Laboratory Investigations Prognosis and Treatment Plan Laboratory Investigations

Laboratory Investigations, Prognosis and Treatment Plan

Laboratory Investigations

Laboratory Investigations Laboratory Aids to Clinical Diagnosis: • Radiographs • Blood tests
: • Designed for easier and")
• The Periodontal Screening and Recording System (PSR): • Designed for easier and faster screening and recording of the periodontal status of a patient Instrument: • Specially designed probe that has a 0. 5 mm ball tip and is color coded from 3. 5 – 5. 5 mm

Procedure: • Patient’s mouth is divided into 6 sextants • Each tooth is probed on 6 surfaces – mesiofacial, midfacial, distofacial, mesiopalatal, mid palatal, distopalatal • Deepest finding is recorded Maxillary right Mandibular right Maxillary anteriors Mandibular anteriors Maxillary left Mandibular left

Code Criteria Code 0 Probe’s colored band is completely visible Gingival tissue is healthy No BOP No calculus or defective margins Patient’s require only preventive care Code 1 Probe’s colored band is completely visible BOP present No calculus or defective margins Patient’s require subgingival plaque removal & oral hygiene instruction Code 2 Probe’s colored band is completely visible BOP present Calculus or defective margins are found Patient’s require calculus removal correction of plaque retentive margins of restorations & oral hygiene instruction

Code Criteria Code 3 Probe’s colored band is partially submerged BOP present Calculus or defective margins are found Patient’s require a comprehensive full – mouth periodontal examination, charting is indicated Code 4 Probe’s colored band is completely submerged (> 5. 5 mm) BOP present Calculus or defective margins are found Patient’s require a comprehensive full – mouth periodontal examination, charting & treatment planning is indicated Code * The code number in addition to Abnormalities like - furcation involvement, mobility, mucogingival problem, gingival recession

The code finding for each sextant & the date are entered on a sticker, which is placed on the patient’s record

Prognosis

Prognosis Ø Prognosis is a prediction of the probable course, duration and outcome of a disease based on the knowledge of the pathogenesis of the disease and presence of risk factors. Ø It is established after a diagnosis is made Ø Based on information about disease , physicians knowledge , previous experience

Types of Prognosis Ø Excellent Ø Good Ø Fair Ø Poor Ø Questionable Ø Hopeless

Type of Prognosis Criteria Excellent No bone loss Excellent gingival condition Good patient cooperation No systemic or environmental factors Good Adequate bone remaining Adequate possibility to control etiologic factors Adequate patient cooperation No systemic or environmental factors ( if present well controlled) Fair Less than adequate bone remaining Some tooth mobility Grade 1 furcation involvement Adequate maintenance possible Acceptable patient cooperation Presence of limited systemic or environmental factors

Type of Prognosis Criteria Poor Moderate to advanced bone loss Tooth mobility Grade 1 &2 furcation involvement Difficult to maintain areas Doubtful patient cooperation Presence of systemic or environmental factors Questionable Advanced bone loss Tooth mobility Grade 2 & 3 furcation involvement Inaccessible areas Presence of systemic or environmental factors Hopeless Advanced bone loss Severe tooth mobility Grade 2 & 3 furcation involvement Non maintainable areas Extractions indicated Presence of uncontrolled systemic or environmental factors

Types of Prognosis • Overall Prognosis - concerned with the dentition as a whole • Individual Prognosis - concerned with the individual teeth

Factors in Determining Prognosis

Relationship between Diagnosis and Prognosis • Factors such as – patient age severity of disease genetic susceptibility presence of systemic disease Important criteria in the diagnosis of the condition These are important in developing a prognosis

Prognosis for patients with Gingival Disease • Dental plaque induced Gingival Disease • Non plaque induced Gingival Disease Dental plaque induced Gingival Disease • Gingivitis associated with Dental plaque only: - Reversible - Plaque removal Prognosis: Good

• Plaque induced Gingival Disease modified by Systemic factors: - Inflammatory response to bacterial plaque - Influenced by systemic factors Prognosis: Long term prognosis depends not only on control of bacterial plaque but also on control of the systemic factors

• Plaque induced Gingival Disease modified by Medication: – – Drug induced gingival enlargement Oral contraceptive associated gingivitis Plaque control alone is not sufficient Surgical intervention required Prognosis: Long term prognosis depends on whether the patient’s systemic problem can be treated with an alternative medication that does not cause gingival enlargement

