LABORATORY DIAGNOSIS OF SYPHILIS Lab diagnosis is essential

LABORATORY DIAGNOSIS OF SYPHILIS •

• Lab diagnosis is essential because of the asymptomatic phase in the disease. • And also to asses the cure after treatment. o IT is done mainly by demonstration of • Spirochetes under microscope • Antibodies in serum or CSF

MICROSCOPY • Specimens collected –infectious. so care required PROCEDURE: • Lesion first cleaned with gauze soaked in warm saline & margins-gently scraped so that superficial epithelium is abraded. • Gentle pressure applied at base of lesion & serum that exudes is collected • Wet mount is prepared & observed under DARK GROUND MICROSCOPE

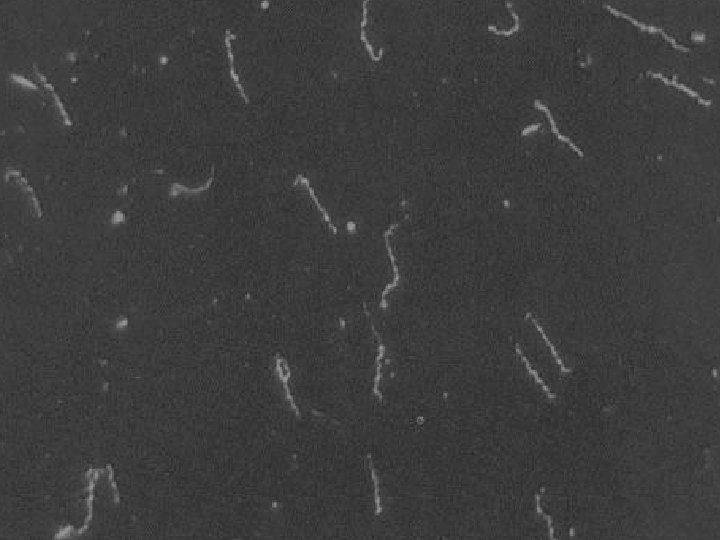
SLENDER SPIRALS


CONTD. . • Treponema pallidum is identified by its slender SPIRAL structure with spiral ends & pointed ends. IMPORTANCE: • Useful in primary , secondary and congenital syphilis. NOTE: Negative results don’t exclude diagnosis of syphilis because of its low sensitivity.

CONTD. . DFA-TP: • Direct fluorescent antibody test-better & safe for diagnosis. • Smears fixed with acetone & sent to laboratory • Requires fluorescent tagged anti –Treponemal antiserum. • More reliable-Specific monoclonal antibody


SEROLOGICAL TESTS • The serological tests that are in practice are: ü Standard test for Syphilis – test for antibodies reacting with cardiolipin antigen. ü Tests for antibodies reacting with group specific Treponemal antigen ü Tests for specific antibodies to pathogenic Treponema
 LIPOIDAL antigen ü ü ü Wassermann")
REAGIN ANTIBOBY TESTS • Antigen – CARDIOLIPIN (or) LIPOIDAL antigen ü ü ü Wassermann complement fixation test(1906) Modificated method by PANGBORN(1945) Tube flocculation test of KAHN Venereal disease research laboratory test(VDRL) Rapid plasma reagin test(RPR)

VDRL TEST • Slide flocculation test • Term-REAGIN • Principle: patients suffering from syphilis produce antibodies that react with antigen CARDIOLIPIN to produce flocculation that is read by microscope.

• Requirements: ü VDRL antigen ü VDRL diluant ü VDRL slide ü Microscope ü Micropipette 16 guage syringe ü Water bath ü Tips

• VDRL antigen: alcoholic solution of composed of 0. 03% cardiolipin, 0. 21% lecithin, 0. 9% cholesterol. • VDRL slide: glass slide having eight depressions.


SAMPLE PREPARATION: • serum is separated from patient’s blood that is collected & is inactivated. • Sample is allowed to reach room temperature. ANTIGEN PREPARATION: • 4. 5 ml VDRL diluant is taken & added to vial drop by thorough mixing. • Use limited to 18 -24 hours.

Procedure: • VDRL slide is taken. To test well, serum sample is added. (0. 05 ml) • Positive & negative controls added to their respective wells. (50 micro. L) • With the help of 16 guage syringe, 1 ml of prepared antigen is added to all wells drop by drop

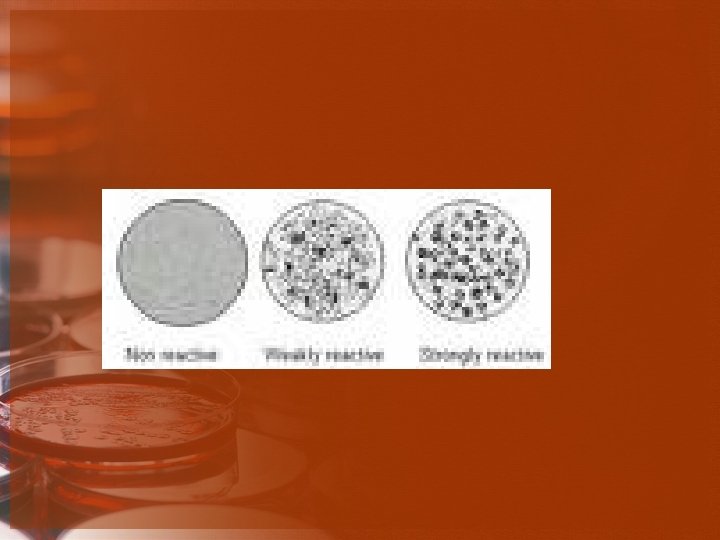
• Antigen & specimen mixed thoroughly using separate tips. • Now, slide is placed on VDRL rotator & rotated for 4 min, observed under microscope • Negative & positive controls are observed first to verify the quality of antigen. • No flocculation -negative test well • Flocculation – positive well

• If flocculation is observed, screening test is considered REACTIVE. accordingly, it is termed reactive, weakly reative & non-reactive. • further confirmed by semiquantitative assay • To say it reactive, minimum of 1/8 titre is required. • Non-reactive- less than 1/2 titre.

CONTD. . RPR test : Advantages: NOTE: CSF is not recommended testing with the help of this method • Antigen – VDRL antigen with fine CARBON particles • Evident to naked eye • Time accessible since serum collected does not require heating

CONTD. . RPR test : • Antigen – VDRL antigen with fine CARBON particles Advantages: • Evident to naked eye • Time accessible since serum collected does not require heating NOTE: CSF is not recommended testing with the help of this method

CONTD… Automated RPR • For large scales Automated VDRL-ELISA test • To measure Ig. M & Ig. G separately & suitable for large scales

CONTD… • BFP TESTS: biological false positive • Reason : cardiolipin is present in mammalian tissue too • Positive in about 1% individuals

CONTD… BFP REACTIONS: • Acute-only for few weeks or months Ø Due to acute infections, injuries, inflammation • Chronic-greater than 6 months Ø Seen in SLE, leprosy, malaria, relapsing fever, infectious mononucleosis, hepatitis, tropical eosinophilia

CONTD… REAGIN ANTIBODY : detectable 7 -10 days after appearance of primary chancre sensitivity titre Primary stage. Low-8 60. 75% Secondary stage High-16 to 128 or -100% more

CONTD… • Reagin tests are preferred mostly because they become negative on treatment.

GROUP SPECIFIC TREPONEMAL TESTS • Tests using cultivable treponemes as antigen ü Reiter protein complement fixation test Ø Antigen-lipopolysaccharide protein complex derived from treponeme Ø Sensitivity & specificity-low
- Slides: 29