzyme found in neuroendocrine cells, neurons, and tumors derived from them. Merkel-cell carcinoma contains NSE; however, NSE can be detected in a variety of other tumors, including malignant melanoma, and therefore has low specificity. The keratin marker CK 20 has better specificity for Merkel-cell tumors than for melanoma and other neuroendocrine tumors.

Chromogranin The soluble proteins of chromaffin granules are called chromogranin. Chromogranins consist of three families of acidic proteins: chromogranin A, B, and C. They are normally found in most endocrine cells (e. g. , thyroid, parathyroid, anterior pituitary). In the skin, chromogranin A has been found in Merkel-cell carcinoma. In contrast, nevi and melanoma do not contain chromogranin.

Synaptophysin is a 38 -k. D glycoprotein that participates in calcium-dependent release of neurotransmitters. It is a neuroendocrine antigen with a distribution similar to chromogranin. Positive staining with antibodies to synaptophysin is useful in the diagnosis of neuroendocrine tumors such as Merkel-cell carcinoma. Interestingly, normal Merkel cells are negative for this antibody. Similar to chromogranin, melanocytic tumors do not stain with synaptophysin.

S-100 Protein S-100 protein is an acidic protein that binds Ca 2+ and Zn 2+. It was called S-100 because of its solubility in 100% ammonium sulfate at neutral p. H. It is found in the cytoplasm and in the nucleus. S-100 protein can be detected in a large variety of cells: melanocytes, Langerhans cells, eccrine and apocrine gland cells, nerves, muscles, Schwann cells, myoepithelial cells, chondrocytes, and their malignant counterparts. Histiocytes may also stain positively with S-100 protein. Its high sensitivity contrasts with a low specificity, a feature that supports the concept of a panel approach to immunohistochemistry. Useful applications of the antibody against S-100 protein include (a) diagnosing of spindle-cell melanoma and desmoplastic melanoma; (b) distinguishing between melanocytes and lymphocytes in halo nevi; (c) differentiating between pigmented actinic keratoses and lentigo maligna; and (d) diagnosing poorly differentiated cutaneous metastases.

HMB-45 is a monoclonal antibody that was initially generated from an extract of metastatic melanoma. Both primary and metastatic melanomas reveal cytoplasmic staining with HMB 45; spindle-cell melanomas and desmoplastic melanomas are frequently negative. This antibody reacts with a melanosomal protein, GP-100, which tends to be expressed in immature or proliferating cells. Unfortunately, HMB-45 may react with melanocytes in nevi, including dysplastic nevi and Spitz nevi. Therefore, it should not be used for the differential diagnosis between a malignant melanoma and a benign nevus. Most desmosplastic melanomas as well as some metastatic melanomas may show negative staining with HMB-45.

Thanks for your attention
 is a relatively new melanocytic differentiation")
MART-1/Melan-A Melanoma antigen recognized by T cells (MART-1) is a relatively new melanocytic differentiation marker. The antigen is expressed in : 1)normal melanocytes 2)common nevi 3)Spitz nevi 4)malignant melanoma
 neurotized nevi 2)desmoplastic melanomas In the skin,")
Negative staining is frequently seen in: 1) neurotized nevi 2)desmoplastic melanomas In the skin, Melan-A m. RNA has only been found: 1)melanocytic lesions 2)angiomyolipomas This antibody is a useful addition when evaluating intraepidermal melanocytes 1)Vitiligo 2)early melanoma in situ), as well as amelanotic melanomas.

CD 34 Both benign and malignant vascular tumors express this antigen. In dermatopathology CD 34 positivity in dermatofibrosarcoma protuberans is useful in differentiating these lesions from dermatofibromas, which are CD 34 negative and factor XIIIa positive.
solitary fibrous tumor 2)giant cell fibroblastoma")
Other cutaneous neoplasms that express CD 34 include 1)solitary fibrous tumor 2)giant cell fibroblastoma 3)Neurofibroma 4)epithelioid sarcoma 5)spindle cell lipoma 6)sclerotic fibroma 7) fibrous papule of the nose.
 is a large glycoprotein produced")
Factor. Vlll-Related Antigen Factor Vlll-related antigen (von Willebrand factor) is a large glycoprotein produced by endothelial cells and therefore useful in benign and malignant vascular neoplasms.
50% of hemangiomas 2)5% to")
some studies have demonstrated factor VIII positivity in only 1)50% of hemangiomas 2)5% to 25% of malignant endothelial tumors.

CD 31 This 130 -k. D glycoprotein, whose major function is to mediate platelet adhesion in vascular endothelial cells, is also known as platelet endothelial cell adhesion molecule (PECAM).

CD 31 is a sensitive marker for vascular tumors except Kaposi's sarcoma. It is a more sensitive marker for cutaneous angiosarcoma than factor VIII-related antigen.

Factor Xllla It is a blood coagulation factor, is responsible for stabilizing newly formed clots by cross linking fibrin. Also present in 1)fibroblast-like mesenchymal cells 2) dermal dendrocytes 3)platelets 4)Megakaryocytes 5) peritoneal and alveolar macrophages 6)normal adipose tissue 7)Monocytes 8)placenta 9) Uterine 10) Prostate tissue.