• Gingival Disease modified by Malnutrition: - Vitamin C deficiency Prognosis: The prognosis depends on the severity and duration of the deficiency and on the likelihood of reversing the deficiency through dietary supplementation

• Non plaque induced Gingival Disease: - Seen in bacterial , fungal, and viral infections Prognosis: Prognosis for these patients depends on the elimination of the causative agent

Prognosis for patients with Periodontal Disease • Chronic Periodontitis: - slow progressing Prognosis: Slight to moderate periodontitis – Good Severe disease – Fair to poor prognosis

• Aggressive Periodontitis: - Rapid attachment loss & bone destruction - Familial aggregation - Use of systemic antibiotics is a must Prognosis: Early – Good Advanced – Fair, Poor, Questionable

• Periodontal Disease as a manifestation of Systemic condition: - These disorders manifest early in life - The impact on the periodontium is similar to Ag. P Prognosis: Fair to Poor

• Necrotizing Periodontal Disease – - ANUG - NUP Prognosis: ANUG – Fair NUP – depends on the systemic condition of patient

Revaluation of Prognosis after Phase 1 Therapy • Reduction in pocket depth & inflammation – Favorable prognosis • Inflammation uncontrolled – Unfavorable prognosis • Progression of periodontitis occurs in episodic manner • Advanced , active lesions - progress rapidly to hopeless stage

Treatment Plan

Treatment Plan After the diagnosis and prognosis have been established The treatment is planned The treatment plan is the blueprint for case management It includes all procedures required for the establishment & maintenance of Oral Hygiene

It includes procedures like - ØDecisions to teeth to be retained or extracted Ø Decisions on techniques to be used for pocket therapy Ø The need for Mucogingival Surgery / Reconstructive surgery Ø The need for occlusal correction Ø The need for temporary or final restorations Ø The need for orthodontic consultation ØEndodontic therapy

The Master Plan for Total Treatment Ø The primary goal is elimination of gingival inflammation and correction of the conditions that cause or perpetuate it Ø It is important to establish and maintain the health of the periodntium throughout the mouth rather than to tighten loose teeth Ø The periodontal condition of the teeth to be retained is more important than the number of such loose teeth
 Phase I therapy ( Etiotropic")
Sequence of Treatment Plan Preliminary phase ( Emergency Phase) Phase I therapy ( Etiotropic Phase) - Scaling and root planing Phase II therapy ( Surgical Phase) - Periodontal surgery - R. C. T. Phase III therapy ( Restorative Phase ) - Final restorations - Fixed prosthesis Phase IV therapy ( Maintenance Phase ) - Periodic recalls
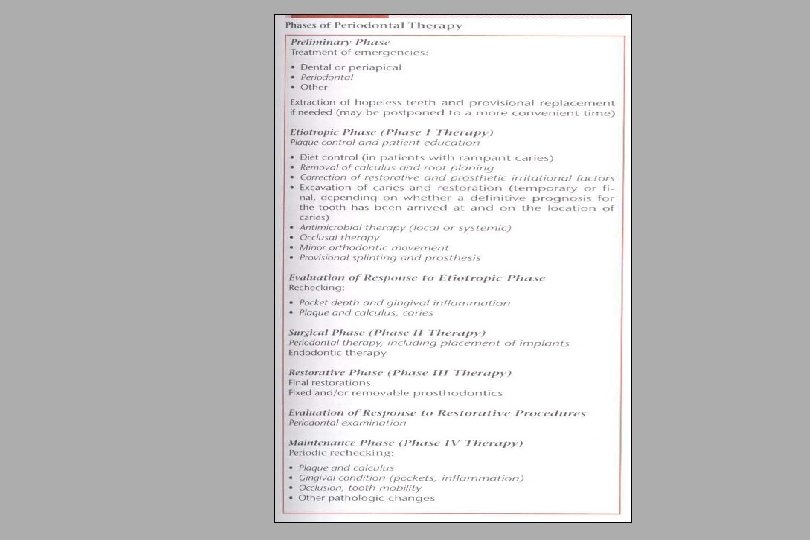

Preferred Sequence of Periodontal Therapy

Thank You
- Slides: 34