Laboratory diagnostic of STDs Clinical aspects of BV

Laboratory diagnostic of STDs








Clinical aspects of BV www. usc. edu/. . . /adolhealth/content/b 3 stis 3. html

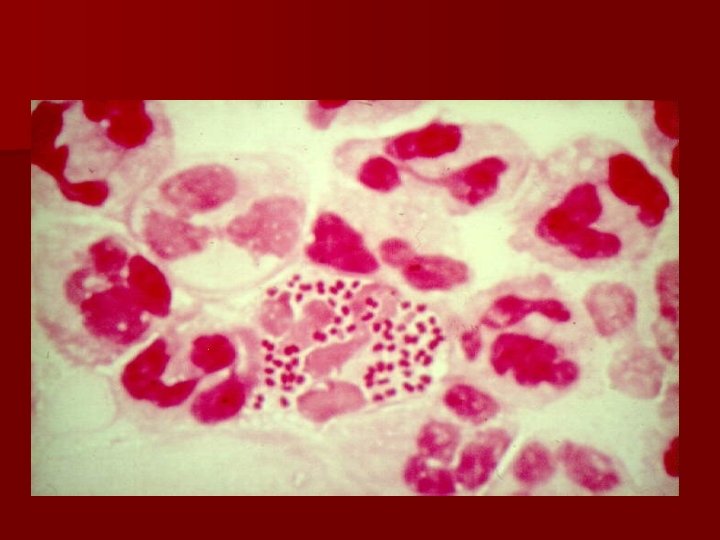
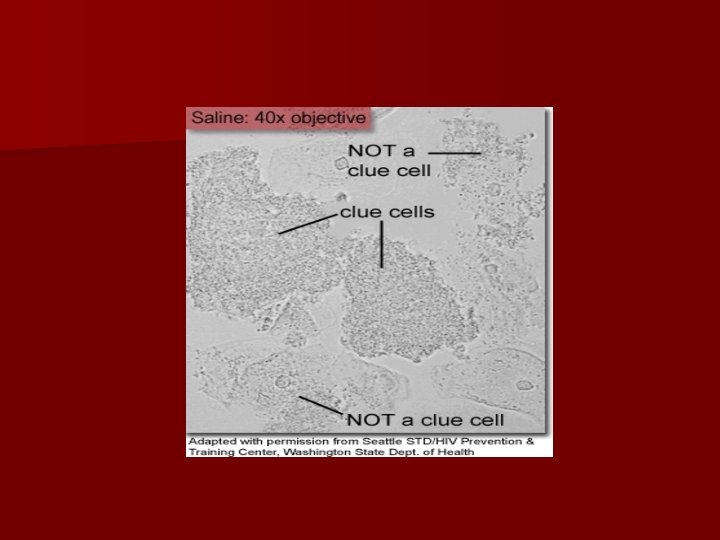
Clue cells

Gardnerella vaginalis - Clue Cells Pap Smear X 10 imagecache 6. allposters. com/. . . /3040/EDPBF 00 Z. jpg

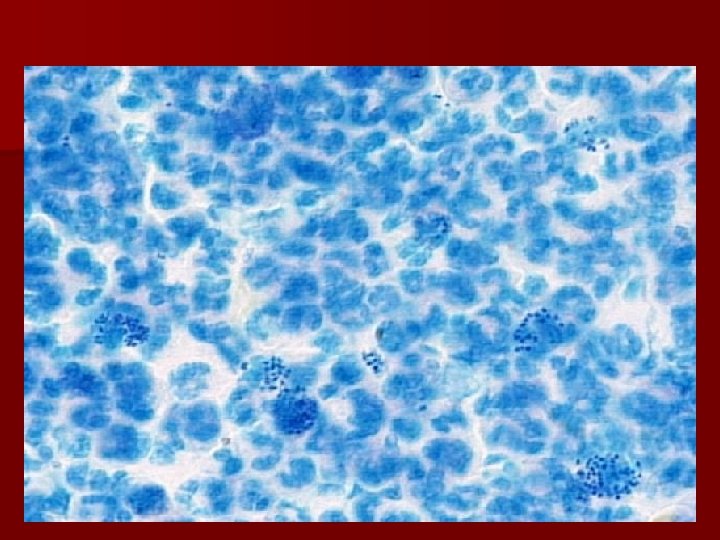
Normal vaginal flora A: 4+ morfotipuri lactobacili, fara bacterii gram negative – scor 0; B: 3+ morfotipuri lactobacili, 1+ Garnerella spp – scor 2; Nugent RP, Krohn MA, Hillier SL (1991). "Reliability of diagnosing bacterial vaginosis is improved by a standardized method of gram stain interpretation ”