As noted earlier, using factor XIIIa in combination with CD 34 can be helpful in differentiating dermatofibroma from dermatofibrosarcoma protuberans this factor is positive in 1)fibrous papule 2)atypical fibroxanthoma 3)xanthogranuloma 4)atypical cells in radiation dermatitis 5)Multinuclate cell angiohistocytoma 6)Epithelioid cell histiocytoma

Antibodies Against Lysozym; a 1 -Antitrypsin a 1 -Antichymotrypsin These antibodies have been regarded as markers of mononuclear phagocytic cells. Although once felt to be markers for fibrohistiocytic neoplasms, they have also been identified in 1)Carcinomas 2) Melanomas making them less specific.
 CD 117 is present on a number of cell types, including:")
c-kit (CD 117) CD 117 is present on a number of cell types, including: 1)mast cells 2)melanocytes 3)hematopoietic stem cells 4)immature myeloid cells 5)myeloid and lymphoid progenitors 6)germ cell lineages and it plays a crucial role in their activation and growth.

Constitutively activec -kit has been implicated in the pathogenesis of a number of disorders including 1)systemic mastocytosis 2)gastrointestinal stromal tumors Increased c- kit expression has been seen on malignant cells from many acute myeloid leukemia subtypes and chronic myelogenous leukemia.

in addition, a number of solid tumor cells have been shown to express high-affinity c-kit receptors, including 1)Breast 2)Lung 3)gastric carcinoma as well as some melanomase, specially of the 1)acral 2)lentigo maligna 3) Ocular subtypes.

CD 1 a Like other members of the CD 1 family, CD 1 a functions to mediate the presentation of lipid and glycolipid antigens to T cells. In pathology, CD 1 a has become a marker of 1)Langerhans cells 2) blood monocyte-derived dendritic cells.

As a diagnostic tool, it has been used together with S 100 to define dendritic cell populations as well as for the diagnosis of: *Langerhans cell histiocytosis (histiocytosis X).
 This antibody helps to distinguish between undifferentiated Iymphomas")
Antibodis Against leukocyte common Antigen(CD 45) This antibody helps to distinguish between undifferentiated Iymphomas and carcinomas. Leukocyte common antigen (LCA) is found on all leukocytes, including 1)Granulocytes 2)lymphocytes 3)monocytes 4) Macrophages 5) mast cells 6)Langerhans

The lymphomas and leukemias react with the antibody against LCA; carcinomas and melanomas are negative. In addition to LCA, lysozyme and chloroacetate Esrerase aid in the diagnosis of leukemia cutis.

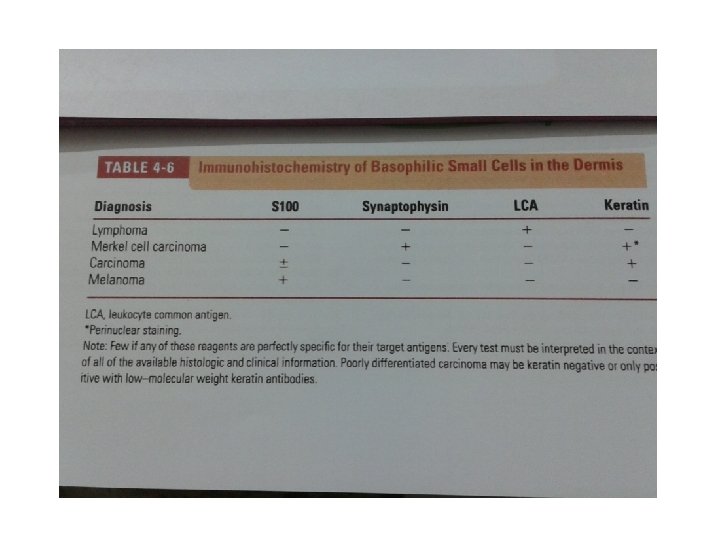
LCA is particularly useful in the evaluation of tumors composed of small atypical basophilic cells in the dermis.

Diagnosis of Lymphomas The application of monoclonal antibodies for the diagnosis of lymphomas is expanding. However, there is no antibody that distinguishes between benign and malignant lymphocytes. Hence, the difficult distinction between lymphoma and pseudolymphoma remains.
helper or")
Monoclonal antibodies can determine the cell types in a lymphoma or pseudolymphoma: 1)helper or suppressor T cells 2)B cells 3)plasma cells 4)macrophages.

confusing issue is that B-cell lymphomas may contain reactive T-cell infiltrates, which can outnumber B cells. The predominance of a T-helper lymphocytic infiltrate with epidermotropism of the Thelper subtype is highly suggestive of cutaneous T-cell lymphoma.

In contrast, a mixture of T-helper and Tsuppressor phenotypes is most consistent with a reactive profile (e. g. , spongiotic dermatitis). In dense nodular infiltrates, the presence of germinal center formation with B -lymphocyte aggregates surrounded by a mantle of T cells favors lymphocytoma cutis over lymphoma.

Electron Microscopy Transmission electron microscopy may be beneficial in the diagnosis of poorly differentiated skin neoplasms for which immunohistochemistry is negative.
intercellular junctions (epithelial tumors) 2)melanosomes (melanocytic tumors) 3)")
Using electron microscopy, the identification of 1)intercellular junctions (epithelial tumors) 2)melanosomes (melanocytic tumors) 3) Weibel-Palade bodies (endothelial cells) can provide an important diagnostic aid.

Other uses of diagnostic electron microscopy include the subtype determination of *epidermolysis bullosa And the diagnosis of metabolic storage diseases 1) eg , Fabry disease 2)amyloidosis.
- Slides: 99