BV E: lactobacili absenti, 4+ bacili gram negativi; prezente “clue cells” – scor 8; F: lactobacili absenti, 4+ bacili gram negativi; prezente “clue cells” si Mobiluncus spp. – scor 10. Nugent RP, Krohn MA, Hillier SL (1991). "Reliability of diagnosing bacterial vaginosis is improved by a standardized method of gram stain interpretation ”


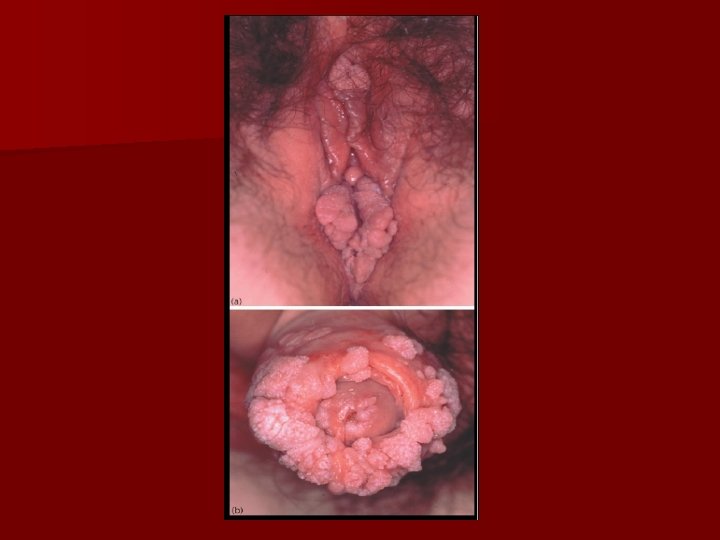
• • Figure A – a patient with exophytic genital condyloma acuminatum Figure B – the initial form of Buschke Lowenstein tumor Figure C – verrucous carcinoma Figure D – perianal Buschke Lowenstein tumor


STD: normal flora and causative agents Anatomic site Normal flora Distal urethra Enterobacteriaceae, alpha streptococci, enterococci, coagulase negative staphylococci, anaerobs Chlamydia trachomatis Neisseria gonorrhoeae Mycoplasma genitalium Ureaplasma urealyticum Extern genital organs coagulase negative staphylococci, diphtherimorf, yeasts, Enterobacteriaceae HSV, HPV, Treponema pallidum, Haemoplilus ducrey, C. trachomatis, Candidas pp. Vagina Lactobacillus, Enterobacteriaceae, alpha streptococci, enterococci, coagulase negative staphylococci HPV, Trichomonas vaginalis STDs Causative agents non STDs HSV type 1, Candida spp, S. pyogenes Candida, Trichomonas vaginalis.

Anatomic site Normal flora STDs Cervix Endometrium, Fallopian tube, ovary Normal sterile Causative agents non STDs HPV, HSV type 1, CMV N. gonorrhoeae, C. trachomatis Mixt ascending infections, S. pyogenes, L. monocytogenes, B group streptococci, Actinomyces israelii

Diseases: Urethritis: - N. gonorrhoeae - non gonococcal – C. trachomatis - Ureaplasma urealyticum - Mycoplasma genitalium - Trichomonas vaginalis - HSV type 2 - post gonococcal – re infection - failure treatment - double infection ( C. trachomatis, U. urealyticum has longer incubation than gonococcal infection) Vulva infection : – T. pallidum - HSV, 1 - HPV (6, 11) - Sarcoptes scabiei

Vaginitis – vaginal discharge - specific – Candida albicans - T. vaginalis Vaginosis - Gardnerella vaginalis, Bacteroides, Peptococcus, - Mobiluncus, Mycoplasma hominis girls – vulva - vaginitis – N. gonorrhoeae - C. trachomatis - S. pyogenes Cervicitis – T. vaginalis - Candida albicans - Treponema pallidum - Papillomavirus - N. gonorrhoeae - HSV, 2

Laboratory diagnostic Sampling and transport of the pathologic products - Urethral discharge: - at least 2 hours after micturition - Spontaneous / swab - Smears (3), culture – preferable - Vaginal discharge: through aspiration /swab - Endocervicitis: the cervix is scrape with 2 – 3 sterile compress, and then sampling of 3 swabs – gram staining, culture, Giemsa.

- genital ulcers: swab syphilis – dark field examination - fluorescent antibody examination Herpes ulcers: - Giemsa, Papanicolau smear for giant cells. IF for viral antigens in epithelial cell. - serology: syphilis confirmation, C. trachomatis - genital warts – biopsy – genotyping HPV

Case 1 Man, 22 years old, after a holiday in Turkey, present dysuria and purulent urethral discharge. Presumptive diagnostic: gonococci urethritis Sampling: urethral discharge, 3 smears, cultivation, ELISA for Chlamydia Diagnosis: gonococcal urethritis Treatament : - First intention… What do you prescribe to the patient?

Case 2 Professional driver request a medical examination for legs pain, walking difficulty. History: painless penille lesion which cured spontaneous, without treatment. Probably diagnosis: tertiary syplilis Laboratory findings: serum – VDRL positive (titer 512), TPHA positive, FTA-abs positive. CSF – VDRL positive (titru 512), TPHA şi FTA-abs – positive. Therapeutic behavior: - Hospitalization - Penicilin, - Repeat the serologic tests and lumbar puncture after 3 – 6 month.

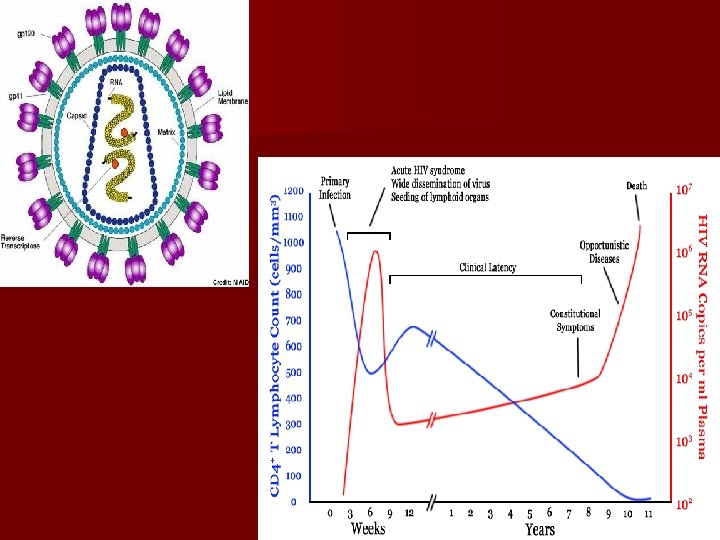
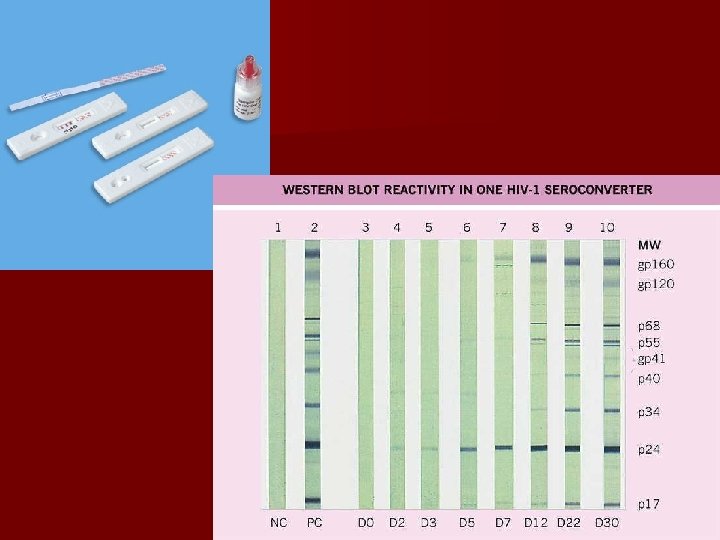
Case 3 New – born, caesarian section; the mother is HIV positive since 4 years ago. The gynecologist found about the history of the patient after delivery; the mother came at the hospital in the last moment. Laboratory findings: child - antibody anti HIV type Ig. G (ELISA, Western-blot). After 4 month: the child doesn’t grow, present oral candidiasis, generalized lymphadenopathy, persistent diarrhea. ARN / HIV is present in the blood. Diagnostic – AIDS. Treatment: anti retroviral – after some month the symptomatology disappeared.

Case 4 Man, 25 years old, detect on a wart lesion on the penis, before 4 month ago. Quickly after, his wife present genital warts, also. The dermatologyst confirm the diagnostic. Advise the women to perform a gynecologic exam. Questions: - When and how was the husband contaminated? - Is the wife infected? What are the clinical consequences? - How can the diagnosis be confirmed ?
- Slides: 32